
Meningitis is defined as inflammation of the meninges, characterized by an abnormal number of WBCs on the CSF. The most common cause of meningitis is viral, with organisms such as echovirus, coxsackievirus, and the enteroviruses being a common etiology. Further, bacterial meningitis can be caused by H. influenzae and Streptococcus spp. One odd etiology is fungal meningitis. Typically this is seen in immunocompromised hosts, however a recent series of odd events have made international headlines, as fungal meningitis has been linked to contaminated epidural anesthesia in cosmetic surgery clinics in Matamoros, Mexico (1). Unfortunately, we have been here before.
The original outbreak from 2002 identified 5 patients with fungal meningitis, who ended up growing Exophiala dermatitidis, occurring up to 152 days after injection with contaminated methylprednisolone (2). All cases were treated with voriconazole and only one had died. Several things are notable with this outbreak, mainly the timeframe from initial exposure to presentation. Further, it was found that some strains of fungi can have their growth enhanced due to methylprednisolone. This was seen in one study, which found that certain species of aspergillus yielded higher growth rate when incubated with hydrocortisone (3):
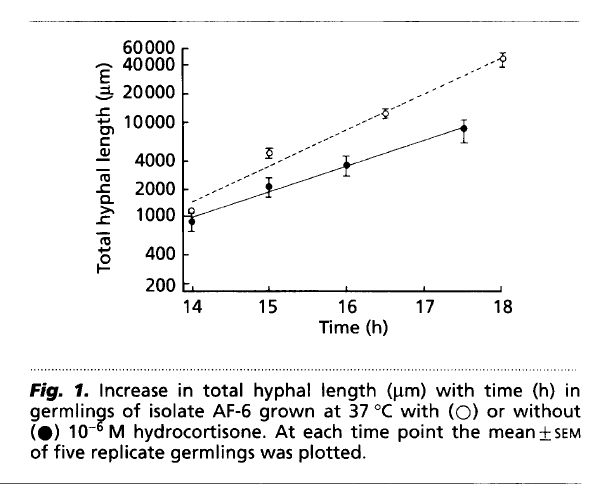
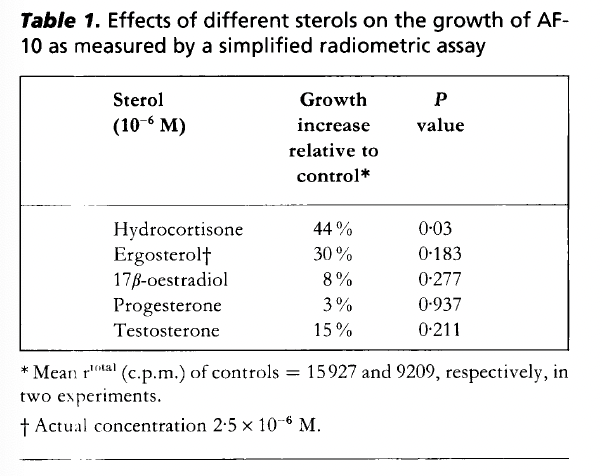
The same effect was not seen with A. oryzae or A. niger, however it was seen with A. flavus.
The 2012 Outbreak
This is the big one that everyone talks about. The index case highlighted a male who presented with meningismus roughly 4 weeks after his last methylprednisolone injection (4). His presentation was delayed, with the initial CSF showing significant pleocytosis and was treated for presumed bacterial meningitis, and his course was complicated by the development of seizure-like activity and intraventricular and subarachnoid hemorrhage. Interestingly, this patient ended up growing Aspergillus fumigatus, in comparison to the other cases, which grew E. rostratum. A preliminary study from the Tennessee Department of Health identified 66 patients who met the definition of iatrogenic fungal infection (5). Median time from injection to symptom onset was 18 days, ranging up to 56 days in one case. Of these, 71% had meningitis, 17% had cauda equina syndrome. Moreover, 12% had posterior circulation stroke with or without meningitis. Other symptoms included vertigo in 17% of cases and falls in 14%. The CSF of patients who had meningitis or meningitis with stroke is described below:
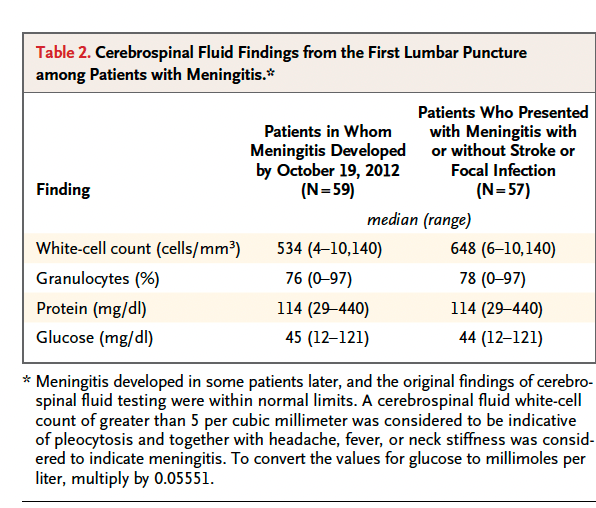
All had pleocytosis and elevated protein though glucose was overall normal. MRI of spine findings included arachnoiditis, neuritis, epidural abscess, psoas or paraspinal muscle abscess, ventriculitis, enhancement of meningitis, and subarachnoid hemorrhage. Infarcts were seen in the thalamus, pons, midbrain, and cerebellum. When comparing patients who had a stroke with those who did not, there was no difference in terms of time from symptom onset to start of IV antifungal therapy or time from symptom onset to LP. Mortality amongst those who had a stroke was high at 88%. Univariate analysis found that female sex, age over 60, multiple procedures, and translaminar epidural glucocorticoid injection were associated with higher risk of fungal meningitis:

These findings were confirmed in a multivariate analysis: age >60 (aOR 4.01, 95% CI 1.95 to 8.24), female sex (aOR 2.56, 95% CI 1.29 to 5.12), cumulative dose of 06292012@26 lot injected 45 to 60 days and more than 60 days after production in 40mg increments (aOR 1.29, 95% CI 1.02 to 1.64 and aOR 1.65, 95% CI 1.29 to 2.11, respectively).
PCR techniques found that E. rostratum was the main pathogen, which is a dematiaceous (black) mold that contains melanin in its cell wall and is found in the environment, including plants, soil, and water. In this cohort, the calculated attack rate was 5.5 cases per 100 people exposed.
Another study of 172 patients found that the incubation period ranged from 1 to 71 days, with 25 having met the case definition for meningitis based on the CSF WBC count (6). As highlighted below, all had significant pleocytosis:
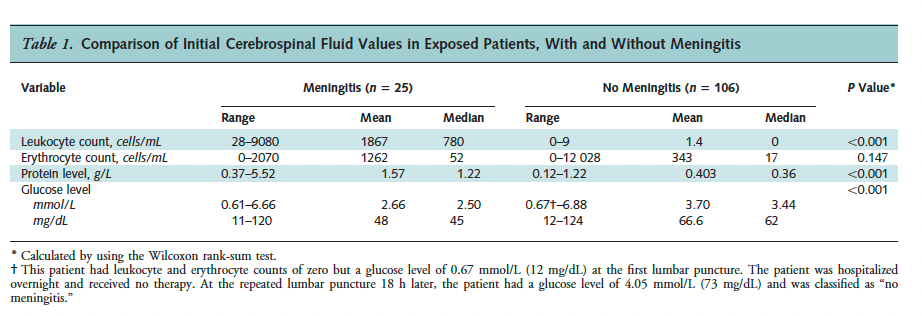
Moreover, headache was the predominant symptoms however other neurological symptoms such as word-finding difficulty, gait disturbances, and sensory changes were also present:

Not surprisingly, 64% of the patients treated with voriconazole experienced transaminitis, usually a mean of 9 days after therapy initiation. In this cohort, LPs were planned every 3 to 4 weeks until negative samples were obtained, and a favorable outcome was seen when there was a decrease in CSF WBC.
