
At the end of the 19th Century, the British hospital in Valletta, housed in the Hospital of the Knights (which had the longest ward in Europe), was full of soldiers ill with the disease, many of whom are invalided to Britain. Nearly half were discharged because of complications of arthritis and their pensions were a serious drain on the British Treasury. Bruce, now a Colonel and a Fellow of the Royal Society, continued to press for research into the disease and in 1904 he was appointed to head the MFC with four researchers – with typical economy, no new salaries were necessary.
This is a description from an interesting historical paper (1) that highlights the discovery of the etiology of Brucellosis. Originally known as “Malta fever” and “Mediterranean fever,” Brucellosis is inherently a systemic disease with what the literature describes as “protean” manifestations i.e. it has a lot of different ways it can show up. Along with tuberculosis and syphilis, it is known as the “great mimicker” due to the number of diseases it can imitate. As you can glean from the quote, I’ll be focusing on a more mundane presentation: sacroiliitis. I won’t talk much about diagnosis, but the presentation is actually interesting.
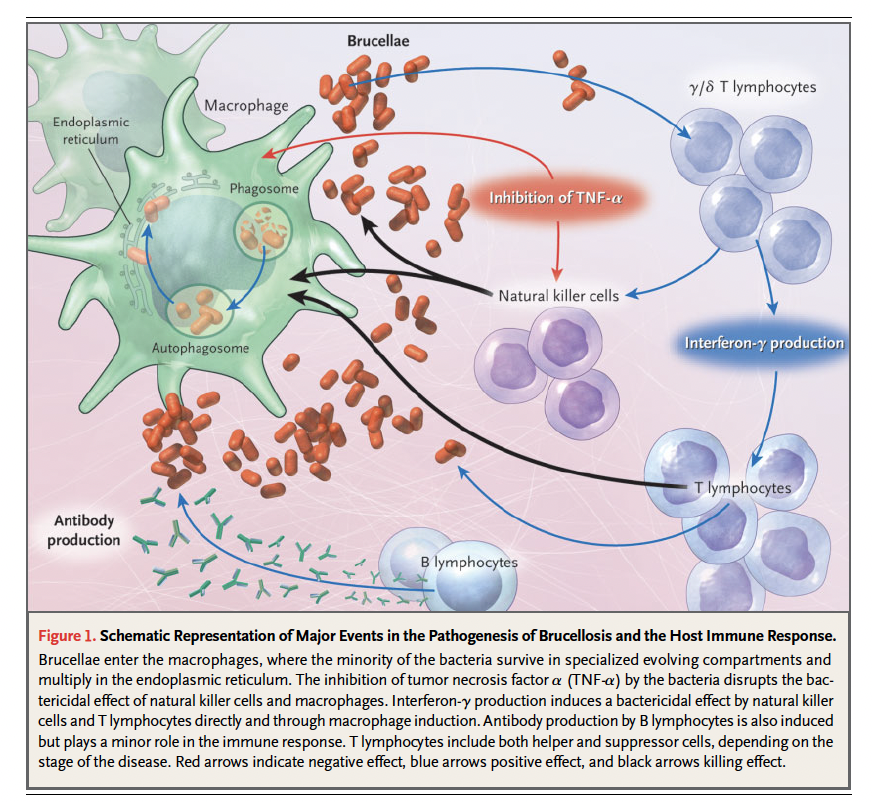
The organism that was named after David Bruce, are small, gram negative, non-spore forming, intracellular coccobacilli (2). It is a type of alpha-2 subdivision proteobacteria that include bartonella and rickettsia, which tend to be intracellular (3). Four are known to cause human disease: Brucella abortus, B. melitensis, B. suis, and B. canis. The bacteria can survive up to 6 weeks at 4oC in cream, 30 days in ice cream, and 15 to 100 days in fresh cheese. Lactic acid fermentation as well as heat kills the bacteria. One of the characteristics of this organism is that it does not bear the classic virulence factors such as exotoxins or endotoxins. How does it provide its pathogenicity? Phagocytosis by non-professional phagocytes, or something (3). After internalization, brucella bacteria are killed by phagolysosome fusion, of which only 15 to 30 percent of bacteria survive. They do this by setting up specialized compartments within the cellular machinery. The bacteria then survive and replicate in the endoplasmic reticulum. From here, TNF-alpha and IFN-gamma are both inhibited, which leads to the proliferation of bacteria.
