
Echinocandins. This is the drug we use mostly on the inpatient side for invasive candidiasis. The most well known is micafungin, but analdafungin is another option that is also commonly used. Besides resistance, the issue with echinocandins are the fact they are intravenous drugs, which makes administration of it easy on the inpatient side but difficult on the outpatient side without a PICC line and a functional OPAT program. If you strike luck and the organism is susceptible to fluconazole, then you can use that. The utility of other tri-azoles is unknown. One randomized trial compared a cohort of 400 patients with invasive candidemia treated with voriconazole (either oral or IV) or amphotericin B IV with fluconazole step down (1). There was no difference in the primary endpoint of 12 week mortality. Moreover, roughly around 50% of those in the voriconazole group had a serious adverse event, the most common being transaminitis. A similar multicenter, randomized, non-inferiority trial compared caspofungin with oral voriconazole stepdow to isavuconazole IV with oral isavuconazole step down in invasive candidiasis and found that voriconazole did not reach its non-inferiority margin for the primary outcome of clinical or mycological response (adjusted difference -10.8, 95% CI -19 to -1.8, 2). Ideally, we could use these for outpatient therapy however the lack of data makes it difficult to argue for its use despite its high bioavailability. Enter, rezafungin.
Echinocandins are non-competitive inhibitors of the beta-1-3-D glucan synthase, which inhibit said structure, a major component of the fungal wall. Given this target, and the lack of said target in mammals (read: humans), we can use it with little toxicity. Rezafungin is able to do this by its structure. While I am not a fan of biochemistry, I will still show the structure (3).
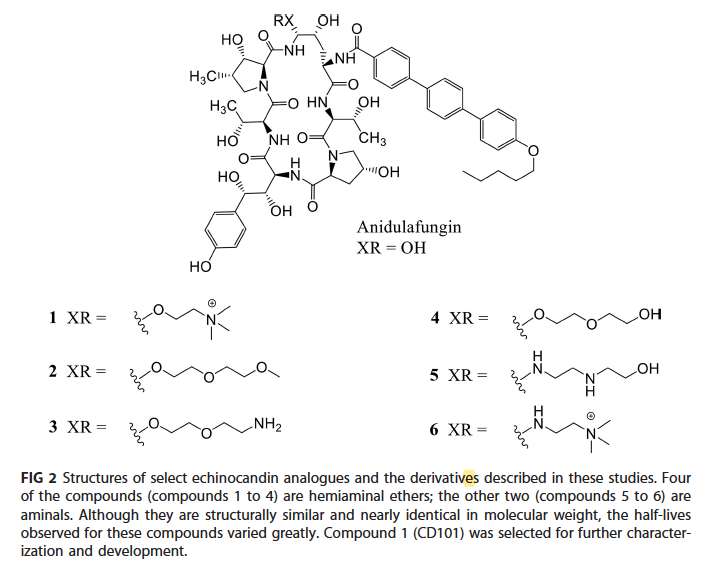
A study found the structure-activity relationship favored rezafunginin. When compared to experimental structures and anildafungin, half-life for rezafungin was higher and had the lowest volume of distribution and slower clearance. An animal study showed that rezafungin was highly protein bound, similarly to anidulafungin (98%, 4). Further, it did not inhibit CYP450 and did not show hepatotoxicity in an animal model.