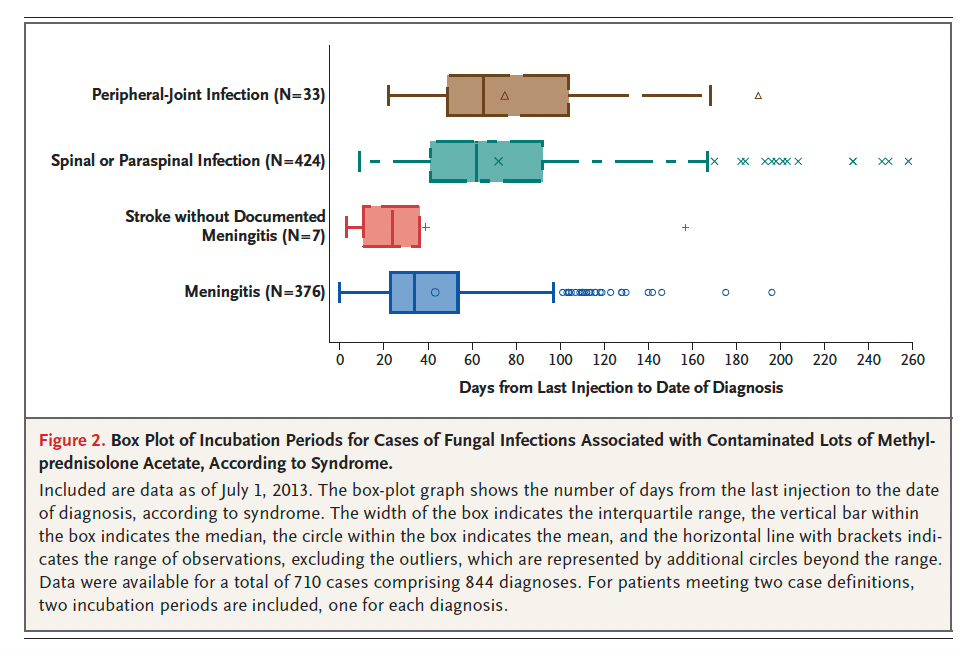
The epidemiological investigation involved over 17,000 vials of methylprednisolone distributed to 76 facilities across 23 states (7). Over 13,000 people were exposed to at least one of these lots, with most undergoing spinal, epidural, or paraspinal injections. While spinal injections were the most common use of methylprednisolone, at least 1648 had peripheral joint injections. One cohort identified 749 cases, of which 61 had died. Within this cohort, 43% had either spinal or paraspinal infections only, 233 had meningitis only, 151 had both paraspinal infection and meningitis, and 33 had joint related infection. Notably, only 7 had a stroke from presumed meningitis, however the CDC had reported 40 patients who had a stroke however whether these were from fungal meningitis it is not known. The most common symptoms for those who had meningitis included headache (88%) and neck stiffness (49%). CSF studies showed pleocytosis, with those who had both meningitis and spinal/paraspinal infection having higher WBC than the meningitis cohort:
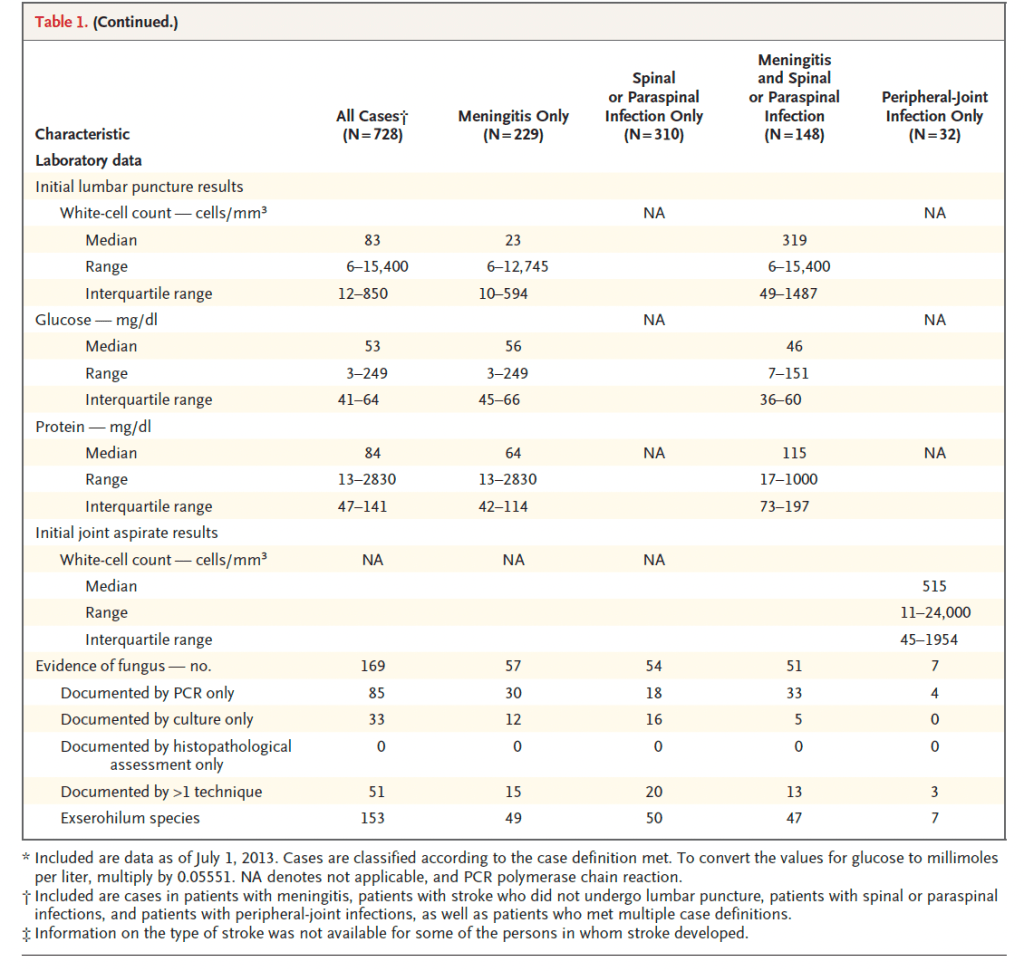
Notably, the mean incubation was 47 days, with the longest being for peripheral joint infections (65 days), and the showertes are those with a stroke without documented meningitis (24 days).
