
Procalcitonin is a precursor of the hormone calcitonin and is released into systemic circulation within 4 hours of inoculation of bacterial endotoxin, In general, cytokines enhance procalcitonin release while interferons, which are released in context of viral infections. Because of this, there has been a push towards using PCT to differentiate bacterial from viral infections and to guide antibiotic therapy or de-escalation. Most of the data has been on pulmonary infections as there is difficulty in differentiating bacterial and viral etiologies in these cases.
Utility of PCT in Pneumonia
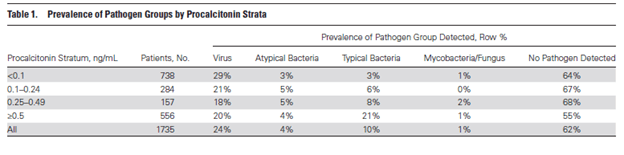
The association of serum PCT concentration with the etiology of pneumonia was evaluated in a prospective multicenter active surveillance study (1). Hospitalized patients with community acquired pneumonia by CXR had their PCT levels measured and the distribution of these were compared between etiologies, including bacterial pneumonia, atypical pneumonia, viral pneumonia, and fungal pneumonia. 1735 patients were evaluated, and patients with typical pneumonia tended to have a higher mean PCT when compared to other etiologies.
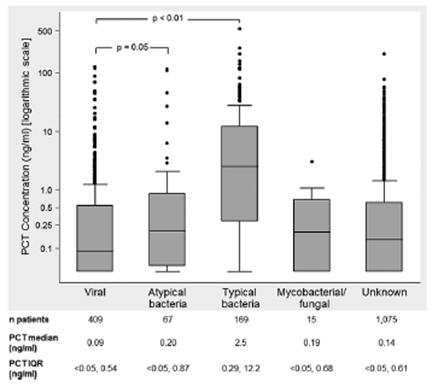
Further, more patients with bacterial pneumonia had a PCT >0.5, however 20% of patients with viral pneumonia also had a PCT >0.5.
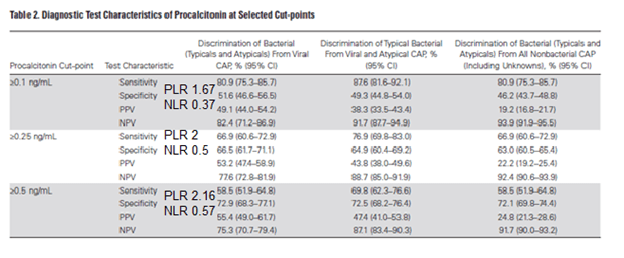
In other words, a cut-off of <0.5 may be useful to rule out bacterial pneumonia but a PCT >0.5 does not necessarily imply a bacterial etiology. Overall, PCT had a decent sensitivity at a cutoff of >0.1 to differentiate bacterial pneumonia from viral pneumonia as well as bacterial vs atypical pneumonia and bacterial vs non-bacterial pneumonia. Sensitivity, predictably, decreased with a higher PCT threshold. At best, it was able to differentiate bacterial pneumonia from non-bacterial pneumonia and a negative PCT had a fairly high NPV:
ROC seems to match up with the above results:
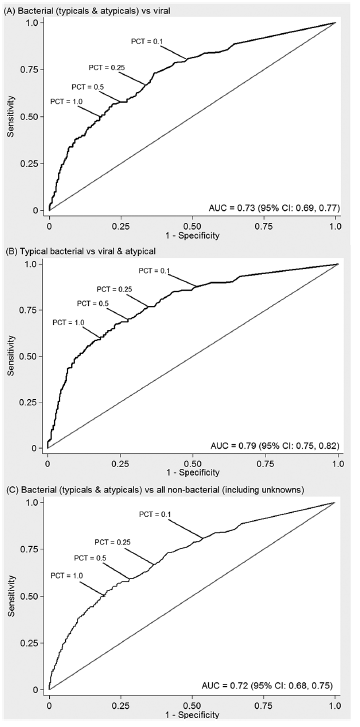
Suggesting that if negative, it is fairly helpful but a positive result is not necessarily all that is cracked up to be.
