
Diabetic foot infections are one of the most feared complications of diabetes, since it is the most tangible consequence of the disease. While peripheral vascular disease and neuropathy may take a while, having a foot infection leading to osteomyelitis and possible amputations is disfiguring, costly, and has an impact on a person’s quality of life. The combination of peripheral neuropathy leading to decreased sensation in the feet, vascular insufficiency leading to poor wound healing, and hyperglycemia causing relative immunodeficiency set up the perfect storm for the development of diabetic foot infection with particularly virulent organisms, such as staphylococcus aureus and pseudomonas (see my post on diabetic foot infection microbiology, 1). The gold-standard is bone biopsy, which I do not see often, with the next best thing being advanced imaging such as MRI and bone scans (likely a topic for a future post). A quick and dirty way to assess if someone at bedside has osteomyelitis of the foot would be through the probe-to-bone test, which relies on the idea that if you are able to probe the bone with a blunt instrument, such as a sterile metal probe, so can bacteria (2):

Seems simple. Is it reliable?
One of the first studies involved 76 patients with 77 pedal ulcers (3). In this cohort, osteomyelitis was confirmed with bone biopsy. Probe-to-bone was positive in 33 of 50 patients who had contiguous osteomyelitis, compared to only 4 in those who did not have contiguous osteomyelitis. This yielded a sensitivity and specificity of 66% and 85%, respectively.
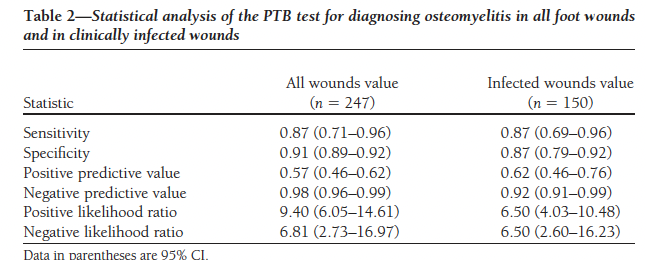
One of the criticisms of this study was the relatively high incidence of osteomyelitis may not be necessarily applicable to a more realistic population. Indeed, these were fairly selected patients. A follow up study which included 247 unselected patients with diabetic wounds found the overall sensitivity to be fairly high for all wounds evaluated for biopsy confirmed osteomyelitis (4):
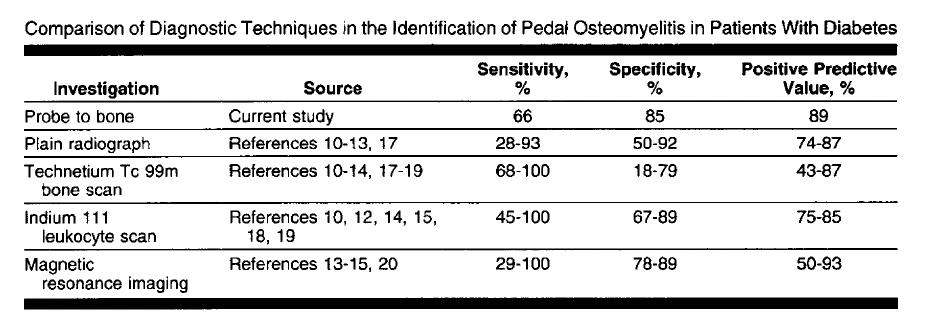
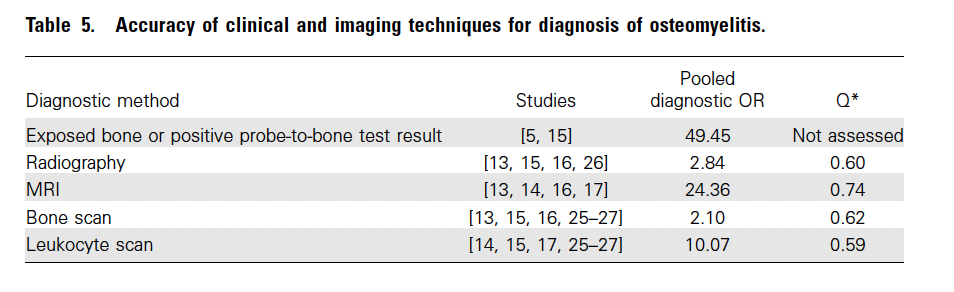
A validation, observational cohort of 132 diabetic foot ulcers in an outpatient clinic found that the PTB test had the highest sensitivity in pathologically confirmed osteomyelitis in comparison to other methods (5):