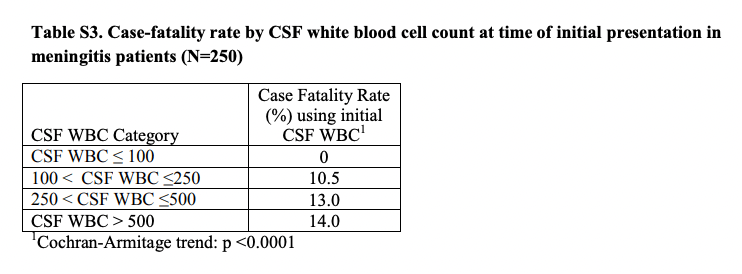
The most thorough review of 328 patients identified 265 patients with CNS infections, of which 250 had meningitis (8):
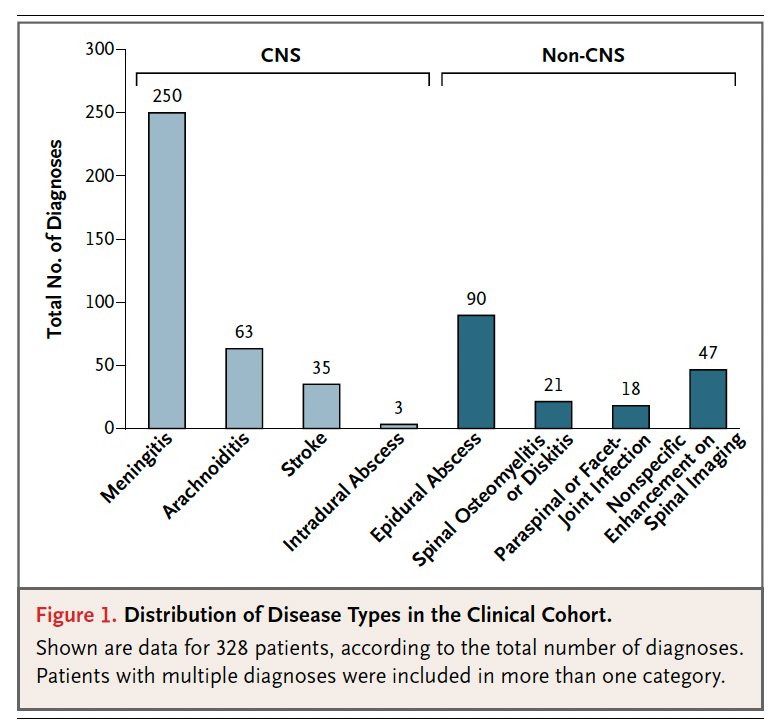
Headache, fever, neck pain, back pain, and neurological deficits were the most commonly cited symptoms across this cohort. 35 of these patients had a stroke, mostly localized in the areas supplied by the vertebrobasilar vessels such as the cerebellum and brainstem. Notably, the CSF from those who had strokes tended to have a higher mean WBC count when compared to those who had meningitis only:
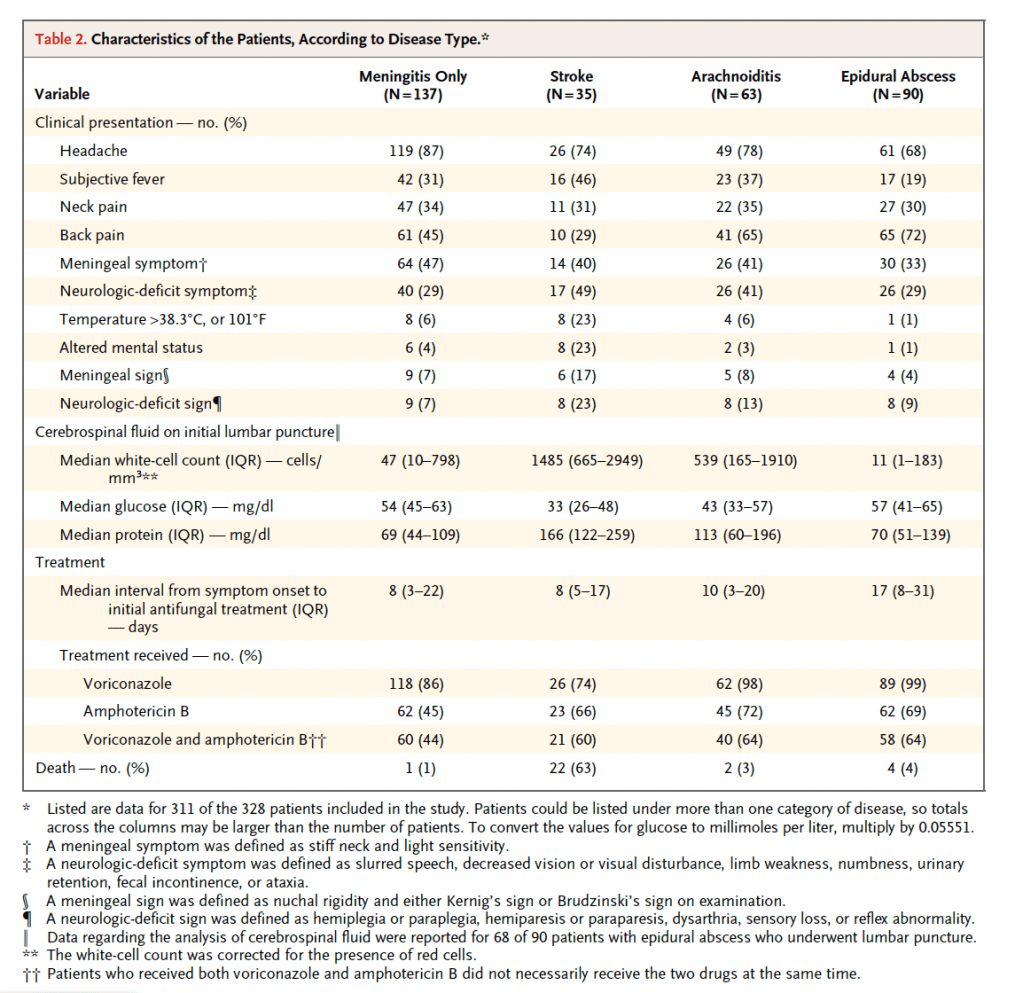
Indeed, higher WBC count was correlated with higher case fatality:
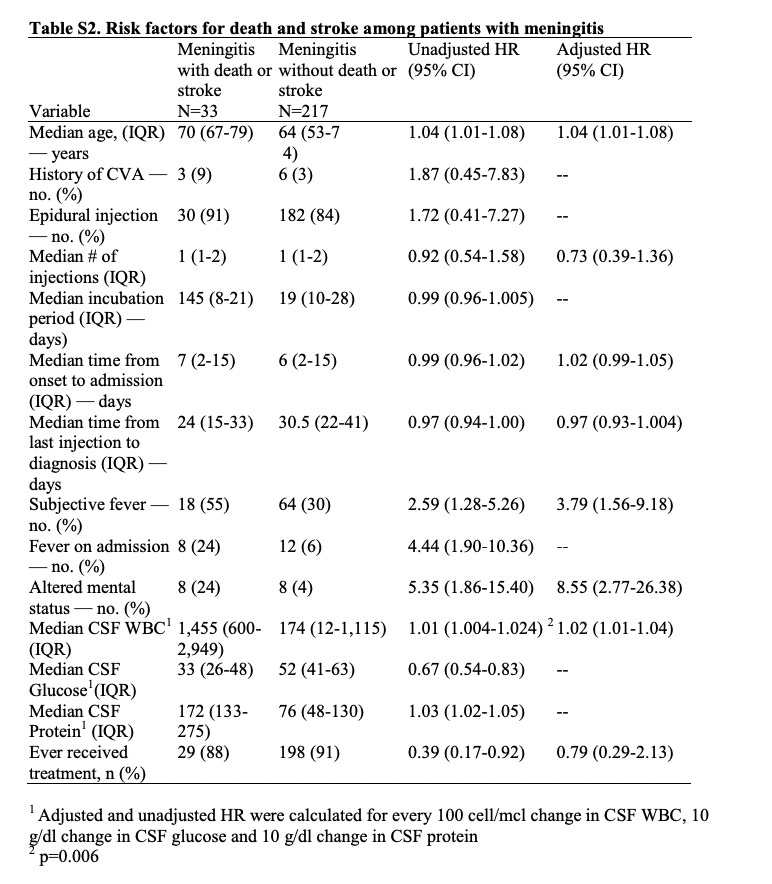
Risk factors for death and stroke included older age, altered mental status, presence of fever, and high WBC count:
Moreover, E. rostratum was not the only organism found on PCR assay. 7 others were found, including Alternaria alternata, Aspergillus fumigatus, Aspergillus terrus, A. tubingensis, Paecilomyces niveus, Stachybotrys chartarum, and Cladosporium spp.