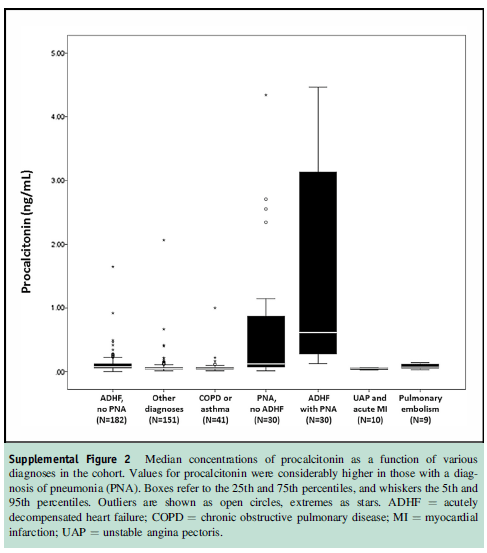
In a prospective study (2), PCT was used to differentiate patients presenting with either pneumonia or heart failure as the cause of dyspnea. 453 patients were evaluated in the cohort, with 212 presenting with acute heart failure, 41 with COPD/Asthma, and 30 presenting with pneumonia. An additional 30 patients with heart failure were also diagnosed with pneumonia. Overall, patients with pneumonia had higher PCT levels when compared to those who had acute heart failure, 0.38 (0.12-1.40) vs 0.06 (0.04-0.09):
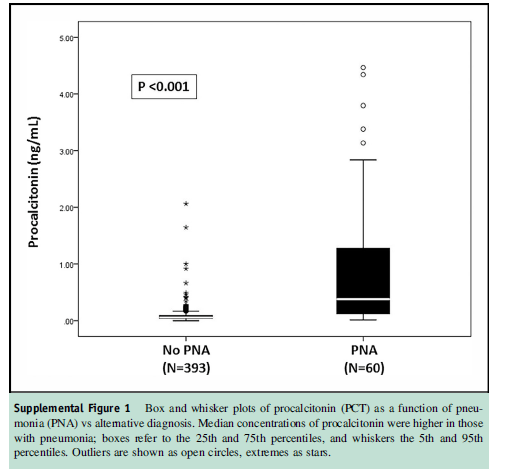
Notably, those with both heart failure and PNA had significantly higher levels than those with PNA alone, 0.62 (0.28-3.2):
Using a PCT threshold of 0.1, the AUC was 0.84 (95% CI 0.77-0.91), with it performing significantly better the higher the pre-test probability of pneumonia was:
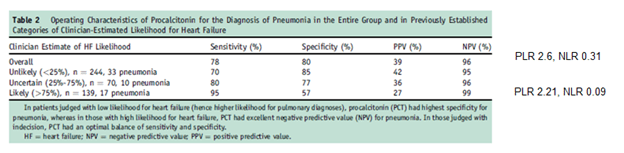
As you can see, the PLR is not terribly great (i.e. PCT is not great to diagnose) but has a good NLR, so a negative study helps in discarding the diagnosis of bacterial pneumonia.
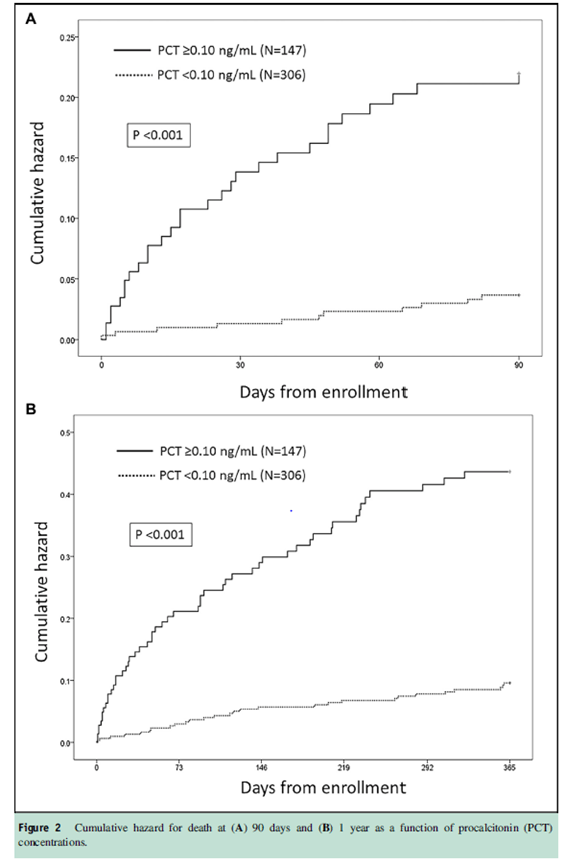
Notably, those with a positive PCT had a higher mortality than those with a negative PCT:
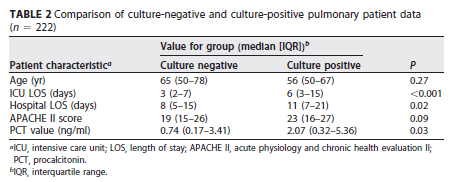
In 2 prospective studies (3) several biomarkers were evaluated in 178 patients with a diagnosis of pneumonia. Overall, both IL-6 and CRP had higher diagnostic accuracy when compared to PCT (IL-6 had AUC = 0.80, 95% CI 0.77-0.85; CRP AUC =0.82, 95% CI 0.79-0.85; PCT AUC =0.75, 95% CI 0.71-0.78). In another retrospective study (4), PCT was able to predict positive cultures for bacteremia better than for respiratory infections:
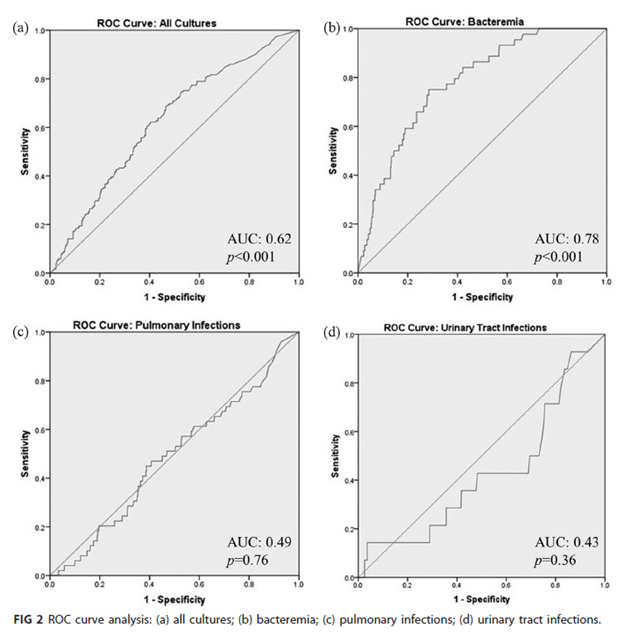
Though those with positive respiratory culture had higher PCT and longer hospital length of stay along with longer ICU stay:
PCT as a De-escalation Tool:
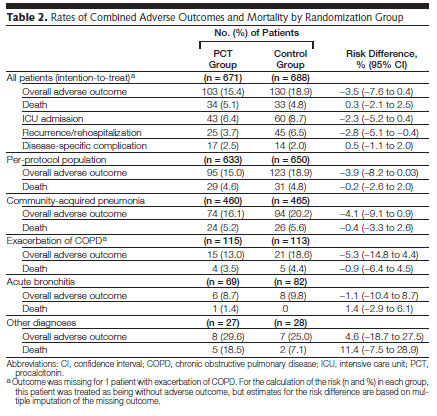