In vitro data suggests similar coverage to that of other echinocandins. Epidemiological studies have evaluated clinical breakpoints against worldwide fungal isolates. A total of 1679 samples of various fungal species from 2019 to 2020 were evaluated (5). The susceptibility using the new CLSI breakpoints was high against candida albicans (100%), C. tropicalis (100%), C. glabrata (98.3%), C. krusei (100%), C. dubliniensis (100%), C. parapsilosis (99.6%). Most of the studies strains had similar profiles to comparator echinocandins (see the table at the end of the post for further details):

Rezafungin was found to have no activity against cryptococcus neoformans, however it had favorable activity against aspergillus fumigatus and A. flavi:
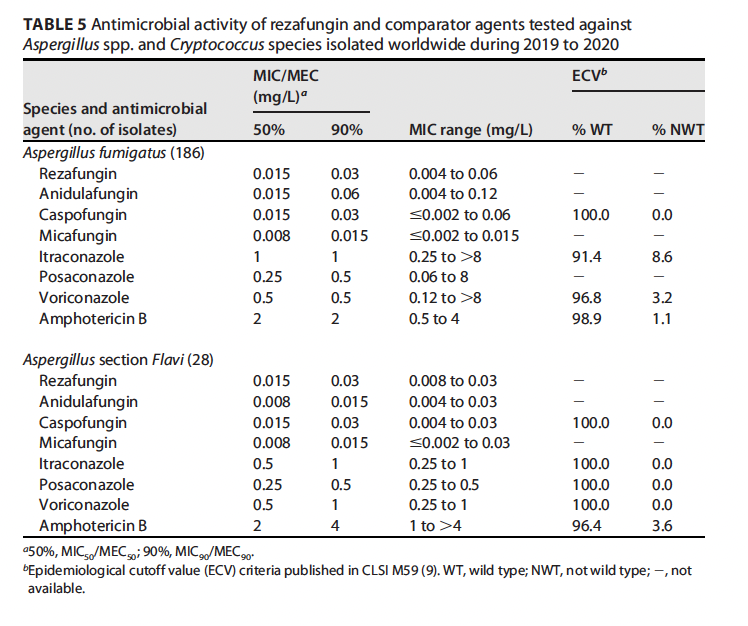
One thing to note is that strains harboring the 1-3 beta-d-glucan synthetase mutation (aka FKS1 or FKS2) had increased the MIC to all echinocandins, including rezafungin however the clinical implications of this are unknown:

Similarly, SENTRY data suggests rezafungin had activity against C. albicans, C. tropicalis, and C. krusei and least active against C. parapsilosis (6). Similarly, it had activity against A. fumigatus and A. flavus, comparable to that of other echinocandins:

Not surprisingly, it was inactive against Cryptococcus.
Pharmacokinetic Data
Several early trials have demonstrated the long half-life of rezafungin. One phase 1 randomized trial of 44 patients found the median time to max concentration was around 144 hours, with a median half life of around 193 hours (7):
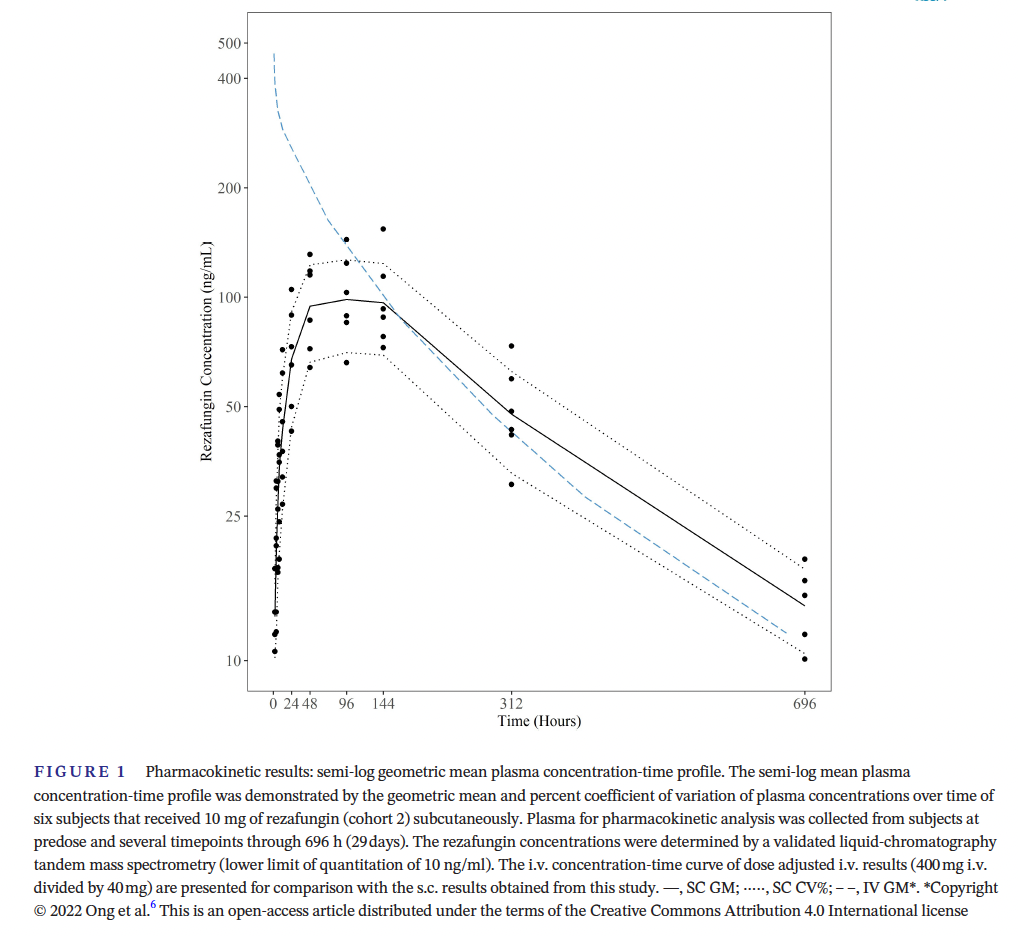
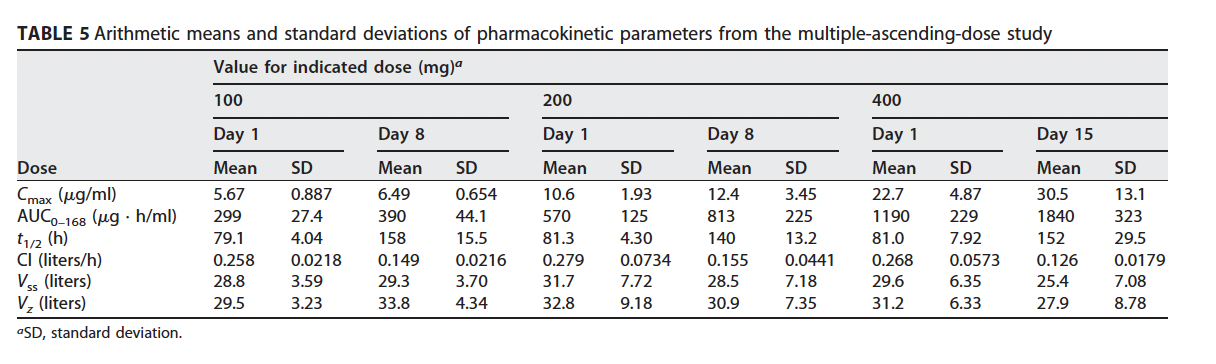