Further data comes from Mutluoglu and colleagues (6). In this cohort of 65 patients, 30 had a positive probe-to-bone test. 26 of these positive PTB tests were found to have osteomyelitis by either MRI or bone biopsy, compared to 13 with osteomyelitis with negative PTBs yielded a sensitivity of 66% but a specificity of 84%. The PPV and NPV were 87 and 62%, respectively.
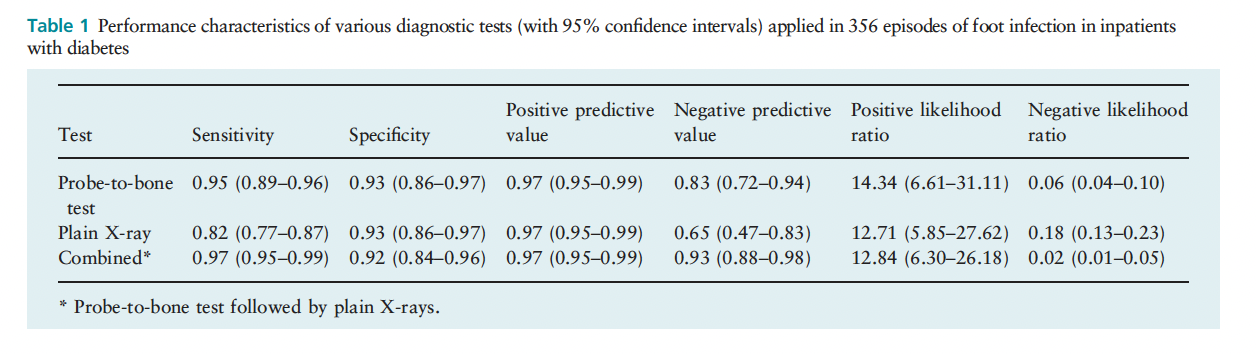
A retrospective analysis of 338 inpatients with diabetic foot infections evaluated the combination of probe-to-bone test and plain films in the diagnosis of osteomyelitis (7). 72.5% had pathologically confirmed osteomyelitis, with the sensitivity of the probe-to-bone test alone being fairly high compared to other cohorts, likely due to the fairly high prevalence of this population:
Similar findings were confirmed in a cohort study of 34 patients with bone biopsies, showing that 25 had a positive PTB test (78% sensitivity and specificity, 8).
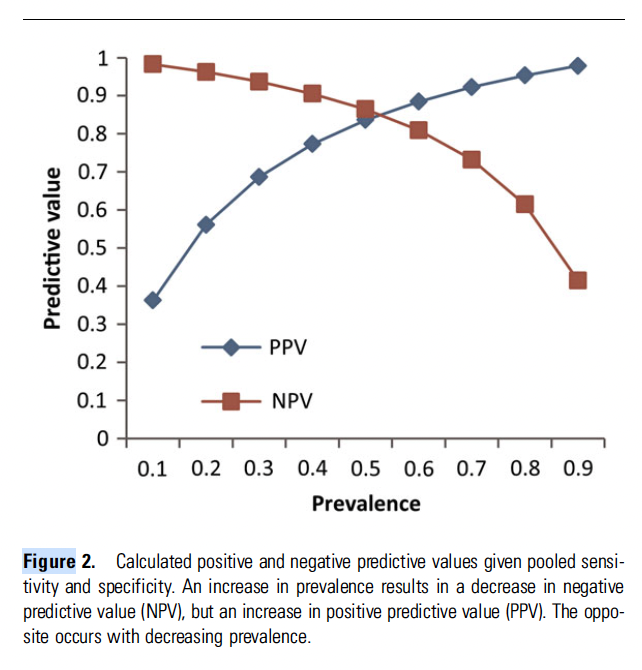
Two meta-analyses of the above studies confirmed the fairly high sensitivity. In one review of 7 studies, the pooled sensitivity/specificity for the PTB was 87% (95% CI 75-93%) and 83% (95% CI 65 to 93%), respectively (9):

Although as previously mentioned, the PPV depended largely on the prevalence of OM in the population studied:
Another meta-analysis, looking at 2 studies (Lavery 2007 and Newman 1991) found a pooled sensitivity/specificity of 60% and 91%, respectively (10):