This was evaluated in a large, multicenter RCT from Switzerland (5). PCT was compared to conventional therapy with the primary endpoint being the composite of overall adverse events occurring within 30 days following ED admission (including death from any cause, ICU admission, disease specific complications, and recurrence of disease). 1359 patients were randomized, with 103 patients in the PCT group (15.4%) and 130 patients in the standard group (18.9%) reaching the primary end point, which was not statistically significant. This held true in the per protocol population, as well as across different patients, including CAP, COPD exacerbation, and acute bronchitis:
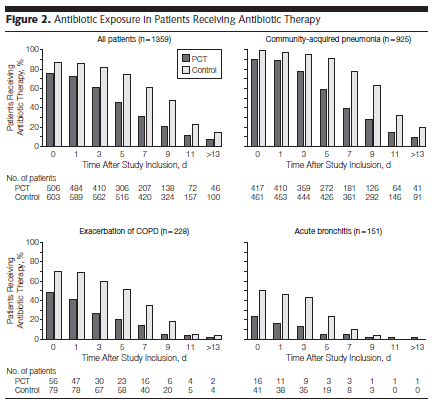
PCT group also had lower antibiotic use:
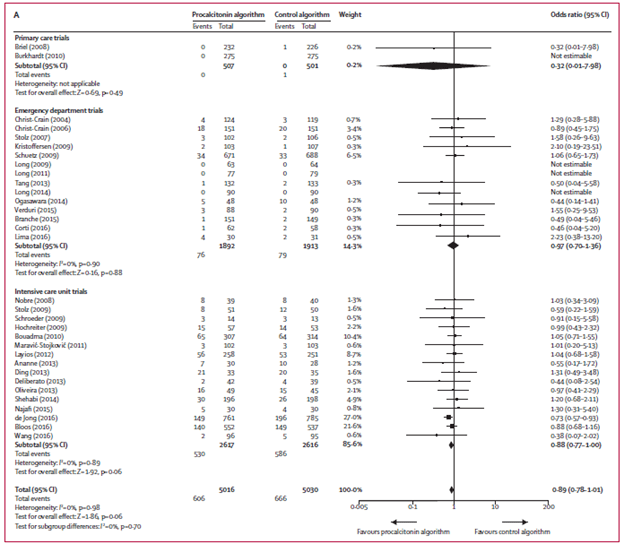
A Cochrane analysis of 26 studies (6) evaluating PCT, there was no difference in 30 day mortality between a PCT directed algorithm and standard of care:

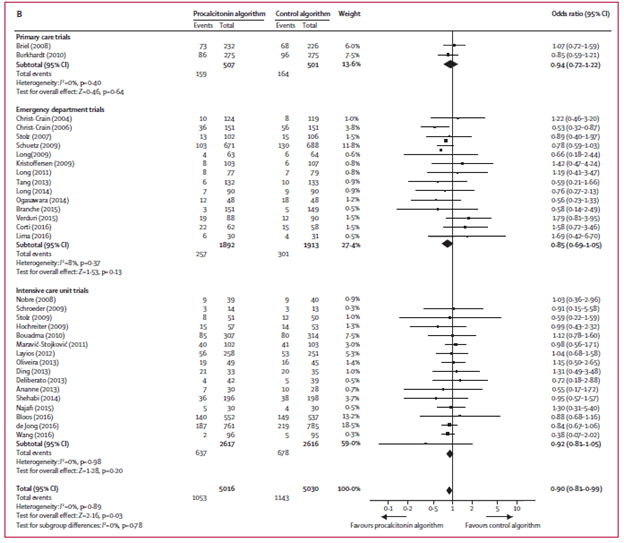
Further, treatment failure at 30 days favored PCT-guided therapy, but this may have been a statistical fluke:
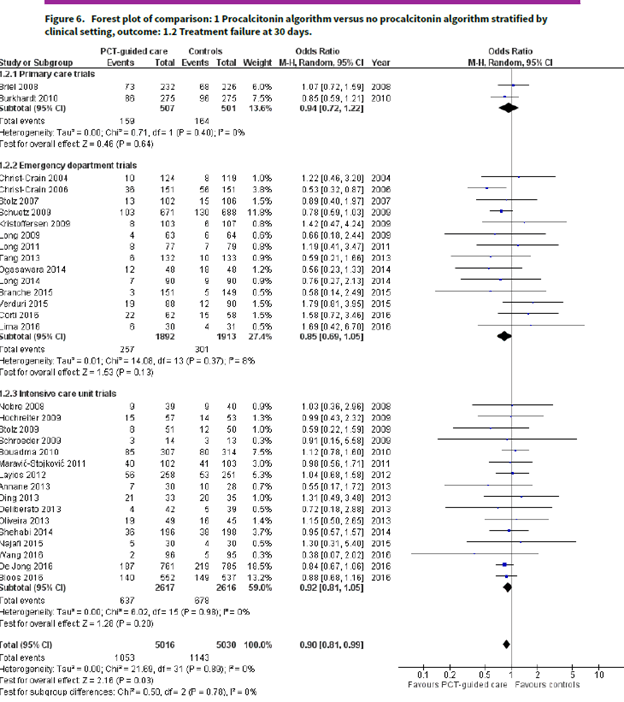
And to complete the trifecta of studies of PCT on mortality (from the same author!), this meta-analysis (7) evaluated 6708 patients in 26 trials to evaluate all-cause mortality within 30 days as well as treatment failure within 30 days. Most of these trials were in the ED and in ICUs. Overall, the use of PCT did not affect all cause mortality:
There was also no differences in treatment failure:
This suggests that the use of PCT for pulmonary infections may be associated with lower antibiotic use (actually, it is, duh) without any impact on mortality or treatment failure/relapse. So as a diagnostic tool, doesn’t really (given the positive likelihood ratio of ~2, doesn’t really tip the scale if positive), but if negative it is helpful for de-escalating antibiotics without any impact on outcomes.