Notably, in 5 of 6 subjects, rezafungin was detected up to day 30. One interesting pharmacokinetic study evaluated single-ascending doses (50mg, 100mg, 200mg, and 400mg) and multiple-ascending doses (100mg for 2 doses, 200mg for 2 doses, 400mg for 3 doses) separated by 7 days each dose (8). Plasma concentrations were found to be higher on day 8 in the first 2 cohorts and day 15 in the third cohort of the multiple-ascending doses when compared to day 1. Moreover, the AUC was higher on day 8 in the first 2 cohorts and day 15 in the third cohort, suggesting a cumulative effect:
A neutropenic mouse model found rezafungin displayed dose-dependent activity, with potency at high doses against C. albicans and C. glabrata, and less so against C. parapsilosis (9):

Clinical Data
Few large trials have looked at the utility of rezafungin. The first trial, the STRIVE study, was a phase 2, double-blind, randomized, double-dummy, multicenter trial across 10 countries (10). Here, 2 parts were performed; the first one had patients being randomized in a 1:1:1 fashion to received rezafungin weekly for 2-4 weeks at either 400mg (group 1), 400mg on week 1 followed by 200mg thereafter (group 2), or caspofungin daily (group 3). Part b had patients randomized in 2:1 fashion to rezafungin;caspofungin. After review, dosing for rezafungin was modified to 400mg on week one followed by 200mg weekly. Primary endpoint was overall response defined as resolution of clinical signs of candidemia/candidiasis and mycological eradication at day 14. 207 patients were randomized, with both groups being fairly well balanced; however, those in the rezafungin group seemed to be sicker as they tended to have more patients with APACHE scores >20 but the overall mean was the same. Most species were of albicans (~50%), followed by glabrata (20.2%), and parapsilosis (15%). At the end of the study period, there was no difference in outcomes between groups and rezafungin met non-inferiority criteria, though those in the rezafungin group had numerically higher rates of cure:
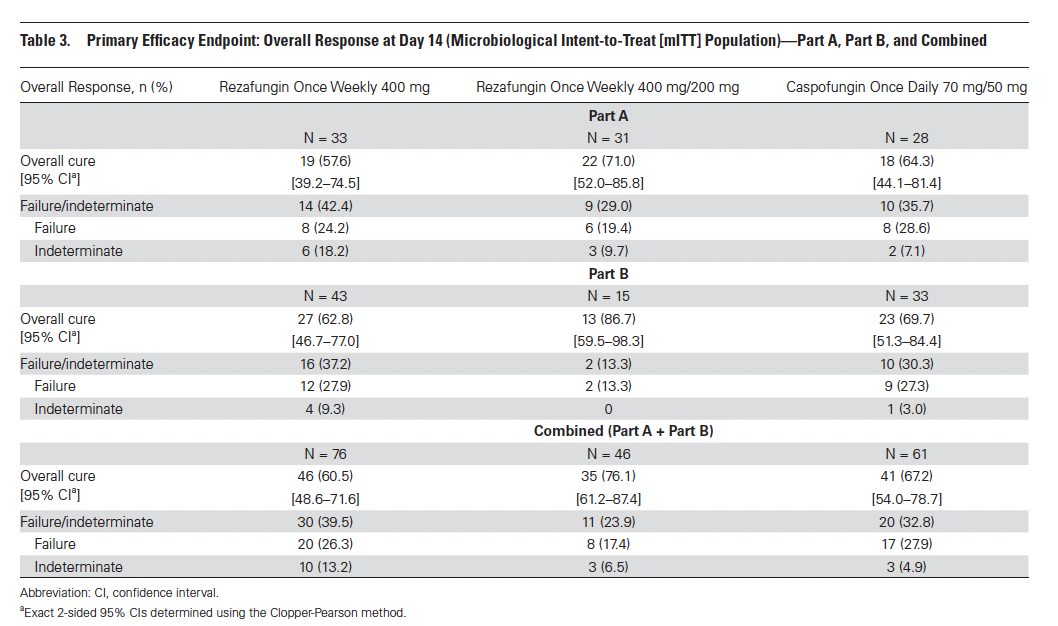


Surprisingly, the percentage of patients cured in the 400/200 regimen was higher than the 400mg weekly regimen of rezafungin. Adverse events were similar in both cohorts:

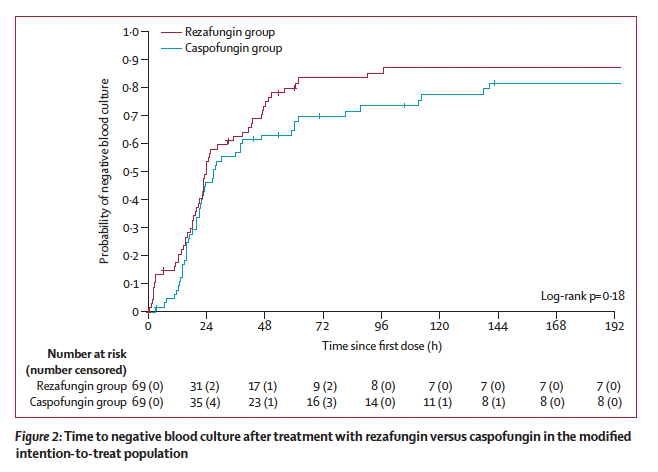
In a similar trial, rezafungin and caspofungin were compared in patients with invasive candidiasis or candidemia without osteomyelitis or endocarditis (11). 199 patients were randomized in a 1:1 fashion to either rezafungin (400mg on week one and 200mg weekly thereafter) or caspofungin in this multicenter, prospective, double-blind, non-inferiority trial. Patients in the caspofungin arm could be de-escalated to oral fluconazole therapy while those in the rezafungin could receive placebo after 3 days of therapy. Two primary outcomes were evaluated; first was global culture at day 14 and the second was all-cause of mortality up to day 30. Overall, both groups were balanced, with the most common candida isolate being albicans with over 99% of isolates being susceptible to both agents. At the end of the trial period, rezafungin met non-inferiority margin in both primary outcomes:


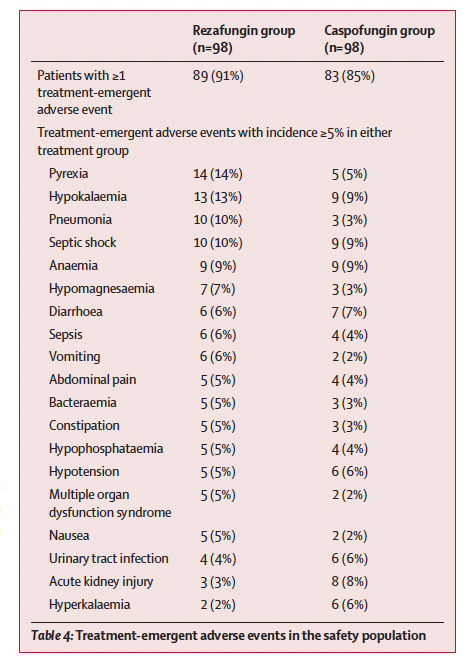
Moreover, adverse events were numerically higher in the rezfungin group (91% vs 85%):
One small trial compared the utility of topical rezafungin to topical fluconazole for vulvovaginitis (12). 126 women were enrolled, and randomized in one of three groups: 1) 3% gel applied vaginally on days 1 and 2; 2) 6% ointment applied on day 1 and 3) oral fluconazole for one day. Primary outcome was clinical and mycological cure at day 28. At the end of the trial period, the rates of clinical cure were 35%, 30%, and 52.6%, respectively. Mycological cure was 45%, 40%, and 57.9%, respectively.