A few patterns emerge here:
- The incubation time can be long, several weeks up to months.
- The more common presentations are localized infections such as spinal abscesses
- Higher CSF WBC are correlated with worse outcomes
- Strokes, both hemorrhagic and ischemic, have been described
2023 Cases
So what is going on this time around? The current outbreak stems from 2 clinics in Matamoros, Mexico, near the border of Texas, that provide cosmetic surgeries including tummy tucks, liposuction, and BBLs. Spinal anesthesia provided to the patients is the source of the cases of meningitis. Starting this past month (May 2023), several young patients presented with headaches, photophobia, fevers, and findings of papilledema several weeks after their procedure (see below, provided by P. Vega, MD VBMC-Harlingen/UTRGV, personal communication):

Several compilations have been noted, including hemorrhagic strokes, increased intracranial pressure, and vasospasm with at least 2 dead from strokes and one other still in critical condition as of the time I am writing this. PCR sent to University of Washington confirmed the organism to be Fusarium solani, which was also seen in a similar outbreak in November 2022 in Durango, Mexico. The CSF studies are also similar to those of the prior cases, with one notable test:
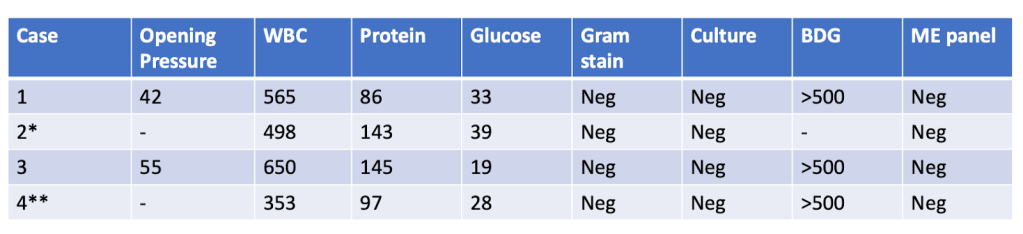
All had elevated CSF pressure and significant pleocytosis.
One of the most interesting tidbits in these cases are the vascular complications. Indeed, many of these patients have a change in mental status during their disease course, only to have subarachnoid hemorrhages or ischemic strokes. As a result, we have prophylactically done angiograms showing basilar artery mycotic aneurysm and vasospasms, however this should not have been a surprise. A case series of 3 patients who presented with fungal meningitis were found to have ischemic strokes in the midbrain, thalamus, cerebellum, lateral pons, and internal capsule (9). The pathogenesis of mycotic aneurysms results from degradation of the arterial wall secondary to microbial infection (10). The infection leads to acute infiltration of both the media and adventitia vessel wall by PMNs, as well as marked proliferation of the intima and destruction of the elastic lamina. Pulsations from blood flow then promote the development of the aneurysm. These can develop quite quickly. An animal study of dogs found that three days after infection with S. aureus, inflammatory cell infiltration in the outer one-third of the media and adventitia were already seen (11). Destruction of the media and disappearance of muscle and elastic fibers were seen one week after infection, with media muscle cells being replaced by inflammatory cell infiltration. Ischemic strokes have also been seen, with one case having multiple strokes in the pons, midbrain, cerebellum, thalamus, and brainstem (12).
CSF Beta-D Glucan
I mentioned something about the above CSF studies, and that is the beta-D glucan, which is a marker used for a variety of fungal infections (and to be fair, this is the purpose of the post). I think this is a helpful tool, as it has been notoriously difficult to culture this fungi, and many of the molecular diagnostics are not widely available. One animal study evaluated the utility of BD-glucan in the rat model for hematogenous candida meningoencephalitis (13). Notably, only 5 of 62 animals with established CNS infection yielded a positive culture, however mean concentration of BD-glucan in untreated rabbits was 3801 pg/mL. Indeed, this seem to correlate with CSF fungal burden:
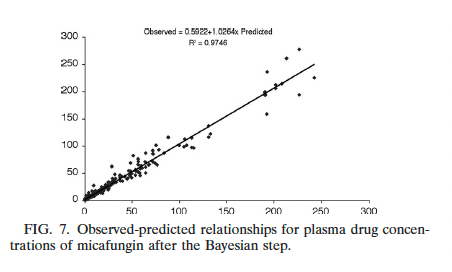
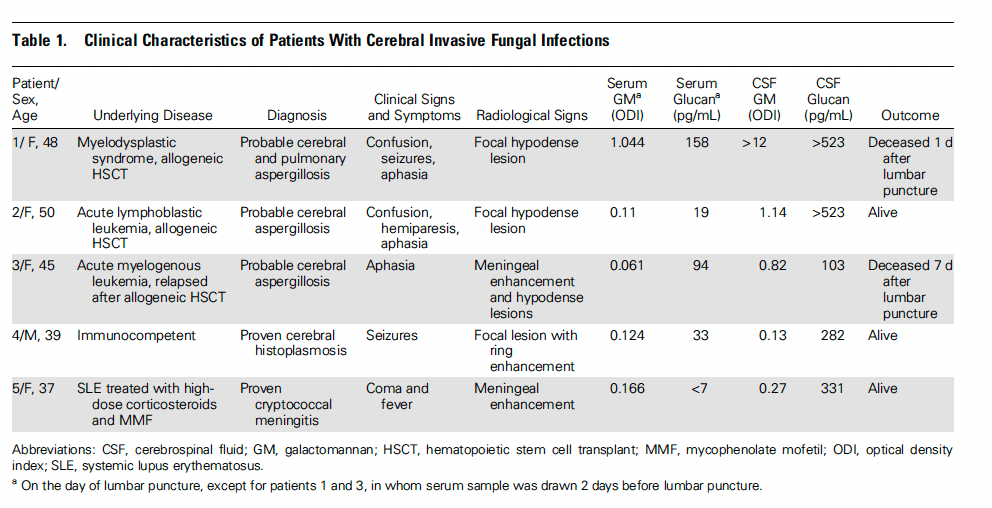
One interesting observation was that BD glucan decreased significantly with micafungin therapy, with increasing dose being correlated with a gradual decrease in CSF BD-glucan. One proof-of-concept study evaluated the utility of BD glucan off CSF in hematological patients with cerebral aspergillosis (14). All 5 patients studied had positive levels of BD glucan:
In a cohort of pediatric patients with leukemia, BD glucan CSF was used to track CNS fungal infections (15). The pattern of clearance correlated with favorable therapeutic outcomes:
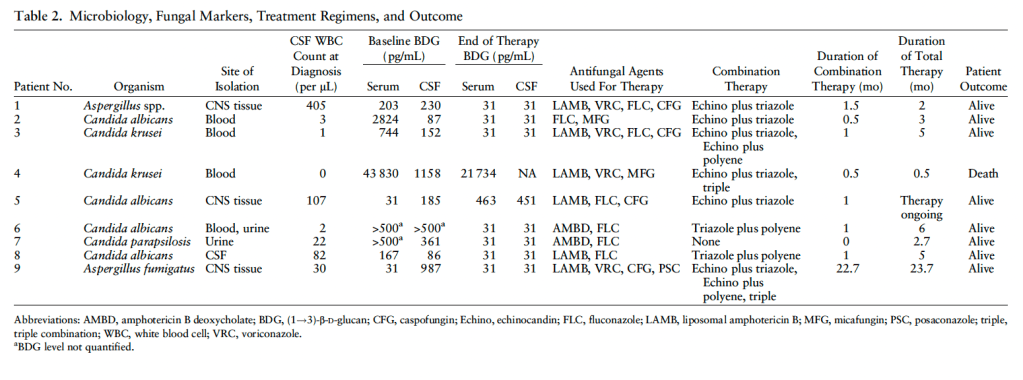
As can be seen, those whose CSF BD-glucan reached undetectable levels had a more favorable outcome, suggesting this can be used as a prognostic marker.