Utility of PCT in Asthma and COPD
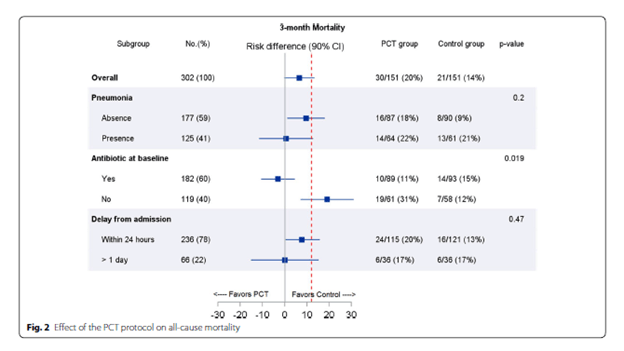
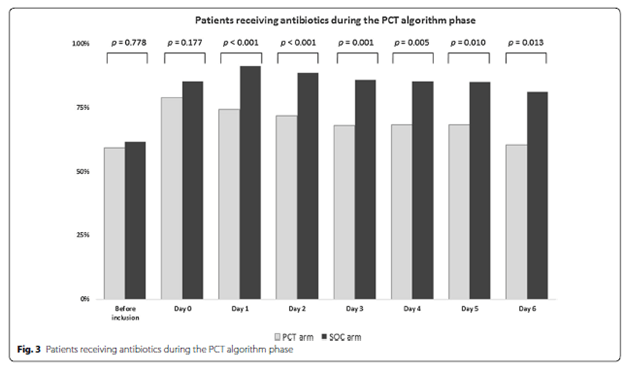
PCT can be used for COPD and asthma exacerbations to de-escalate antibiotic therapy. For instance, in a prospective, multicenter RCT from France (8) PCT guided antibiotic therapy was evaluated for all-cause 3 month mortality in COPD patients being admitted to the ICU. 302 patients were enrolled. Overall, there was no statistical difference in 3 month mortality between groups, although those who PCT use was associated with higher mortality in those patients who did not get antibiotic therapy upfront:
While there was a trend toward decreased antibiotic use in the PCT group;
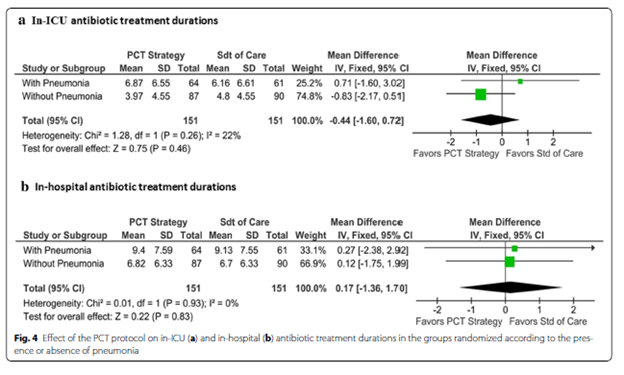
The exposure duration during ICU stay or in-patient stay was not different in both groups:
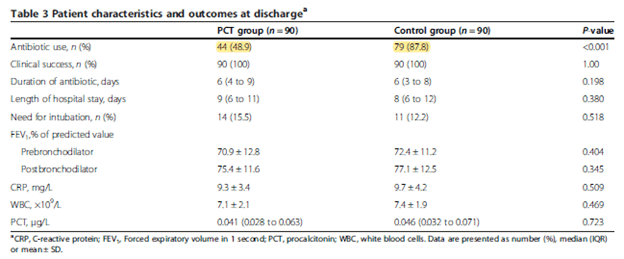
In a single center RCT, a PCT cutoff of <0.1 was used to withhold antibiotics in patients presenting with COPD. Primary outcome was treatment success rate at day 10, and all patients were treated for COPD exacerbation per usual including antibiotics. In the non-antibiotic group, 17.7% of patients received antibiotic therapy. Overall, there was no difference in the 10d success rate or length of hospital stay between 2 groups, suggesting that low PCT in COPD exacerbation did not require antibiotic therapy:
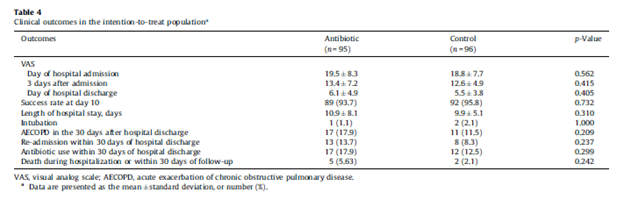
In another randomized controlled trial of PCT use in asthma-exacerbation patients (10), 180 patients were randomized to either standard anti-microbial group or PCT guided group. Primary outcome was antibiotic use, with secondary endpoints including treatment success, length of stay, and lab/spirometry outcomes at discharge and at 12 months. Not surprisingly, there was a significant difference in antibiotic use:
But no real difference in other secondary outcomes at 12 months.
