
In part two of “Ticks and Us” we look at two related viruses that come from ticks and lead to the same symptoms as any tick-borne illness, namely flu-like illness with thrombocytopenia and transaminitis: the Heartland and severe fever and thrombocytopenia syndrome virus!
Heartland Virus:
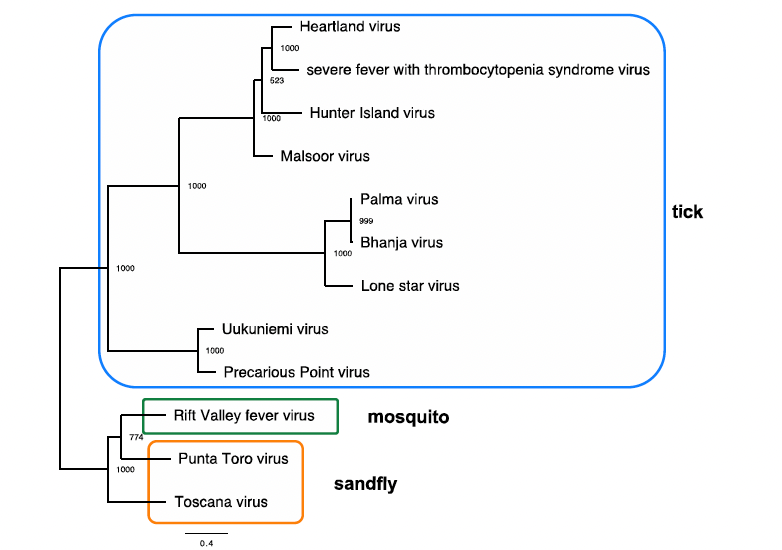
The heartland virus is part of the Phenuviridae family, genus Phlebovirus which is a single-stranded negative sense RNA virus (1). As highlighted below, the phlebovirus serocomplex is a group of serologically cross-reactive viruses that phylogenetically associate with the arthropod vector associated with their transmission. Indeed, tick-borne, mosquito-borne, and sand-fly borne phleboviruses are phylogenetically related, including the two viruses we will be talking about:
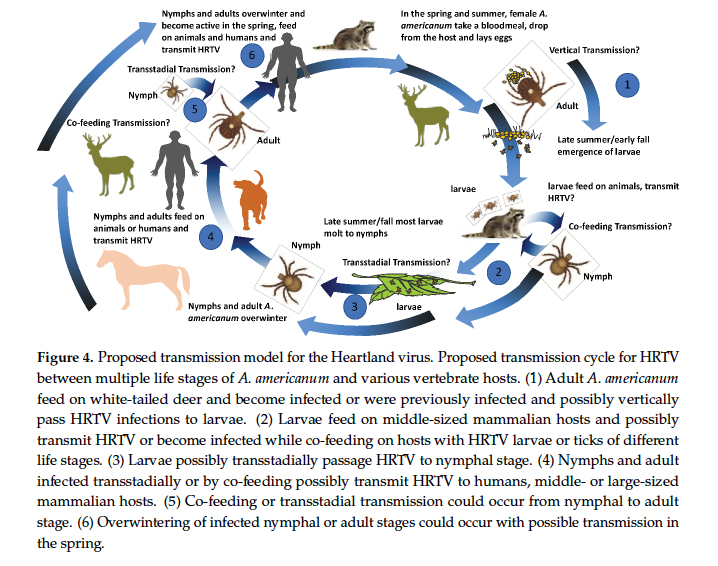