A retrospective cohort of patients with disseminated fungal infections, CNS fungal infections, and non fungal CNS infections compared CSF BD glucan across said patients (16). 15% of 66 patients without fungal infection had an undetectable ( <4 pg/mL) BD glucan compared to the rest, which had a BD glucan ranging from 4 up to 109 pg/mL. Compare this with those with definitive or probable CNS infections, which had higher CSF BD glucan levels:
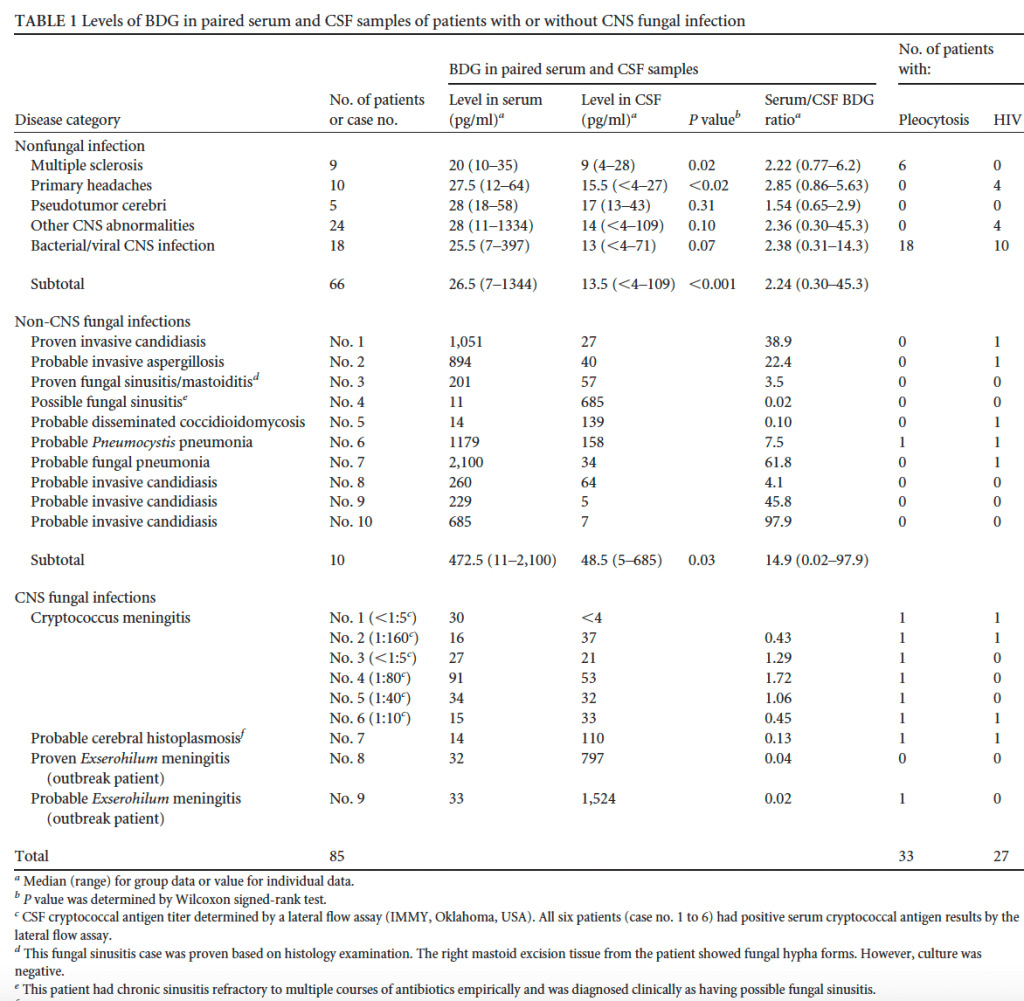
Despite this, there were no differences in the CSF BD glucan levels when analyzed by the presence or absence or CSF pleocytosis. Moreover, 27 patients were infected with HIV, making the generalizability of this cohort a bit problematic to the current outbreak. One cohort of 26 patients with coccidioidal meningitis had their CSF BD-glucan levels compared to 11 controls (17). Using a cut-off of 31pg/mL, the BD glucan was able to discriminate against meningitis with a 96% sensitivity, 82% specificity, and a PPV and NPV of 93% and 90%, respectively:
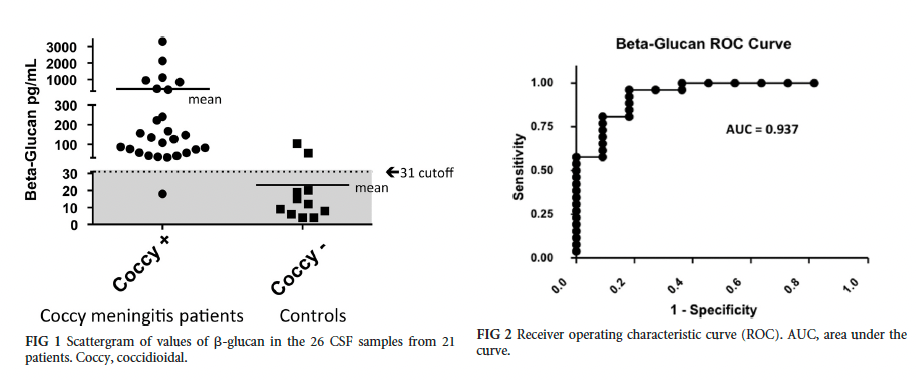
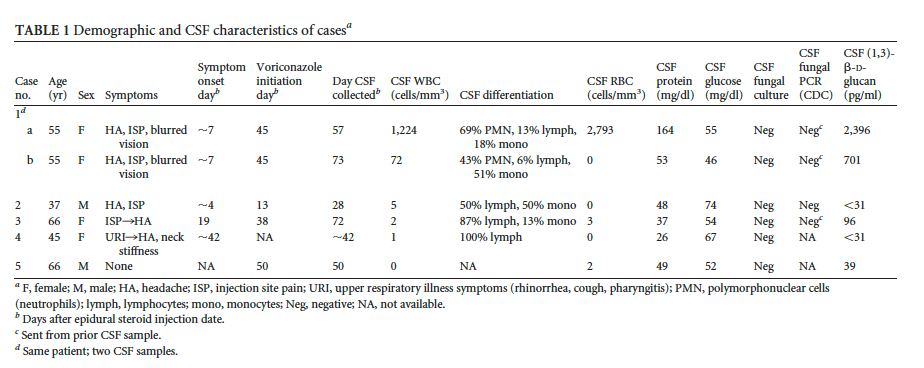
Using a cutoff of 103 pg/mL, the ROC was 0.937, yielding a sensitivity of 100%. What about data from the 2012 outbreak? Here, 5 individuals had CSF BD glucan levels monitored (18). One notable thing was that the levels ranged from undetectable to 2396, with CSF studies also ranging in terms for their WBC counts:
Of course, this study is small and it makes it difficult to draw a conclusion in terms of CSF WBC and BD glucan levels, and which one can be used to track disease progression, however it serves as a proof-of-concept that BD glucan off CSF can be a meaningful marker. One of the largest retrospective studies involved 223 patients, of which 45 were found to have fungal meningitis and 32 found to have spinal or paraspinal infections (19). The rest, 135, received the injection but did not develop meningitis. Using a cut-off of 80pg/mL, 96% of the proven meningitis cases were positive, while 84% of both proven and probable cases were positive. The sensitivity and specificity for proven meningitis was 96% and 95%, respectively while for probable meningitis it was 84% and 95% respectively. Notably, those who had proven meningitis tended to have significantly higher levels of CSF BD glucan:
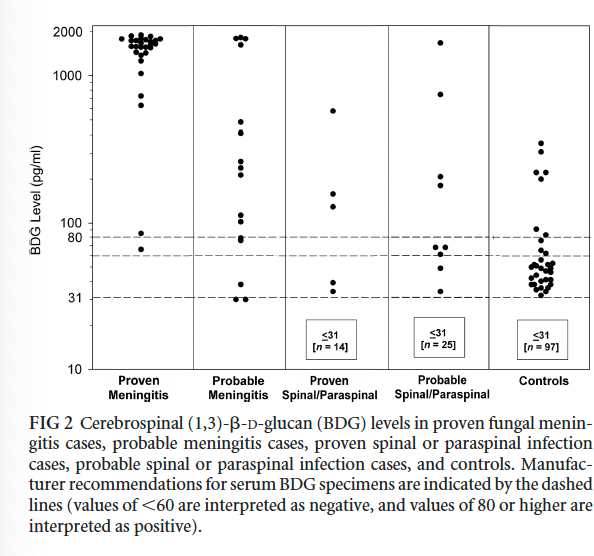
Using a cut-off of 66pg/mL, the sensitivity and specificity were 100% and 94%, respectively.