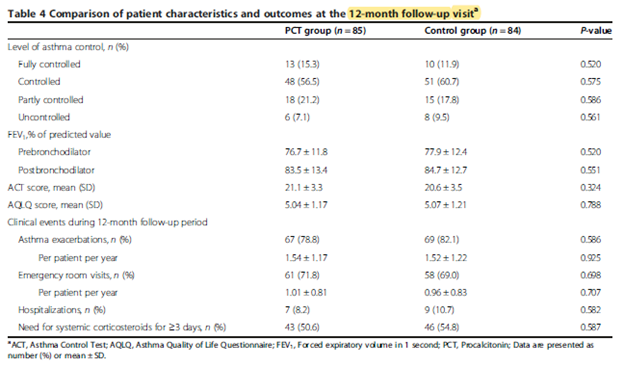
This suggest the use of PCT-guided antibiotic usage for asthma may be a reasonable option without any harms in terms of long term outcomes, though these were secondary endpoints and the study was not adequately powered to look into differences of length of stay or treatment success/failure. Notably, both groups had comparable readmission rates and exacerbation-free rates:

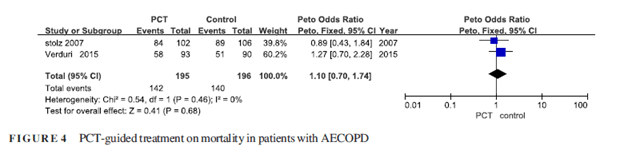
Two other meta-analysis on COPD suggested no impact of de-escalation of antibiotics on mortality or re-admission. For instance, in one meta-analysis (11) of of 4 RCTs evaluating the use of PCT to guide therapy for COPD exacerbations, there was no statistical difference in clinical outcomes:
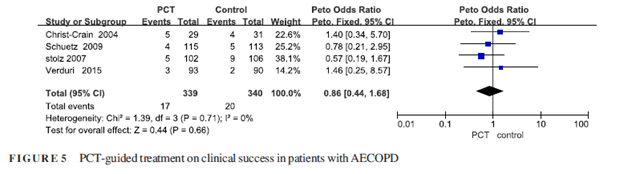
Mortality:
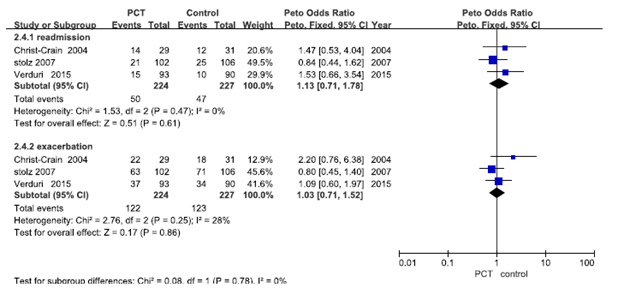
Or readmission rates:
Overall, this seems to suggest that for COPD, PCT can be used to de-escalate therapy on the in-patient setting, though its utility for starting antibiotics is questionable. The trend held true in another meta-analysis of 8 studies (12), with PCT guided therapy being associated with decreased antibiotic prescriptions, but not with decreased antibiotic exposure days or their use after discharge. Though one things to consider was the degree of heterogeneity between the studies, though the authors report the risk ratio did not change when any single study was excluded:
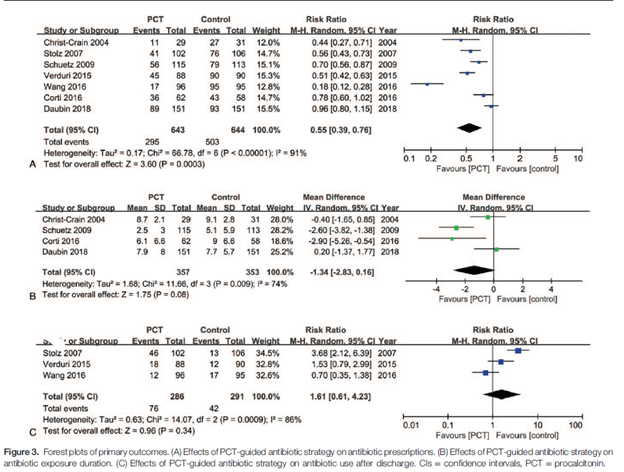
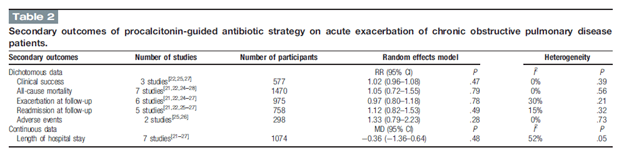
Overall, secondary outcomes which included all-cause mortality, exacerbation at follow up, or readmission at follow up were not statistically different.
With this, it seems that for patients presenting with either an asthma exacerbation or COPD exacerbation, starting antibiotics upfront may be a reasonable idea and PCT can be used to de-escalate antibiotic therapy without much of an impact on outcomes. The PCT threshold used in these studies was 0.25, which is lower than the 0.5 used in other studies, but allows a higher specificity for non-bacterial infections (i.e. by setting the threshold lower, you are not going to miss bacterial etiologies as often).