It is found in adult and nymphal A. americanum ticks, with possible transmission of Heartland virus requiring multiple life stages as well as transmission within mammals such as white-tailed deer:
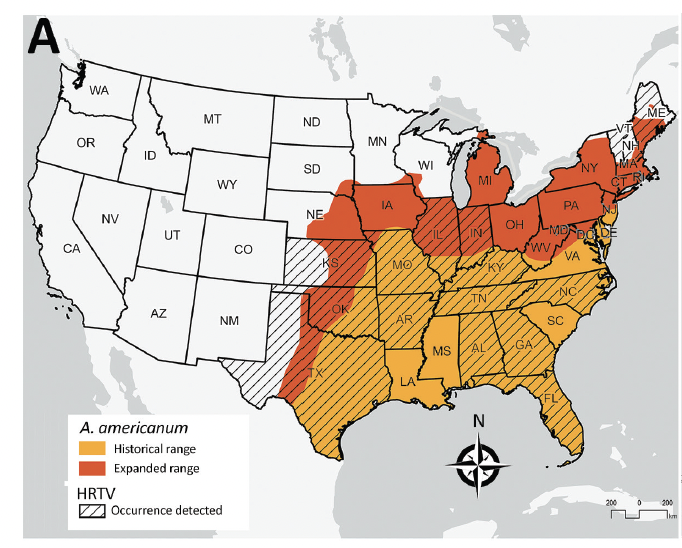
One cohort of A. americanum nymphs found the infection rate to be 0.57 per ticks screened, with the predominance being in the southeastern United States (2):
Heartland virus has been isolated from ticks in Georgia (11), Illinois (12), as well as Suffolk County, New York (13) and has been isolated from 0.9% of blood donors in a pool of 500 people from Missouri (14). Whether or not a mammalian reservoir is involved remains to be seen, however one cohort of white-tailed deer seem to show that 6.6% of those tested had neutralizing antibodies, suggesting these mammals can be infected (3). One of the first reported cases was of two patients from Missouri (4). Both had fevers, non-specific symptoms such as headache, anorexia, diarrhea with labs showing transaminitis and thrombocytopenia following a tick bite:
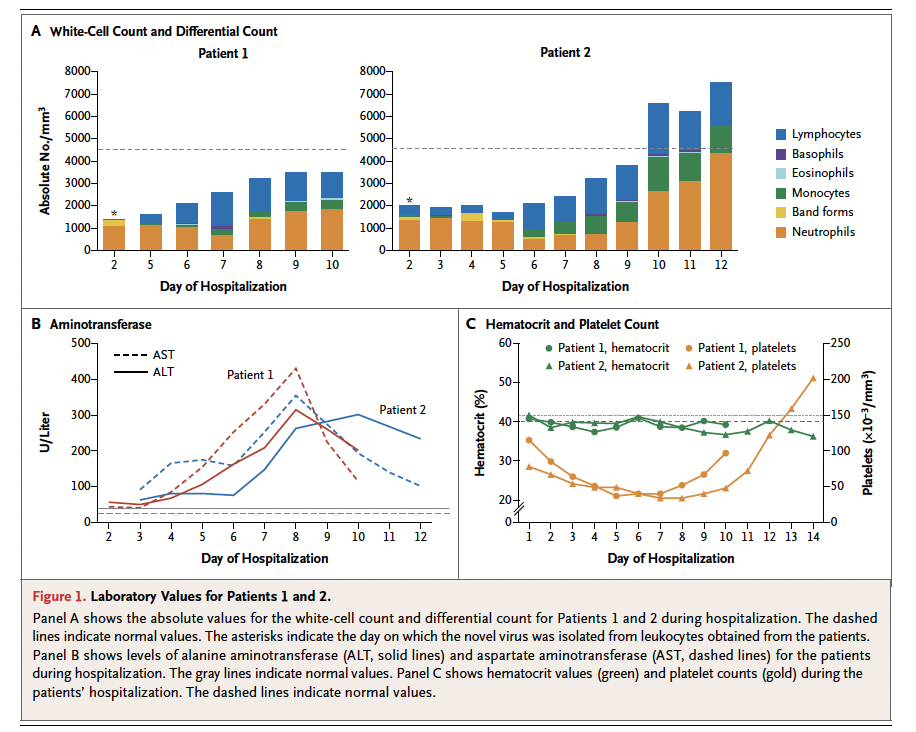
Laboratory data and electron microscopy revealed a new virus in the Bunyaviridae family, which was a single-stranded negative-sense RNA viruses:

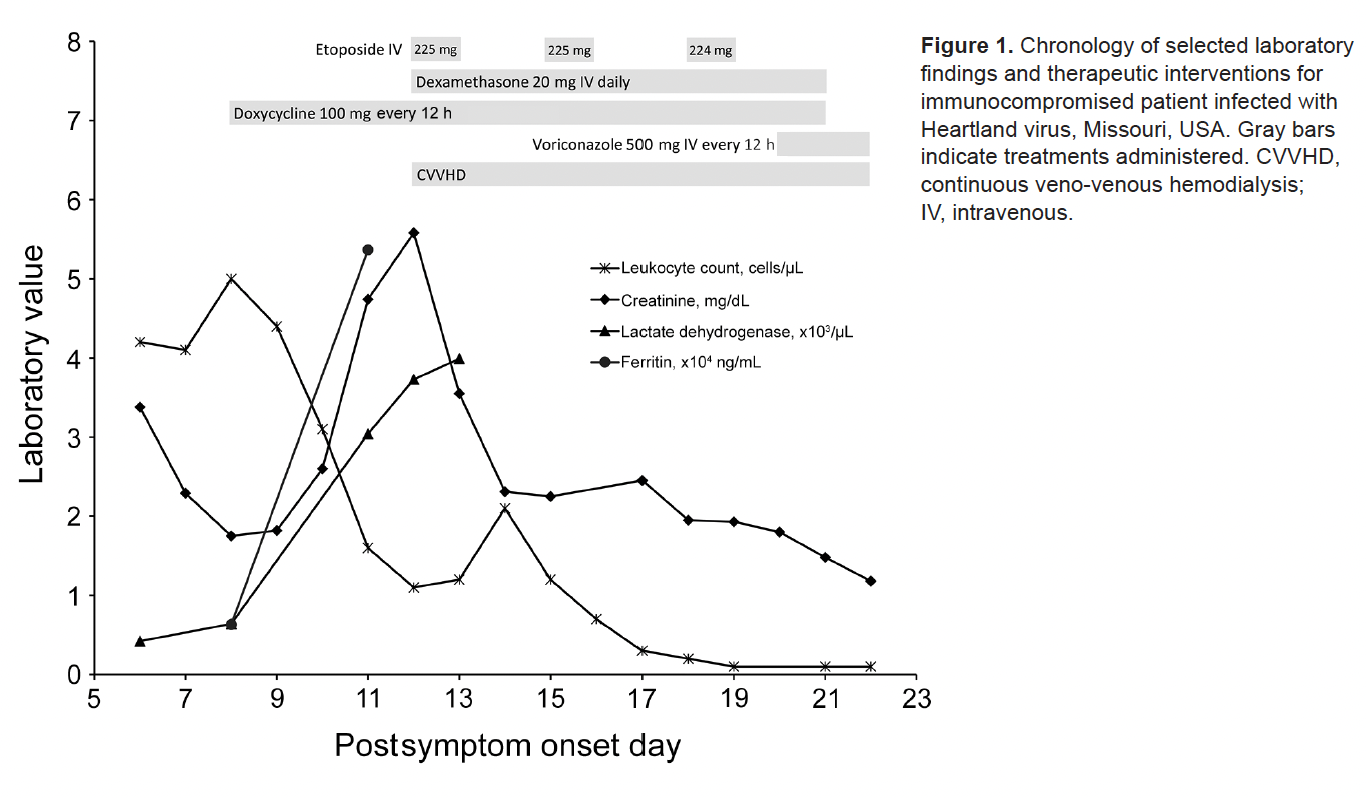
A fatal case of heartland virus was described in an 80-year old man from Tennessee (5). Similar to other tick-borne illnesses, patients tended to have thrombocytopenia and transaminitis, as seen in this graph over the course of his illness:

3 cases, two of which were suspected, also highlighted thrombocytopenia, transaminitis, and leukopenia, with one testing positive by IgM and IgG antibodies (6). Symptoms here were non-specific, however, including loss of appetite, lassitude, and generalized weakness after noticing nymphal ticks on him.