Overall, it appears rezafungin will be used for complicated invasive candidiasis, where fluconazole cannot be used.
TABLE:

References:
- Kullberg BJ, Sobel JD, Ruhnke M, Pappas PG, Viscoli C, Rex JH, Cleary JD, Rubinstein E, Church LW, Brown JM, Schlamm HT, Oborska IT, Hilton F, Hodges MR. Voriconazole versus a regimen of amphotericin B followed by fluconazole for candidaemia in non-neutropenic patients: a randomised non-inferiority trial. Lancet. 2005 Oct 22-28;366(9495):1435-42. doi: 10.1016/S0140-6736(05)67490-9. PMID: 16243088.
- Kullberg BJ, Viscoli C, Pappas PG, Vazquez J, Ostrosky-Zeichner L, Rotstein C, Sobel JD, Herbrecht R, Rahav G, Jaruratanasirikul S, Chetchotisakd P, Van Wijngaerden E, De Waele J, Lademacher C, Engelhardt M, Kovanda L, Croos-Dabrera R, Fredericks C, Thompson GR. Isavuconazole Versus Caspofungin in the Treatment of Candidemia and Other Invasive Candida Infections: The ACTIVE Trial. Clin Infect Dis. 2019 May 30;68(12):1981-1989. doi: 10.1093/cid/ciy827. PMID: 30289478.
- James KD, Laudeman CP, Malkar NB, Krishnan R, Polowy K. Structure-Activity Relationships of a Series of Echinocandins and the Discovery of CD101, a Highly Stable and Soluble Echinocandin with Distinctive Pharmacokinetic Properties. Antimicrob Agents Chemother. 2017 Jan 24;61(2):e01541-16. doi: 10.1128/AAC.01541-16. PMID: 27919891; PMCID: PMC5278707.
- Ong V, Hough G, Schlosser M, Bartizal K, Balkovec JM, James KD, Krishnan BR. Preclinical Evaluation of the Stability, Safety, and Efficacy of CD101, a Novel Echinocandin. Antimicrob Agents Chemother. 2016 Oct 21;60(11):6872-6879. doi: 10.1128/AAC.00701-16. PMID: 27620474; PMCID: PMC5075098.