Utility of PCT in the ICU setting
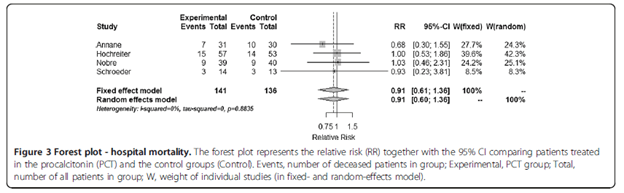
This deals mostly with septic shock. In general, PCT in the ICU setting tends to not perform terribly well when it comes to de-escalating antibiotics. For instance, in a meta-analysis of 7 RCTs evaluating the utility of PCT in severe sepsis and septic shock (13), there was no difference between in-hospital mortality in the PCT-guided group and the standard therapy group:
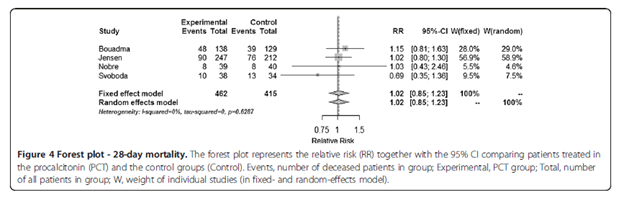
This was the same in the 28d mortality:
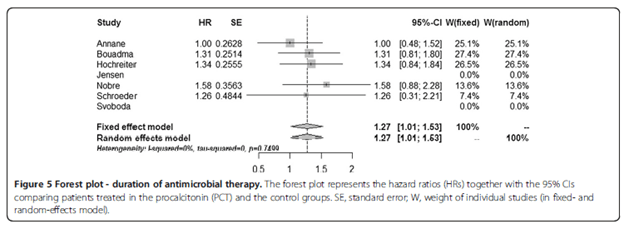
In terms of antibiotic therapy, the PCT group had lower antibiotic therapy duration but the results were barely statistically significant:
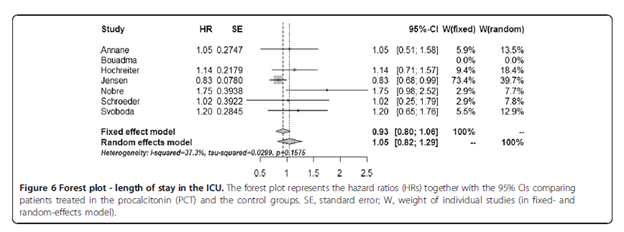
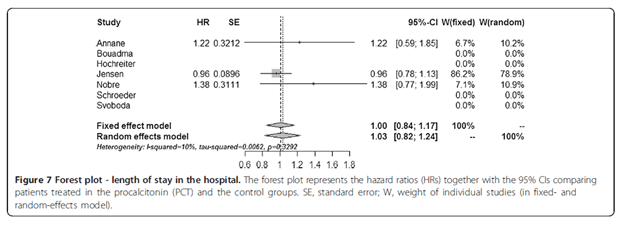
Both ICU length of stay and hospital length of stay did not differ between groups:
This suggests that while a PCT-guided antibiotic cessation may not impact mortality in the ICU setting, the difference in antibiotic duration is not terribly impressive between a PCT-protocol or a standard antibiotic de-escalation protocol. Further, another meta-analysis had similar findings in terms of mortality, but it may have been driven by a much less sicker group of patients. In this meta-analysis of 16 studies (14), there was no difference in mortality between the PCT-guided therapy for septic shock or the standard group:
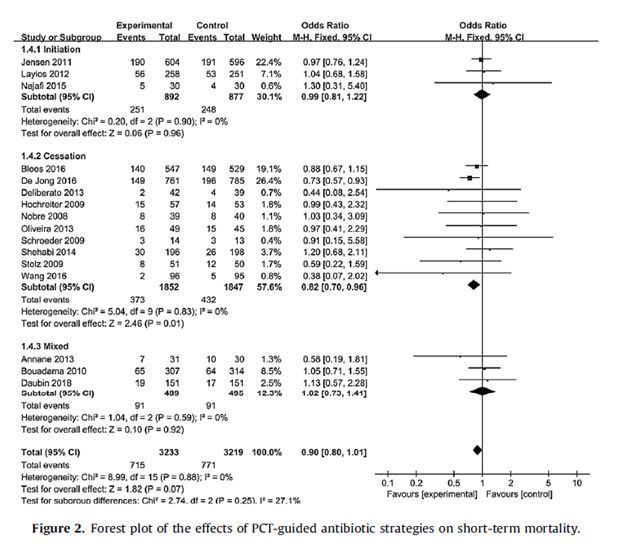
Though PCT-guided cessation of antibiotics was associated with decreased 28 day mortality (RR 0.82, 95% CI 0.70-0.96, p-value 0.01), there no difference was found for the initiation group (RR 0.99, 95% CI 0.81-1.22, p-value 0.96). Further, the benefit derived from a less sicker cohort and those with lack of adherence to PCT-guided therapy. Go figure.