A cohort of 85 patients found that 16 had evidence of acute HRTV infection (7). All had risk-factors for tick bites, including spending at least one hour per day outside, and many having occupational risk factors. All patients had fever, leukopenia, thrombocytopenia, and many had fatigue, anorexia, nausea, headache, and confusion. 6 patients had convalescent samples submitted after 14 days and all had significant elevation in their convalescent plasma. Moreover, 13 of the 15 patients tested were positive for rRT-PCR. Risk factors for death were evaluated in a cohort of 49 hospitalized patients, and found those who died tended to have higher AST and prolonged coagulation parameters:

Moreover, viral load and inflammatory markers were significantly higher in fatal cases, which in turn was associated with worsening host biomarkers i.e higher AST and fibrinogen:

Several complications from the disease have been described. One case of HRTV complicated by multiorgan failure, mechanical ventilation, and infection with both stenotrophomonas maltophilia and A. terrus was found to have met criteria for HLH (9):
Autopsy confirmed findings of HLH, along with angioinvasive candidiasis and multiple brain infarcts. Not surprisingly, pathological reports have described liver and spleen necrosis, with immunohistochemical evidence of the virus being found in brain, liver, pancreas, heart, lung, large and small bowel, kidneys, bone marrow, lymph nodes, spleen, and muscle (10). Similar findings were obtained from a fatal case in Virginia, with congested accessory spleens with histiocytes, phagocytosing erythrocytes, and pulmonary hyperinflammation being seen (15). Moreover, immunohistochemistry testing for HRTV was positive in the heart, spleen, kidney, and liver samples. Notably, this case also triggered secondary HLH, which has been described a third time in the literature (16).