Despite this, the pooled OR for either the physical exam OR a PTB was over 49:
It would appear that the PTB test is useful as a bedside diagnostic tool to diagnose osteomyelitis, with an incredibly high specificity with varying sensitivity. This would likely forego advanced imaging such as MRI in many instances where the diagnosis is in question, such as in the outpatient setting where it would take forever to get one and antibiotic therapy is crucial. Despite this, it appears that who does the test may matter for the purposes of diagnosis. For instance, in one cohort of 75 diabetic patients with foot ulcers and suspicion of osteomyelitis, the concordance of probe-to-bone was contingent on the experience of the person who was performing the tes (11)t. In this cohort, observer 1 was an experienced diabetic foot specialist; observer 2 was a medium-experienced professional who had anywhere of 6 to 12 months of experience with foot ulcers; and observer 3 was someone without much experience. The kappa concordance between observer 1 and 2 was 0.593, while between observer 1 and 3 it was 0.397:

References:
- [edited by] Gerald L. Mandell, John E. Bennett, Raphael Dolin. (2010). Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. Philadelphia, PA :Churchill Livingstone/Elsevier,
- Giurato L, Meloni M, Izzo V, Uccioli L. Osteomyelitis in diabetic foot: A comprehensive overview. World J Diabetes. 2017 Apr 15;8(4):135-142. doi: 10.4239/wjd.v8.i4.135. PMID: 28465790; PMCID: PMC5394733.
- Grayson ML, Gibbons GW, Balogh K, Levin E, Karchmer AW. Probing to bone in infected pedal ulcers. A clinical sign of underlying osteomyelitis in diabetic patients. JAMA. 1995 Mar 1;273(9):721-3. PMID: 7853630.
- Lavery LA, Armstrong DG, Peters EJ, Lipsky BA. Probe-to-bone test for diagnosing diabetic foot osteomyelitis: reliable or relic? Diabetes Care. 2007 Feb;30(2):270-4. doi: 10.2337/dc06-1572. PMID: 17259493.
- Morales Lozano R, González Fernández ML, Martinez Hernández D, Beneit Montesinos JV, Guisado Jiménez S, Gonzalez Jurado MA. Validating the probe-to-bone test and other tests for diagnosing chronic osteomyelitis in the diabetic foot. Diabetes Care. 2010 Oct;33(10):2140-5. doi: 10.2337/dc09-2309. Epub 2010 Jul 9. PMID: 20622159; PMCID: PMC2945149.
- Mutluoglu M, Uzun G, Sildiroglu O, Turhan V, Mutlu H, Yildiz S. Performance of the probe-to-bone test in a population suspected of having osteomyelitis of the foot in diabetes. J Am Podiatr Med Assoc. 2012 Sep-Oct;102(5):369-73. doi: 10.7547/1020369. PMID: 23001730.
- Aragón-Sánchez J, Lipsky BA, Lázaro-Martínez JL. Diagnosing diabetic foot osteomyelitis: is the combination of probe-to-bone test and plain radiography sufficient for high-risk inpatients? Diabet Med. 2011 Feb;28(2):191-4. doi: 10.1111/j.1464-5491.2010.03150.x. PMID: 21219428.
- Malone M, Bowling FL, Gannass A, Jude EB, Boulton AJ. Deep wound cultures correlate well with bone biopsy culture in diabetic foot osteomyelitis. Diabetes Metab Res Rev. 2013 Oct;29(7):546-50. doi: 10.1002/dmrr.2425. PMID: 23653368.
- Lam K, van Asten SA, Nguyen T, La Fontaine J, Lavery LA. Diagnostic Accuracy of Probe to Bone to Detect Osteomyelitis in the Diabetic Foot: A Systematic Review. Clin Infect Dis. 2016 Oct 1;63(7):944-8. doi: 10.1093/cid/ciw445. Epub 2016 Jul 1. PMID: 27369321.
- Dinh MT, Abad CL, Safdar N. Diagnostic accuracy of the physical examination and imaging tests for osteomyelitis underlying diabetic foot ulcers: meta-analysis. Clin Infect Dis. 2008 Aug 15;47(4):519-27. doi: 10.1086/590011. PMID: 18611152; PMCID: PMC7450707.
- García Morales E, Lázaro-Martínez JL, Aragón-Sánchez FJ, Cecilia-Matilla A, Beneit-Montesinos JV, González Jurado MA. Inter-observer reproducibility of probing to bone in the diagnosis of diabetic foot osteomyelitis. Diabet Med. 2011 Oct;28(10):1238-40. doi: 10.1111/j.1464-5491.2011.03283.x. PMID: 21395675.