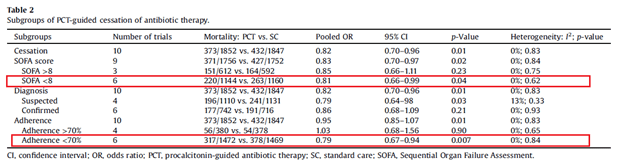
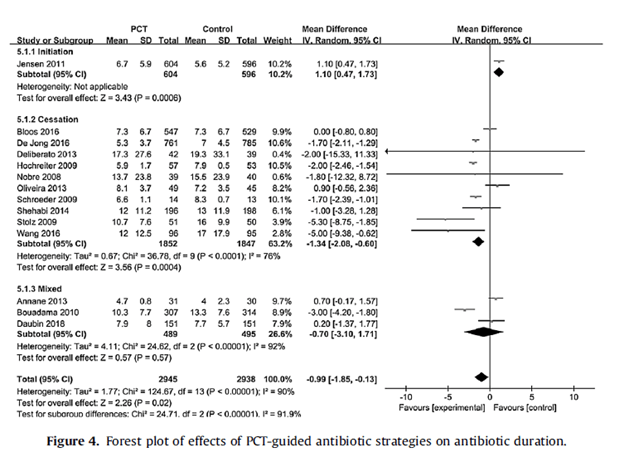
Predictably, PCT-guided therapy was associated with lower antibiotic usage, with a mean antibiotic duration being 0.99 days shorter in the PCT-guided group:
The role of PCT in the ICU setting is still a bit murky. While there is no evidence that its use is causing harm, whether or not it is doing something in terms of driving treatment decisions is still unclear, at least looking at these data. It may do better in the COPD/asthma patients who get admitted to the unit, though.
PCT for Prognostication:
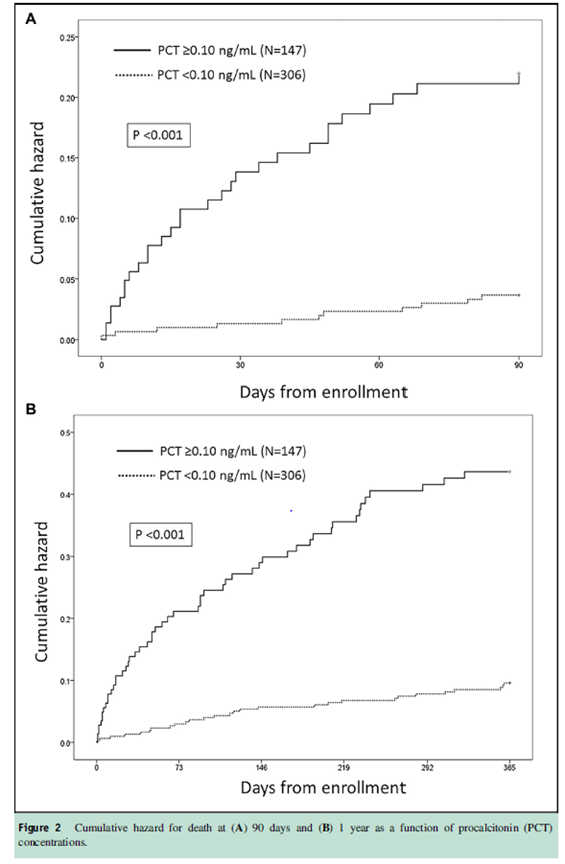
As mentioned previously, patients with bacterial pneumonia had higher levels of PCT (2) and indeed, higher levels of PCT were associated with higher mortality:
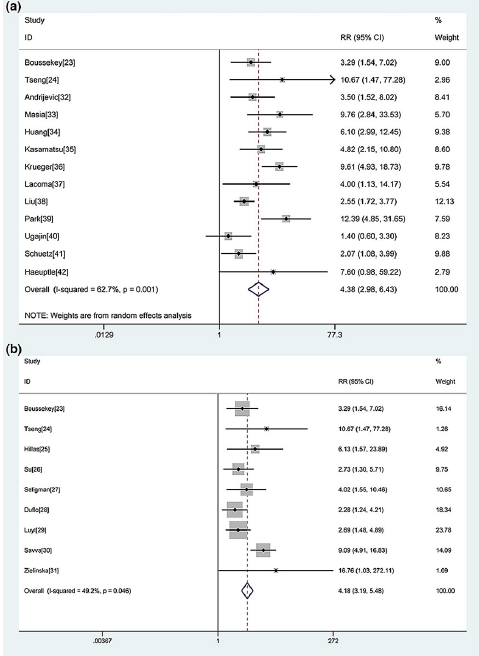
Further, it has been found that PCT levels correlated with higher scores on the pneumonia severity index scale. For instance, patients with PSI of I-III had a median PCT level of 0.3, compared to a median of 0.7 in patients with PSI IV-V (15). A meta-analysis of 21 studies (16) found that elevated PCT in CAP was found to be associated with increased mortality, with RR of 4.38 (95% CI 2.98-6.43). Pooled sensitivity and specificity for mortality were 69% (95% CI 57-79%) and 74% (95% CI 60-84%) respectively. For ICU mortality, elevated PCT had a RR of 4.18 (95% CI 3.19-5.48):
Further, studies with a PCT cut-off of 0.5mg/mL had low sensitivity for predicting mortality in CAP, with functional assays <1ng/mL showing higher sensitivity overall:
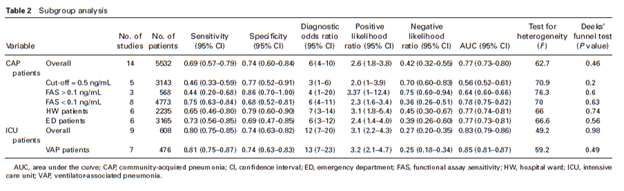
ROC for CAP patient showed an AUC of 0.76 (95% CI 0.73-0.80) while AUC of ICU patients was 0.83 (95% CI 0.79-0.86), showing that PCT in ICU patients had a better diagnostic accuracy, at least for predicting mortality:

What can I say at the end of all of this? In general, procalcitonin may not be terribly helpful to diagnose a bacterial pneumonia. Some viral etiologies can give you an elevated PCT, so you’re stuck with antibiotics. A negative PCT may be helpful to de-escalate antibiotic therapy in the right clinical setting, for instance, if there is no infiltrate on CXR during a respiratory illness, then a low PCT can be used to stop antibiotics (at worse, you would be missing a bronchitis which does not necessarily need antibiotics). Further, this can also be used in COPD and asthma exacerbations without any risk of increasing mortality or readmission rates, which is a plus. The utility in the ICU setting is still up in the air and quite honestly, I would not use it here.