Severe Fever with Thrombocytopenia Syndrome Virus
SFTSV is a phlebovirus of the family Bunyaviridae, which includes many oddly named viruses such as the Crimean-Congo hemorrhagic fever, Rift Valley fever, and La crosse virus (17). SFTSV has been found in Henan, Hubei, Shandong, Liaoning, Anhui, and Jiangsu province as well as in Korea, Vietnam, and even Pakistan. Related to the HRTV, more is known about this virus as it has been studied for a bit longer. The virus was discovered after a 42-year-old male from Henan Province presented with a fever, fatigue, conjunctival congestion, diarrhea, abdominal pain, leukocytopenia, thrombocytopenia, and proteinuria (18). Afterwards, a cohort of 81 hospitalized patients with similar symptoms were evaluated:

186 ticks were evaluated and 10 had SFTSV RNA, suggesting this is a vector for the illness.
In general, the incubation period is usually 7-14 days (17), with the abrupt onset of fever and respiratory tract or GI symptoms followed by thrombocytopenia and leukopenia. The illness is characterized by four distinct periods: incubation, fever, multiple organ failure, and convalescence.

Multiple organ failure develops rapidly, first in the liver and heart, then in the lungs and kidneys. Average period of illness to death is 9 days. One of the earliest cohorts involved 238 patients with fever, thrombocytopenia, leukopenia syndrome (19). All had non-specific symptoms, including fever, fatigue, nausea, myalgia, and body sores:

Similarly, all patients had thrombocytopenia, proteinuria, and transaminitis:

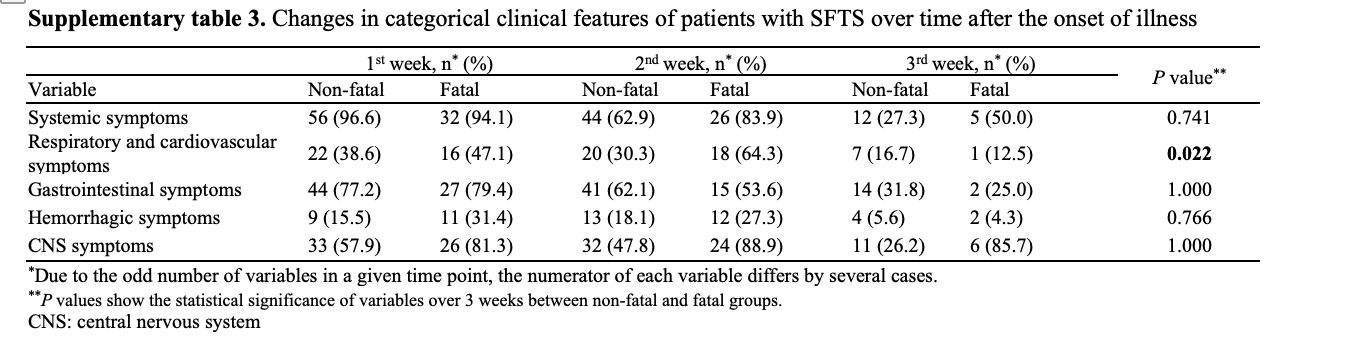