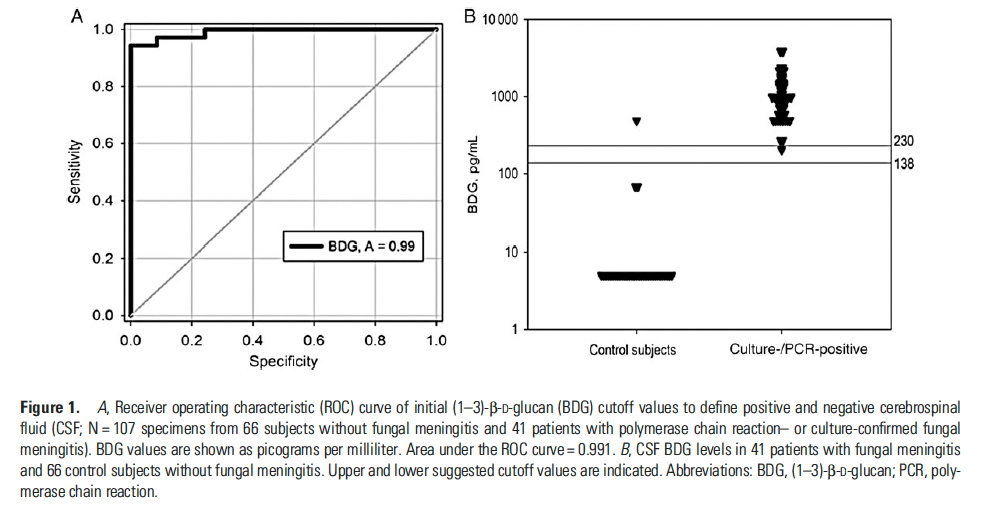
A cohort of 41 patients from the 2012 outbreak found that a cutoff value of 138 pg/mL had a sensitivity and specificity of 100% and 98%, respectively, with a PPV of 32.5 (20):
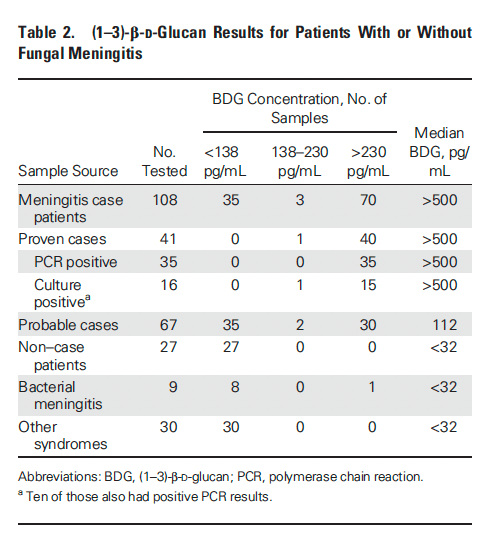
Using a cutoff of 138pg/mL, 41 samples from confirmed meningitis were analyzed and found that 40 of 41 had a BD glucan level >230. Amongst 67 cases of probable meningitis, BDG greater than 230 were found in 30 cases only, with a median level of 112, compared to >500 in those with confirmed meningitis:
The most interesting part of this paper is the serial samples of BD glucan. Here, the authors divided the patients into 2 groups depending on whether levels decreased below 500. Those who had persistently elevated BD glucan levels >500 had worse outcomes, defined as stroke, replaced meningitis, or soft tissue phlegmon. Those whose BD glucan decreased tended to have better outcomes, even if they remained above 138 pg/mL suggesting it can be used as a prognostic indicator:
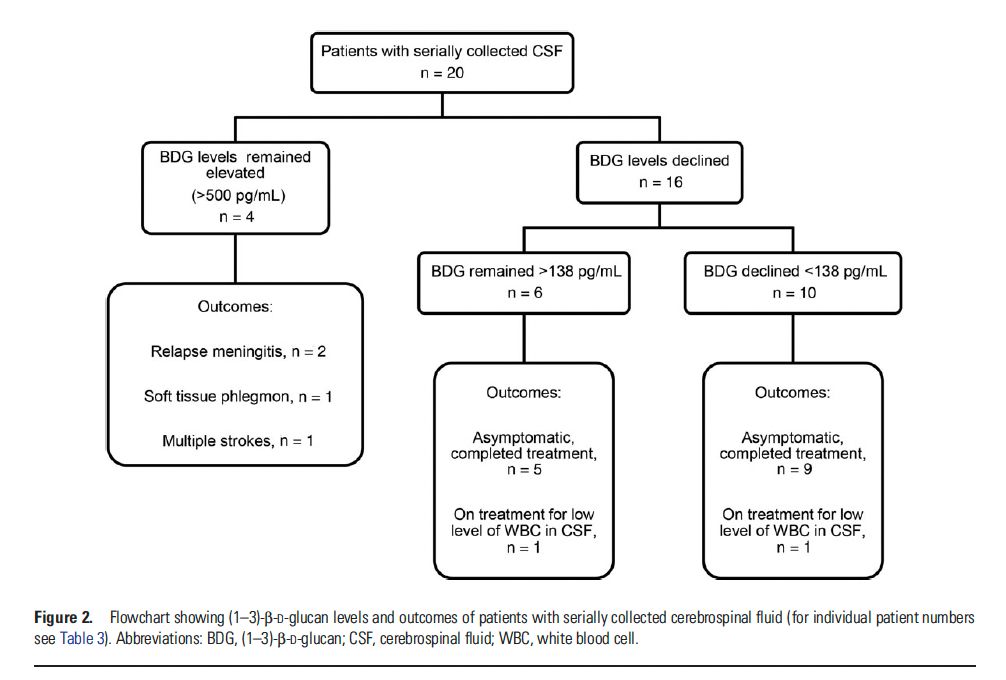
Indeed, even in those whose BD glucan was detectable 5 of them could stop therapy without recurrence of symptoms. Finally, a meta-analysis of 14 studies evaluated the utility of BD glucan off CSF in various fungal infections, including Cryptococcus, Coccidioides, Histoplasma, Aspergillus, Candida, and Exserohilum. I’ll focus on the molds for this post (Exserohilum and Aspergillus). In both organisms, the mean BD glucan levels are significantly higher in cases than in controls (383pg/mL vs 41pg/mL in Aspergillus, for instance) and yielded good sensitivity and specificity when certain cut-offs were defined:

Current Recommendations:
These have been published in the fungus education hub and supported by the CDC (22). Those who were exposed and have symptoms reminiscent of meningismus buy themselves an LP, with standard studies sent off the CSF, including BD glucan, galactomannan (which makes sense, considering other fungi have been described in the 2012 outbreak), bacterial, mycobacterial, and fungal cultures, opening pressure, and multiplex PCR (22). Those who have a CSF Wbc > 5 get empiric therapy with liposomal amphotericin B and voriconazole. This is similar to one opinion piece, which highlighted the combination of liposomal amphotericin B and voriconazole ata dose of 6mg/kg every 12 hours with a goal voriconazole trough of 2 to 5 mcg/mL (23). Analysis from E. rostrum samples of the 2012 outbreak demonstrated that all were susceptible to voriconazole (MIC 1 to 4 ug/mL), amphotericin B (MIC 0.03 to 2ug/mL), itraconazole (0.25 to 4ug/mL), and posaconazole (0.25 to ug/mL), while resistant to fluconazole (24). Despite these susceptibilities, voriconazole was chosen as the main drug due to its experience of use, the option to step down from IV to oral therapy, and high CSF levels. As a result, the recommendation evolved to start empiric voriconazole 6mg/kg twice per day with the option of adding liposomal amphotericin B for severe or refractory CNS disease. Target trough levels are 2 to 5 ug/mL, with therapy being 3 months in length for meningitis, with the recommendation of extending to 6 months in those who had localized spinal abscess or phlegmon, osteomyelitis, or vertebral discitis.