Transmission is a well known characteristic of the disease. Indeed, laboratory exposure was a concern from back in the original Bruce days (1), with many people who studied the illness falling ill after working with it. Transmission to humans occurs through consumption of infected, unpasteurized animal-milk products, through direct contact with infected parts, and through inhalation of aerosolized particles. Indeed, the notorious Unit 731 (WW2 imperial Japan put together to perform biological and chemical warfare research) looked at Brucella as one of their targets for biological weapons (4). This can be consumed or inhaled, usually through unpasteurized animal-milk products, direct contact with infected parts, and through inhalation of released animal products,, making it a fairly good agent for biological warfare. The incubation period ranges from 9 days up to 60 days (2, 4).
Vertebral Brucellosis
As mentioned previously, the manifestations of Brucellosis tend to be described as “protean.” Fevers, rigors, and malodorous perspiration are commonly described manifestations. Osteoarticular disease is the most common manifestation of brucellosis – peripheral arthritis, sacroiliitis, and spondylitis, however a range of disease has been described, including epididymo-orchitis, endocarditis, myocarditis, peritonitis, and CNS symptoms. Multiple case reports have described young patients with unilateral sciatica, low-grade fever, a positive straight leg raise test, and morning stiffness who end up having Brucellosis (5-7).
Given the long history of the disease, multiple large cohorts describing osteoarticular manifestations are available for our reading pleasure. A series of 62 cases with sacroiliitis found 7 were infected due to occupational exposure and 42 were infected due to consumption of dairy products (14). Fevers, chills, malaise, and arthralgias were common findings:
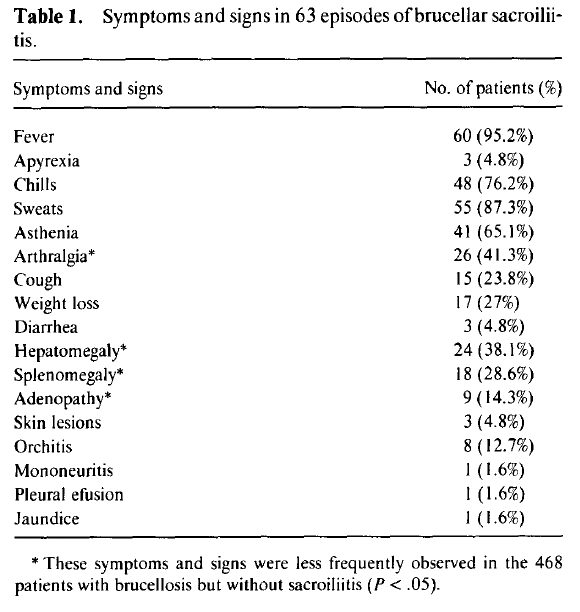
Of those with sacroiliitis, only 16% had bilateral involvement. Only 4 patients had clinical failure, and radiographic evidence of sacroiliitis was vast on plain film:

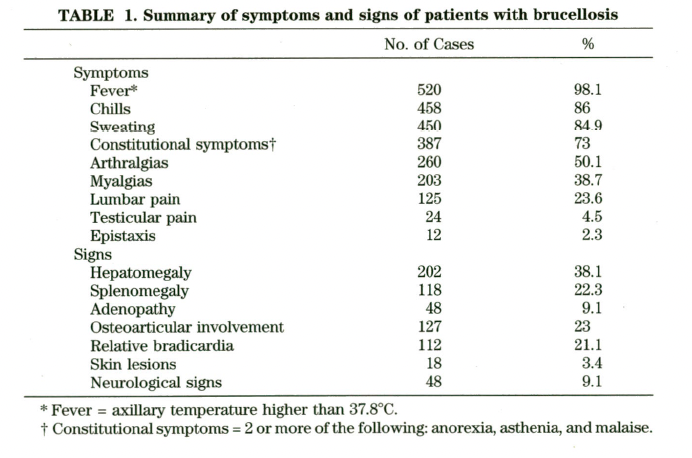
A Peruvian cohort of 304 patients with joint involvement similarly found that fever and malaise were the most prevalent symptoms, however hepatomegaly was also fairly common (8):

Sacroiliitis was the most common articular manifestation, which tended to be unilateral and most cases were acute:
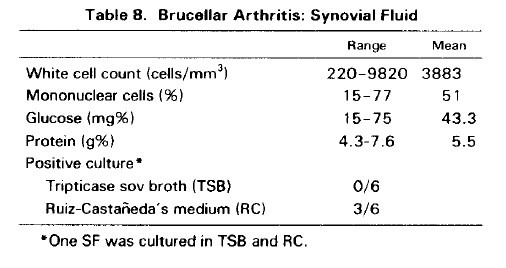
One interesting bit here is that 13 patients had synovial fluid analysis. WBC ranged from 220 to 9820 cells, with cell count ranging from 15% to 77%. A cohort of 452 patients with brucellosis described osteoarticular complications occurring in 169 of these (9). 88% had consumed raw milk and its products or had close contact with animals. These patients were divided into three different subgroups; subgroup 1 had blood cultures positive with Brucella; subgroup 2 had a fourfold rise in antibody titers; and subgroup 3 had consistently high titers. Half of these patients had been ill for less than 2 weeks while for 8%, it lasted longer than 13 weeks (with up to 104 weeks in one subject). The main symptoms included fevers, sweats, and backache:

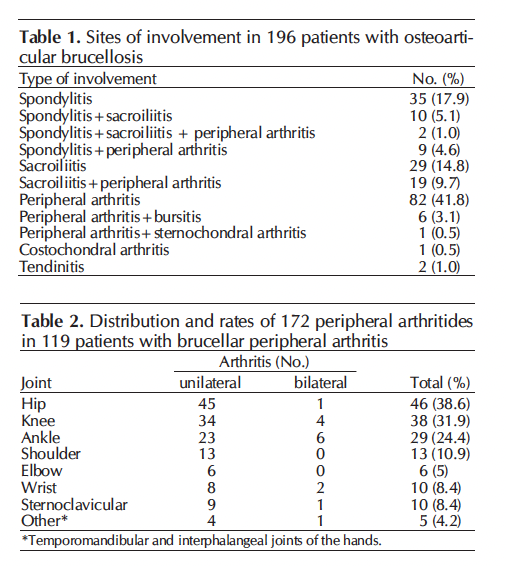
Notably, splenomegaly, hepatosplenomegaly, and lymphadenopathy was also found in a significant percentage of patients with osteoarticular complications. Moreover, gastrointestinal discomfort and anorexia were also reported in this cohort. Hips, spondylitis, knee, ankle, and sacroiliac joints were the most commonly involved joints:

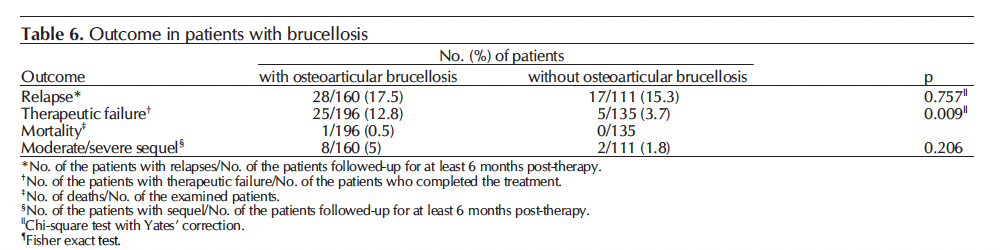
Moreover, dual therapy seems to lead to less incidence of relapse when compared to monotherapy:

In a cohort of 418 consecutive patients with brucellosis, 60% accounted for occupational exposures while 21.5% of them had dietary exposure (10). Within this cohort, the most common presentation was osteoarticular brucellosis, with most having a favorable response:


Most of these patients had combination therapy, usually involving a tetracycline and rifampin:

A cohort of 195 patients with MSK involvement found that 108 patients had sacroiliac involvement, usually unilateral in most cases (11). Major symptoms included arthralgia, chills, sweating, fevers, malaise, and headache:

Notably, most patients who are adults tended to have axial involvement compared to peripheral arthritis:

A cohort of 331 patients with Brucellosis evaluated the frequency of osteoarticular brucellosis (12). WIthin this cohort, 196 had osteoarticular manifestations, followed by hepatic (32.9%), genitourinary (11.2%), hematological (9.1%), and pulmonary (6%). Within this, most had peripheral arthritis, followed by sacroiliitis:
When comparing both cohorts, those in the osteoarticular cohort were more likely to have malaise, arthralgia, or weight loss at least numerically:

A review of 115 cases of Brucellosis in pediatric patients found that most common symptoms included fever, arthralgia/arthritis, hepatomegaly and splenomegaly (13):

The most commonly involved joints included the hip (40.8%), knee (39.7%), ankle (10.7%), elbow (4.3%), sacroiliac (3.2%) and wrist (1%) joints.
530 patients with vertebral brucellosis found that 70% were male, and 30% had a professional risk of acquiring infection (15). Most symptoms include fevers, chills, arthralgias, and constitutional symptoms:
Of these, 169 had focal illness, with median time to diagnosis being around 39 days. Most were osteoarticular disease, with 48 having unilateral sacroiliitis. Of those with sacroiliitis, 32 had abnormal plain radiographic studies and synovial fluid analysis had a cell count ranging from 5690 to 23200.

The largest cohort of 1028 patients with brucellosis found that roughly half of them had some occupational risk of brucellosis, with 61% being described as acute brucellosis (16). Most common symptoms included arthralgia (73%), fever (72%), and fatigue (71%). Findings included splenomegaly and hepatomegaly. Within this cohort, the majority of focal cases were osteoarticular making up 260 cases (25%):


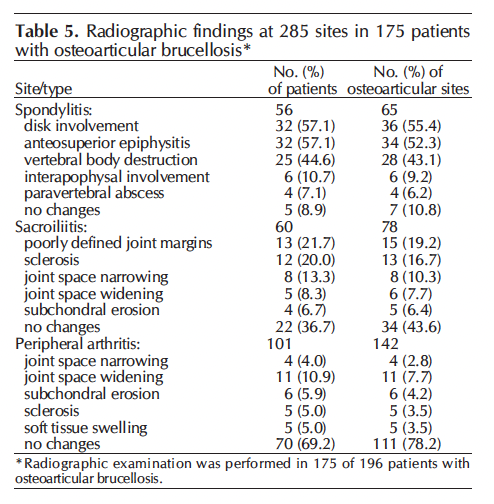
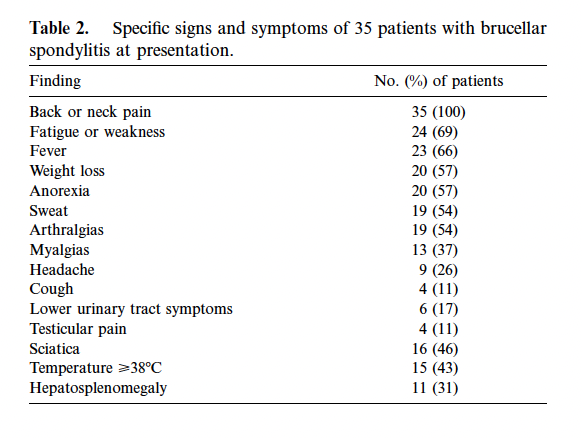
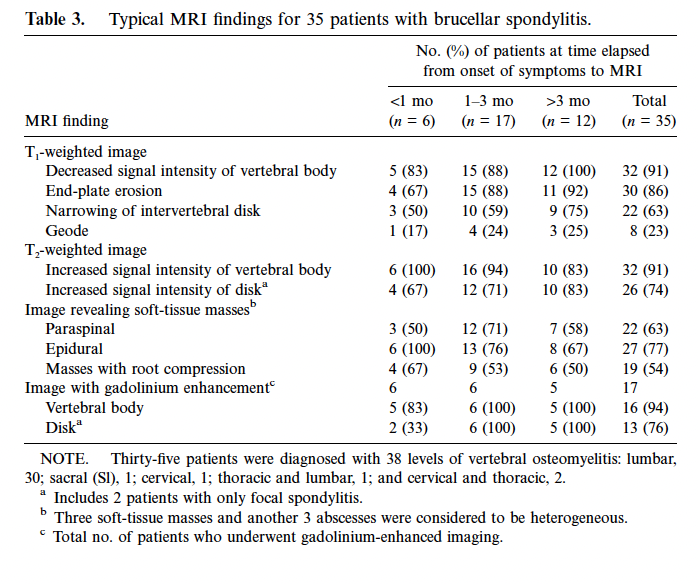
A retrospective cohort of 35 patients with brucellar spondylitis provides the most comprehensive description of the disease (17). These were divided into three groups; those who recovered, those who failed therapy, and those who relapsed. A total of 285 patients were evaluated, of which 35 had spondylitis. Those with spondylitis tended to be older, have longer duration of symptoms, and have a higher ESR. all patients had some sort of symptoms, with the most common being back pain, fatigue, and fever:
In MRI studies, 32 of the 35 were found to have single spinal region involvement; 3 had non-contiguous multifocal spinal involvement, and 31 had diffuse disease.
21 patients who received antibiotic therapy had recovered, with 9 being failures and 5 suffering from relapse.
A retrospective cohort of 96 patients with vertebral osteomyelitis found that the lumbar spine was most often involved and imaging findings in the disk and vertebral bodies (18):