References:
- Self WH, Balk RA, Grijalva CG, et al. Procalcitonin as a Marker of Etiology in Adults Hospitalized With Community-Acquired Pneumonia. Clin Infect Dis. 2017;65(2):183-190. doi:10.1093/cid/cix317
- Alba GA, Truong QA, Gaggin HK, et al. Diagnostic and Prognostic Utility of Procalcitonin in Patients Presenting to the Emergency Department with Dyspnea. Am J Med. 2016;129(1):96-104.e7. doi:10.1016/j.amjmed.2015.06.037
- Wussler D, Kozhuharov N, Tavares Oliveira M, et al. Clinical Utility of Procalcitonin in the Diagnosis of Pneumonia. Clin Chem. 2019;65(12):1532-1542. doi:10.1373/clinchem.2019.306787
- Caffarini EM, DeMott J, Patel G, Lat I. Determining the Clinical Utility of an Absolute Procalcitonin Value for Predicting a Positive Culture Result. Antimicrob Agents Chemother. 2017;61(5):e02007-16. Published 2017 Apr 24. doi:10.1128/AAC.02007-16
- Schuetz P, Christ-Crain M, Thomann R, et al. Effect of procalcitonin-based guidelines vs standard guidelines on antibiotic use in lower respiratory tract infections: the ProHOSP randomized controlled trial. JAMA. 2009;302(10):1059-1066. doi:10.1001/jama.2009.1297
- Schuetz P, Wirz Y, Sager R, et al. Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst Rev. 2017;10(10):CD007498. Published 2017 Oct 12. doi:10.1002/14651858.CD007498.pub3
- Schuetz P, Wirz Y, Sager R, et al. Effect of procalcitonin-guided antibiotic treatment on mortality in acute respiratory infections: a patient level meta-analysis. Lancet Infect Dis. 2018;18(1):95-107. doi:10.1016/S1473-3099(17)30592-3
- Daubin C, Valette X, Thiollière F, et al. Procalcitonin algorithm to guide initial antibiotic therapy in acute exacerbations of COPD admitted to the ICU: a randomized multicenter study. Intensive Care Med. 2018;44(4):428-437. doi:10.1007/s00134-018-5141-9
- Wang JX, Zhang SM, Li XH, Zhang Y, Xu ZY, Cao B. Acute exacerbations of chronic obstructive pulmonary disease with low serum procalcitonin values do not benefit from antibiotic treatment: a prospective randomized controlled trial. Int J Infect Dis. 2016;48:40-45. doi:10.1016/j.ijid.2016.04.024
- Long W, Li LJ, Huang GZ, et al. Procalcitonin guidance for reduction of antibiotic use in patients hospitalized with severe acute exacerbations of asthma: a randomized controlled study with 12-month follow-up. Crit Care. 2014;18(5):471. Published 2014 Sep 5. doi:10.1186/s13054-014-0471-7
- Lin C, Pang Q. Meta-analysis and systematic review of procalcitonin-guided treatment in acute exacerbation of chronic obstructive pulmonary disease. Clin Respir J. 2018;12(1):10-15. doi:10.1111/crj.12519
- Li Z, Yuan X, Yu L, Wang B, Gao F, Ma J. Procalcitonin-guided antibiotic therapy in acute exacerbation of chronic obstructive pulmonary disease: An updated meta-analysis. Medicine (Baltimore). 2019;98(32):e16775. doi:10.1097/MD.0000000000016775
- Prkno A, Wacker C, Brunkhorst FM, Schlattmann P. Procalcitonin-guided therapy in intensive care unit patients with severe sepsis and septic shock–a systematic review and meta-analysis. Crit Care. 2013;17(6):R291. Published 2013 Dec 11. doi:10.1186/cc13157
- Peng F, Chang W, Xie JF, Sun Q, Qiu HB, Yang Y. Ineffectiveness of procalcitonin-guided antibiotic therapy in severely critically ill patients: A meta-analysis. Int J Infect Dis. 2019;85:158-166. doi:10.1016/j.ijid.2019.05.034
- Christ-Crain M, Stolz D, Bingisser R, et al. Procalcitonin guidance of antibiotic therapy in community-acquired pneumonia: a randomized trial. Am J Respir Crit Care Med. 2006;174(1):84-93. doi:10.1164/rccm.200512-1922OC
- Liu D, Su LX, Guan W, Xiao K, Xie LX. Prognostic value of procalcitonin in pneumonia: A systematic review and meta-analysis. Respirology. 2016;21(2):280-288. doi:10.1111/resp.12704

1 comments on “Procalcitonin in Infectious Disease”