There are a lot of questions that remain, however, as this situation evolves. First, duration of therapy. I am assuming, given the prior data, it is likely a long-term deal with 3 to 6 months of therapy, however can monotherapy with voriconazole be used? And what to track? I suspect voriconazole can be used as step down with serial LPs being required prior to de-escalation to monotherapy. How long the therapy is depends on the procedures done (i.e if someone has an aneurysm, and they get clipped, do they get lifelong azoles? I think so) and the LP data. Further, the utility of azoles such as isavuconazole will be tested in this outbreak. Moreover, what does opening pressure management look like? Serial LPs, similar to cryptococcus, seem to be a must, however at what point does one put in an EVD? Finally, the question of when to angio is crucial. One study proposed the following algorithm to treating mycotic aneurysm (25):
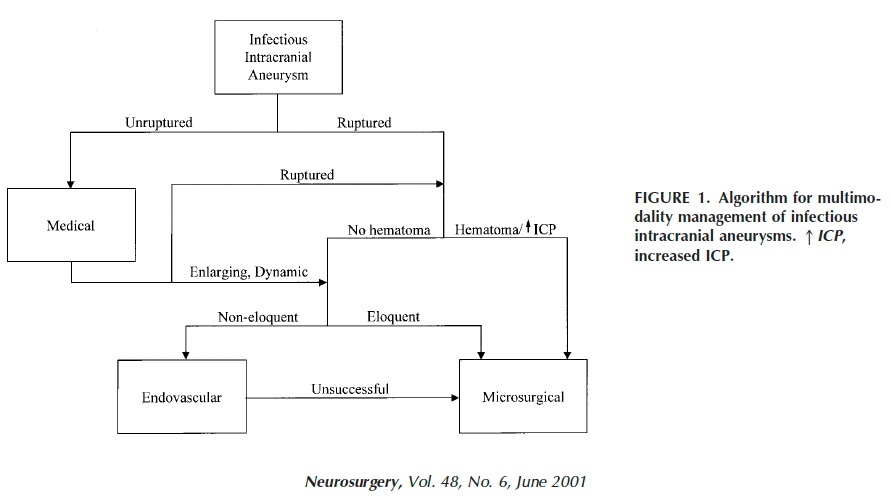
Many questions remains in this evolving outbreak, and I’ll update accordingly.
References:
- https://www.cdc.gov/hai/outbreaks/meningitis-epidural-anesthesia.html
- Arduino, Matthew J. et al. “Exophiala infection from contaminated injectable steroids prepared by a compounding pharmacy–United States, July-November 2002.” MMWR. Morbidity and mortality weekly report 51 49 (2002): 1109-12 .
- Ng TT, Robson GD, Denning DW. Hydrocortisone-enhanced growth of Aspergillus spp.: implications for pathogenesis. Microbiology (Reading). 1994 Sep;140 ( Pt 9):2475-9. doi: 10.1099/13500872-140-9-2475. PMID: 7952197.
- Pettit AC, Kropski JA, Castilho JL, Schmitz JE, Rauch CA, Mobley BC, Wang XJ, Spires SS, Pugh ME. The index case for the fungal meningitis outbreak in the United States. N Engl J Med. 2012 Nov 29;367(22):2119-25. doi: 10.1056/NEJMoa1212292. Epub 2012 Oct 19. PMID: 23083311.
- Kainer MA, Reagan DR, Nguyen DB, Wiese AD, Wise ME, Ward J, Park BJ, Kanago ML, Baumblatt J, Schaefer MK, Berger BE, Marder EP, Min JY, Dunn JR, Smith RM, Dreyzehner J, Jones TF; Tennessee Fungal Meningitis Investigation Team. Fungal infections associated with contaminated methylprednisolone in Tennessee. N Engl J Med. 2012 Dec 6;367(23):2194-203. doi: 10.1056/NEJMoa1212972. Epub 2012 Nov 6. PMID: 23131029; PMCID: PMC4669562.
- Kerkering TM, Grifasi ML, Baffoe-Bonnie AW, Bansal E, Garner DC, Smith JA, Demicco DD, Schleupner CJ, Aldoghaither RA, Savaliya VA. Early clinical observations in prospectively followed patients with fungal meningitis related to contaminated epidural steroid injections. Ann Intern Med. 2013 Feb 5;158(3):154-61. doi: 10.7326/0003-4819-158-3-201302050-00568. Erratum in: Ann Intern Med. 2013 Mar 19;158(6):504. Dosage error in article text. PMID: 23183583.
- Smith RM, Schaefer MK, Kainer MA, Wise M, Finks J, Duwve J, Fontaine E, Chu A, Carothers B, Reilly A, Fiedler J, Wiese AD, Feaster C, Gibson L, Griese S, Purfield A, Cleveland AA, Benedict K, Harris JR, Brandt ME, Blau D, Jernigan J, Weber JT, Park BJ; Multistate Fungal Infection Outbreak Response Team. Fungal infections associated with contaminated methylprednisolone injections. N Engl J Med. 2013 Oct 24;369(17):1598-609. doi: 10.1056/NEJMoa1213978. Epub 2012 Dec 19. PMID: 23252499.