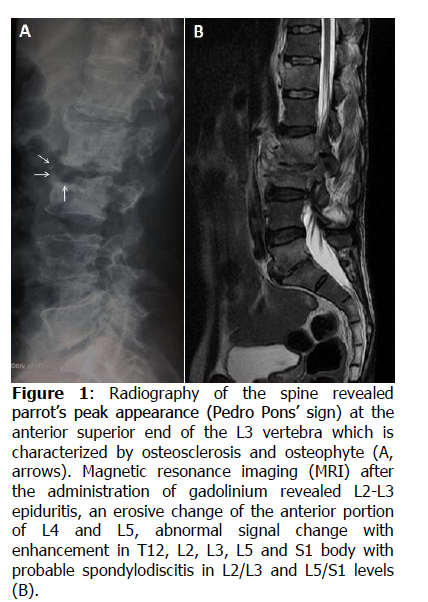
Notably, osteolysis of the vertebral body was involved anteriorly in nearly half of the cases. This erosion of the superior anterior plate into a parrot peak appearance is known as the “Pedro Pons” sign and it is pathognomonic for brucellosis (19):
References:
- Wyatt HV. Lessons from the history of brucellosis. Rev Sci Tech. 2013 Apr;32(1):17-25. doi: 10.20506/rst.32.1.2181. PMID: 23837362.
- Bennett, J. E., Dolin, R., & Blaser, M. J. (2014). Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Elsevier Inc.
- Pappas G, Akritidis N, Bosilkovski M, Tsianos E. Brucellosis. N Engl J Med. 2005 Jun 2;352(22):2325-36. doi: 10.1056/NEJMra050570. PMID: 15930423.
- Pappas G, Panagopoulou P, Christou L, Akritidis N. Brucella as a biological weapon. Cell Mol Life Sci. 2006 Oct;63(19-20):2229-36. doi: 10.1007/s00018-006-6311-4. PMID: 16964579.
- Gupta A, Shyam AM, Sancheti PK, Aiyer SN. Brucellosis sacroiliitis masquerading as inflammatory spondyloarthropathy. Indian Spine J 2022;5:241-5
- Ozgül A, Yazicioğlu K, Gündüz S, Kalyon TA, Arpacioğlu O. Acute brucella sacroiliitis: clinical features. Clin Rheumatol. 1998;17(6):521-3. doi: 10.1007/BF01451292. PMID: 9890684.
- Priest JR, Low D, Wang C, Bush T. Brucellosis and sacroiliitis: a common presentation of an uncommon pathogen. J Am Board Fam Med. 2008 Mar-Apr;21(2):158-61. doi: 10.3122/jabfm.2008.02.070170. PMID: 18343865
- Gotuzzo E, Alarcón GS, Bocanegra TS, Carrillo C, Guerra JC, Rolando I, Espinoza LR. Articular involvement in human brucellosis: a retrospective analysis of 304 cases. Semin Arthritis Rheum. 1982 Nov;12(2):245-55. doi: 10.1016/0049-0172(82)90064-6. PMID: 6101216.
- Mousa AR, Muhtaseb SA, Almudallal DS, Khodeir SM, Marafie AA. Osteoarticular complications of brucellosis: a study of 169 cases. Rev Infect Dis. 1987 May-Jun;9(3):531-43. doi: 10.1093/clinids/9.3.531. PMID: 3496650.
- Bosilkovski M, Krteva L, Dimzova M, Kondova I. Brucellosis in 418 patients from the Balkan Peninsula: exposure-related differences in clinical manifestations, laboratory test results, and therapy outcome. Int J Infect Dis. 2007 Jul;11(4):342-7. doi: 10.1016/j.ijid.2006.10.002. Epub 2007 Jan 22. PMID: 17241808.