- Carvalhaes CG, Klauer AL, Rhomberg PR, Pfaller MA, Castanheira M. Evaluation of Rezafungin Provisional CLSI Clinical Breakpoints and Epidemiological Cutoff Values Tested against a Worldwide Collection of Contemporaneous Invasive Fungal Isolates (2019 to 2020). J Clin Microbiol. 2022 Apr 20;60(4):e0244921. doi: 10.1128/jcm.02449-21. Epub 2022 Mar 7. PMID: 35249367; PMCID: PMC9020363.
- Pfaller MA, Carvalhaes C, Messer SA, Rhomberg PR, Castanheira M. Activity of a Long-Acting Echinocandin, Rezafungin, and Comparator Antifungal Agents Tested against Contemporary Invasive Fungal Isolates (SENTRY Program, 2016 to 2018). Antimicrob Agents Chemother. 2020 Mar 24;64(4):e00099-20. doi: 10.1128/AAC.00099-20. PMID: 32015043; PMCID: PMC7179261.
- Gu K, Ruff D, Key C, Thompson M, Jiang S, Sandison T, Flanagan S. A phase I randomized, double-blind, single subcutaneous dose escalation study to determine the safety, tolerability, and pharmacokinetics of rezafungin in healthy adult subjects. Clin Transl Sci. 2022 Jul;15(7):1592-1598. doi: 10.1111/cts.13286. Epub 2022 May 4. PMID: 35439347; PMCID: PMC9283735.
- Sandison T, Ong V, Lee J, Thye D. Safety and Pharmacokinetics of CD101 IV, a Novel Echinocandin, in Healthy Adults. Antimicrob Agents Chemother. 2017 Jan 24;61(2):e01627-16. doi: 10.1128/AAC.01627-16. PMID: 27919901; PMCID: PMC5278714.
- Lepak AJ, Zhao M, VanScoy B, Ambrose PG, Andes DR. Pharmacodynamics of a Long-Acting Echinocandin, CD101, in a Neutropenic Invasive-Candidiasis Murine Model Using an Extended-Interval Dosing Design. Antimicrob Agents Chemother. 2018 Jan 25;62(2):e02154-17. doi: 10.1128/AAC.02154-17. PMID: 29203480; PMCID: PMC5786781.
- Thompson GR, Soriano A, Skoutelis A, Vazquez JA, Honore PM, Horcajada JP, Spapen H, Bassetti M, Ostrosky-Zeichner L, Das AF, Viani RM, Sandison T, Pappas PG. Rezafungin Versus Caspofungin in a Phase 2, Randomized, Double-blind Study for the Treatment of Candidemia and Invasive Candidiasis: The STRIVE Trial. Clin Infect Dis. 2021 Dec 6;73(11):e3647-e3655. doi: 10.1093/cid/ciaa1380. Erratum in: Clin Infect Dis. 2021 Aug 2;73(3):561-562. PMID: 32955088; PMCID: PMC8662762.
- Thompson GR 3rd, Soriano A, Cornely OA, Kullberg BJ, Kollef M, Vazquez J, Honore PM, Bassetti M, Pullman J, Chayakulkeeree M, Poromanski I, Dignani C, Das AF, Sandison T, Pappas PG; ReSTORE trial investigators. Rezafungin versus caspofungin for treatment of candidaemia and invasive candidiasis (ReSTORE): a multicentre, double-blind, double-dummy, randomised phase 3 trial. Lancet. 2023 Jan 7;401(10370):49-59. doi: 10.1016/S0140-6736(22)02324-8. Epub 2022 Nov 25. PMID: 36442484.
- Nyirjesy P, Alessio C, Jandourek A, Lee JD, Sandison T, Sobel JD. CD101 Topical Compared With Oral Fluconazole for Acute Vulvovaginal Candidiasis: A Randomized Controlled Trial. J Low Genit Tract Dis. 2019 Jul;23(3):226-229. doi: 10.1097/LGT.0000000000000473. PMID: 30893271.
