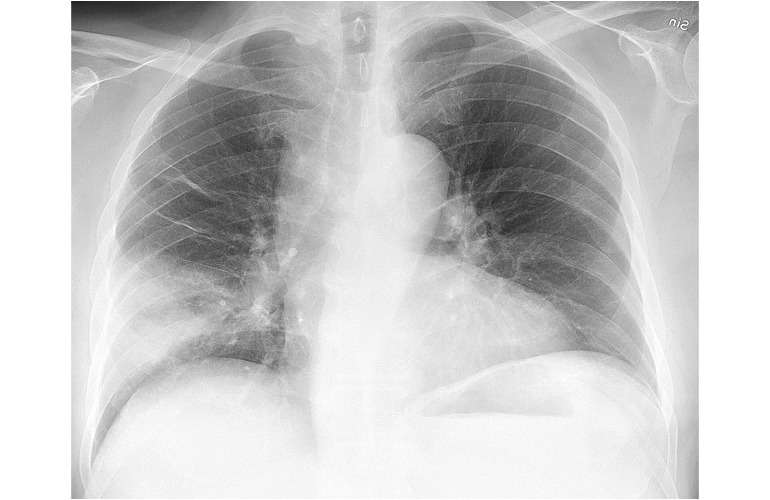
Diagnosing pulmonary tuberculosis can be a tricky thing. As highlighted previously, the Ziehl-Neelsen smear is not a terribly sensitive methodology and the MTB-PCR sensitivity depends on if the sample is smear positive. Given that pulmonary tuberculosis tends to have a higher bacterial burden, it would be reasonable to think that other diseases without this high