- Geyik MF, Gür A, Nas K, Cevik R, Saraç J, Dikici B, Ayaz C. Musculoskeletal involvement of brucellosis in different age groups: a study of 195 cases. Swiss Med Wkly. 2002 Feb 23;132(7-8):98-105. doi: 10.57187/smw.2002.09900. PMID: 11971204.’
- Bosilkovski M, Krteva L, Caparoska S, Dimzova M. Osteoarticular involvement in brucellosis: study of 196 cases in the Republic of Macedonia. Croat Med J. 2004 Dec;45(6):727-33. PMID: 15578807.
- Shaalan MA, Memish ZA, Mahmoud SA, Alomari A, Khan MY, Almuneef M, Alalola S. Brucellosis in children: clinical observations in 115 cases. Int J Infect Dis. 2002 Sep;6(3):182-6. doi: 10.1016/s1201-9712(02)90108-6. PMID: 12718832.
- Ariza J, Pujol M, Valverde J, Nolla JM, Rufí G, Viladrich PF, Corredoira JM, Gudiol F. Brucellar sacroiliitis: findings in 63 episodes and current relevance. Clin Infect Dis. 1993 Jun;16(6):761-5. doi: 10.1093/clind/16.6.761. PMID: 8329507.
- Colmenero JD, Reguera JM, Martos F, Sánchez-De-Mora D, Delgado M, Causse M, Martín-Farfán A, Juárez C. Complications associated with Brucella melitensis infection: a study of 530 cases. Medicine (Baltimore). 1996 Jul;75(4):195-211. doi: 10.1097/00005792-199607000-00003. Erratum in: Medicine (Baltimore) 1997 Mar;76(2):139. PMID: 8699960.
- Buzgan T, Karahocagil MK, Irmak H, Baran AI, Karsen H, Evirgen O, Akdeniz H. Clinical manifestations and complications in 1028 cases of brucellosis: a retrospective evaluation and review of the literature. Int J Infect Dis. 2010 Jun;14(6):e469-78. doi: 10.1016/j.ijid.2009.06.031. Epub 2009 Nov 11. PMID: 19910232.
- Solera J, Lozano E, Martínez-Alfaro E, Espinosa A, Castillejos ML, Abad L. Brucellar spondylitis: review of 35 cases and literature survey. Clin Infect Dis. 1999 Dec;29(6):1440-9. doi: 10.1086/313524. PMID: 10585793.
- Colmenero JD, Ruiz-Mesa JD, Plata A, Bermúdez P, Martín-Rico P, Queipo-Ortuño MI, Reguera JM. Clinical findings, therapeutic approach, and outcome of brucellar vertebral osteomyelitis. Clin Infect Dis. 2008 Feb 1;46(3):426-33. doi: 10.1086/525266. PMID: 18181740.
- Eljebbouri B, El Asri AC. Pedro Pons’ sign. Pan Afr Med J. 2014 Mar 7;17:177. doi: 10.11604/pamj.2014.17.177.4003. PMID: 25392723; PMCID: PMC4225147.