- Chiller TM, Roy M, Nguyen D, Guh A, Malani AN, Latham R, Peglow S, Kerkering T, Kaufman D, McFadden J, Collins J, Kainer M, Duwve J, Trump D, Blackmore C, Tan C, Cleveland AA, MacCannell T, Muehlenbachs A, Zaki SR, Brandt ME, Jernigan JA; Multistate Fungal Infection Clinical Investigation Team. Clinical findings for fungal infections caused by methylprednisolone injections. N Engl J Med. 2013 Oct 24;369(17):1610-9. doi: 10.1056/NEJMoa1304879. PMID: 24152260.
- Kleinfeld K, Jones P, Riebau D, Beck A, Paueksakon P, Abel T, Claassen DO. Vascular complications of fungal meningitis attributed to injections of contaminated methylprednisolone acetate. JAMA Neurol. 2013 Sep 1;70(9):1173-6. doi: 10.1001/jamaneurol.2013.3586. PMID: 23877880; PMCID: PMC4143418.
- Ducruet AF, Hickman ZL, Zacharia BE, Narula R, Grobelny BT, Gorski J, Connolly ES Jr. Intracranial infectious aneurysms: a comprehensive review. Neurosurg Rev. 2010 Jan;33(1):37-46. doi: 10.1007/s10143-009-0233-1. Epub 2009 Oct 16. PMID: 19838745.
- Nakata Y, Shionoya S, Kamiya K. Pathogenesis of mycotic aneurysm. Angiology. 1968 Nov;19(10):593-601. doi: 10.1177/000331976801901003. PMID: 5695978.
- Lyons JL, Gireesh ED, Trivedi JB, Bell WR, Cettomai D, Smith BR, Karram S, Chang T, Tochen L, Zhang SX, McCall CM, Pearce DT, Carroll KC, Chen L, Ratchford JN, Harrison DM, Ostrow LW, Stevens RD. Fatal exserohilum meningitis and central nervous system vasculitis after cervical epidural methylprednisolone injection. Ann Intern Med. 2012 Dec 4;157(11):835-6. doi: 10.7326/0003-4819-158-1-201212040-00557. PMID: 23277893.
- Petraitiene R, Petraitis V, Hope WW, Mickiene D, Kelaher AM, Murray HA, Mya-San C, Hughes JE, Cotton MP, Bacher J, Walsh TJ. Cerebrospinal fluid and plasma (1–>3)-beta-D-glucan as surrogate markers for detection and monitoring of therapeutic response in experimental hematogenous Candida meningoencephalitis. Antimicrob Agents Chemother. 2008 Nov;52(11):4121-9. doi: 10.1128/AAC.00674-08. Epub 2008 Sep 8. PMID: 18779361; PMCID: PMC2573149.
- Mikulska M, Furfaro E, Del Bono V, Raiola AM, Di Grazia C, Bacigalupo A, Viscoli C. (1-3)-β-D-glucan in cerebrospinal fluid is useful for the diagnosis of central nervous system fungal infections. Clin Infect Dis. 2013 May;56(10):1511-2. doi: 10.1093/cid/cit073. Epub 2013 Feb 7. PMID: 23392391.
- Salvatore CM, Chen TK, Toussi SS, DeLaMora P, Petraitiene R, Finkelman MA, Walsh TJ. (1→3)-β-d-Glucan in Cerebrospinal Fluid as a Biomarker for Candida and Aspergillus Infections of the Central Nervous System in Pediatric Patients. J Pediatric Infect Dis Soc. 2016 Sep;5(3):277-86. doi: 10.1093/jpids/piv014. Epub 2015 Mar 19. PMID: 26407252; PMCID: PMC6281134.
- Lyons JL, Thakur KT, Lee R, Watkins T, Pardo CA, Carson KA, Markley B, Finkelman MA, Marr KA, Roos KL, Zhang SX. Utility of measuring (1,3)-β-d-glucan in cerebrospinal fluid for diagnosis of fungal central nervous system infection. J Clin Microbiol. 2015 Jan;53(1):319-22. doi: 10.1128/JCM.02301-14. Epub 2014 Nov 5. PMID: 25378578; PMCID: PMC4290946.
- Stevens DA, Zhang Y, Finkelman MA, Pappagianis D, Clemons KV, Martinez M. Cerebrospinal Fluid (1,3)-Beta-d-Glucan Testing Is Useful in Diagnosis of Coccidioidal Meningitis. J Clin Microbiol. 2016 Nov;54(11):2707-2710. doi: 10.1128/JCM.01224-16. Epub 2016 Aug 24. PMID: 27558179; PMCID: PMC5078547.
- Lyons JL, Roos KL, Marr KA, Neumann H, Trivedi JB, Kimbrough DJ, Steiner L, Thakur KT, Harrison DM, Zhang SX. Cerebrospinal fluid (1,3)-β-D-glucan detection as an aid for diagnosis of iatrogenic fungal meningitis. J Clin Microbiol. 2013 Apr;51(4):1285-7. doi: 10.1128/JCM.00061-13. Epub 2013 Jan 30. PMID: 23363831; PMCID: PMC3666821.
- Malani AN, Singal B, Wheat LJ, Al Sous O, Summons TA, Durkin MM, Pettit AC. (1,3)-β-d-glucan in cerebrospinal fluid for diagnosis of fungal meningitis associated with contaminated methylprednisolone injections. J Clin Microbiol. 2015 Mar;53(3):799-803. doi: 10.1128/JCM.02952-14. Epub 2014 Dec 24. PMID: 25540391; PMCID: PMC4390625.
- Litvintseva AP, Lindsley MD, Gade L, Smith R, Chiller T, Lyons JL, Thakur KT, Zhang SX, Grgurich DE, Kerkering TM, Brandt ME, Park BJ. Utility of (1-3)-β-D-glucan testing for diagnostics and monitoring response to treatment during the multistate outbreak of fungal meningitis and other infections. Clin Infect Dis. 2014 Mar;58(5):622-30. doi: 10.1093/cid/cit808. Epub 2013 Dec 12. PMID: 24336827; PMCID: PMC4047277.
- Davis C, Wheat LJ, Myint T, Boulware DR, Bahr NC. Efficacy of Cerebrospinal Fluid Beta-d-Glucan Diagnostic Testing for Fungal Meningitis: a Systematic Review. J Clin Microbiol. 2020 Mar 25;58(4):e02094-19. doi: 10.1128/JCM.02094-19. PMID: 31996446; PMCID: PMC7098769.
- https://funguseducationhub.org/wp-content/uploads/2023/05/interim-guidance-Matamoros-FM-outbreak-5_23_23_posting-version.pdf
- Shoham S, Marr KA. Treatment of iatrogenic fungal infections: a black mold defines a new gray zone in medicine. Ann Intern Med. 2013 Feb 5;158(3):208-10. doi: 10.7326/0003-4819-158-3-201302050-00572. PMID: 23147215; PMCID: PMC4696024.
- Kauffman CA, Pappas PG, Patterson TF. Fungal infections associated with contaminated methylprednisolone injections. N Engl J Med. 2013 Jun 27;368(26):2495-500. doi: 10.1056/NEJMra1212617. Epub 2012 Oct 19. PMID: 23083312.
- Chun JY, Smith W, Halbach VV, Higashida RT, Wilson CB, Lawton MT. Current multimodality management of infectious intracranial aneurysms. Neurosurgery. 2001 Jun;48(6):1203-13; discussion 1213-4. doi: 10.1097/00006123-200106000-00001. PMID: 11383721.