SFTS has also been found in Korea. A cohort of 170 patients evaluated the clinical manifestations of the disease (20). From 2013 to 2015, the annual incidence increased from 36 cases per year to 81 cases per year, with case fatality ratio dropping from 47.2% to 25.9%. The median time of onset of illness to hospital visit was 4 days, with main manifestations being fever (93.5%), myalgia (63.3%), diarrhea (54.3%), anorexia (53.8%), nausea (37.4%), headache (34.1%), and confusion (25.6%0. Moreover, many patients had systemic manifestations:
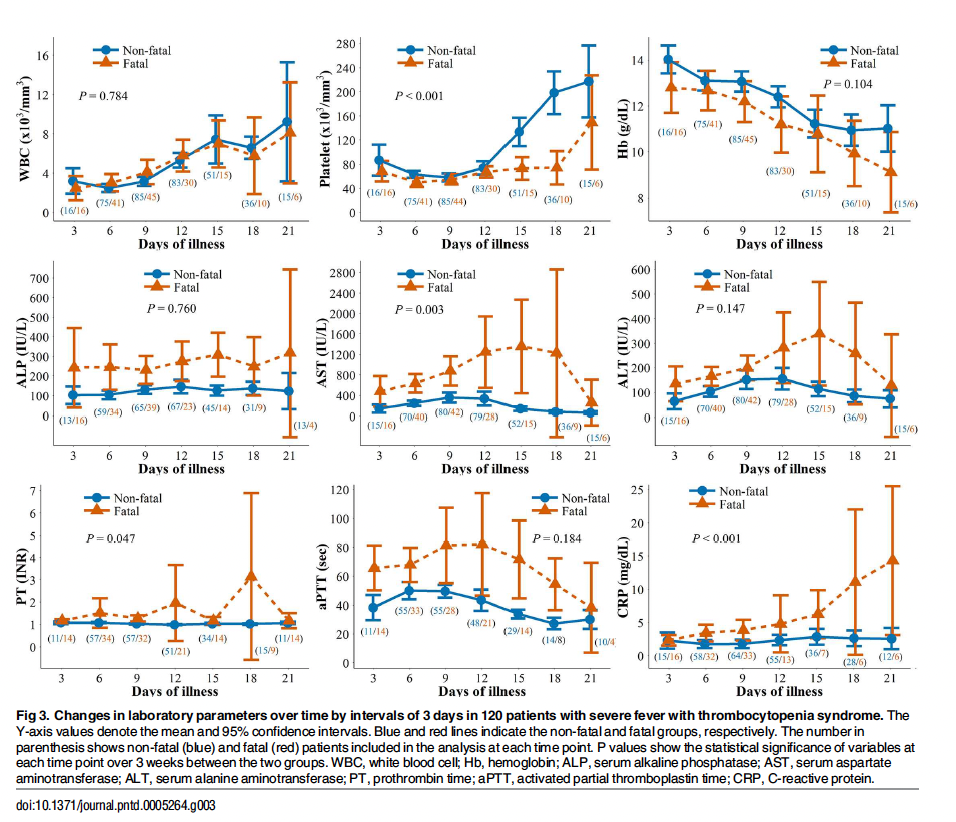
Moreover, laboratory data was trended in this cohort with lymphopenia reaching its nadir after the first week, and LFTs remaining low throughout hospitalization in those who survived:
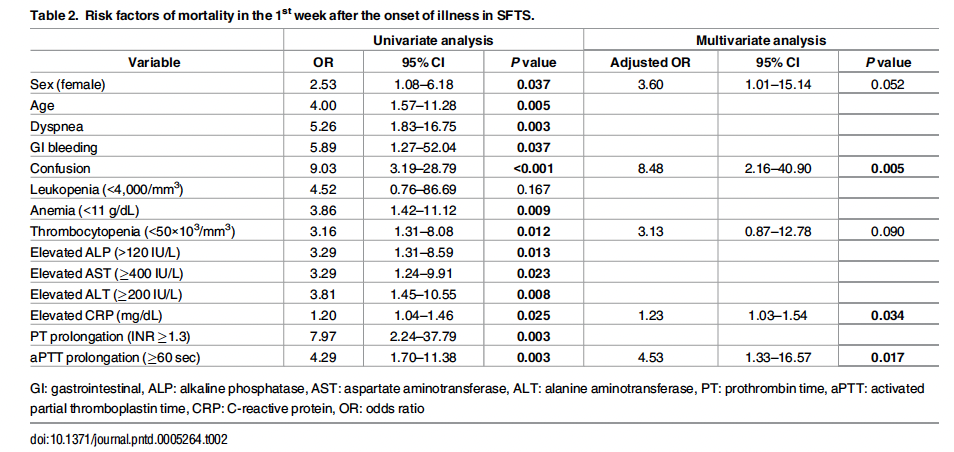
Dyspnea, GI bleed, and confusion within the first week of illness was associated with higher rates of mortality. Univariate analysis found that thrombocytopenia, anemia, high alkaline phosphatase, high CRP, and prolonged coagulation factors were associated with mortality as well:
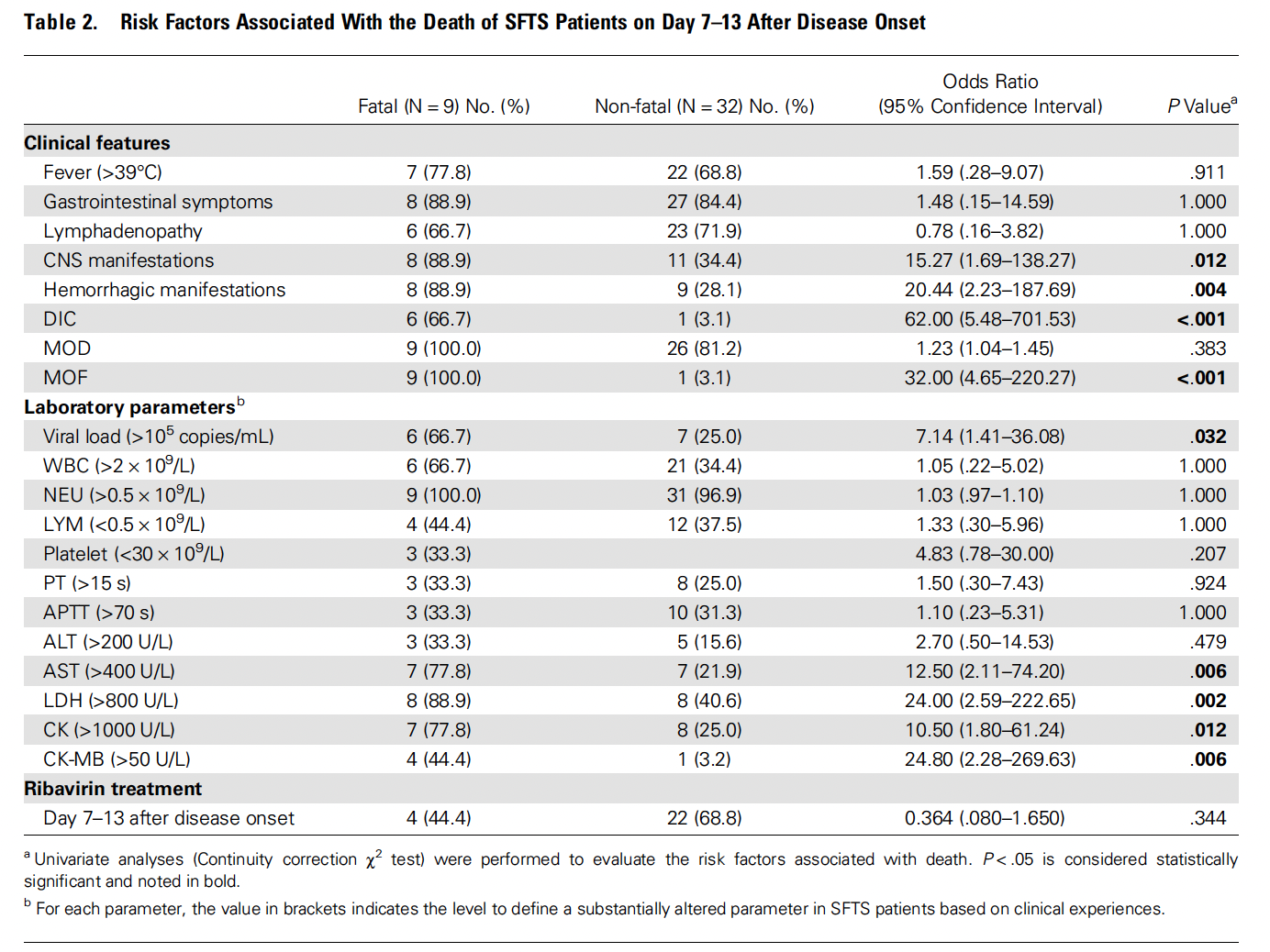
In a cohort of 59 patients, patients who died were more likely to have CNS manifestations such as apathy, lethargy, convulsions, and coma, as well as hemorrhagic manifestations (21). Moreover, viral load was compatible between those who lived and those who died during the first week of illness, however many of the associations with mortality did not occur until the second stage of illness, which was between days 7-13. Patients who died had persistently high viral loads, low platelets, and elevated liver enzymes:

Regression analysis found that viral load, level of liver enzyme elevation, and LDH/CK levels were strongly associated with mortality one week after disease onset:
Animal studies have found that inoculation of viruses into mice lead to a reduction of white blood cells as well as reduction of platelets (22). Blood viral levels peak on day one, with virus distribution being seen in the spleen, liver, kidney, lung, intestine, heart, muscle, and brain. Moreover, RNA was detected in spleen, liver, and kidney with viral RNA being significantly higher in the spleen. Pathological changes were identified in the spleen and bone marrow, with evidence of the spleen being the main target of SFTSV. SFTSV has been found to infect macrophages and platelets, and those platelets infected with SFTSV being phagocytosed by non-infected macrophages.
One last interesting bit deals with transmission. While tick-borne transmission is the rule, it appears other routes of transmission can occur. For instance, one report describes 5 cases of possible person-to-person transmission (23). Two physicians who took care of an index case had possible blood contact, an ICU nurse who drew the patient’s blood, a mortician who prepared the corpse, and family members who had contact with the patient’s blood.
References:
- Brault AC, Savage HM, Duggal NK, Eisen RJ, Staples JE. Heartland Virus Epidemiology, Vector Association, and Disease Potential. Viruses. 2018 Sep 14;10(9):498. doi: 10.3390/v10090498. PMID: 30223439; PMCID: PMC6164824.
- Newman BC, Sutton WB, Moncayo AC, Hughes HR, Taheri A, Moore TC, Schweitzer CJ, Wang Y. Heartland Virus in Lone Star Ticks, Alabama, USA. Emerg Infect Dis. 2020 Aug;26(8):1954-1956. doi: 10.3201/eid2608.200494. PMID: 32687045; PMCID: PMC7392462.
- Clarke LL, Ruder MG, Mead DG, Howerth EW. Heartland Virus Exposure in White-Tailed Deer in the Southeastern United States, 2001-2015. Am J Trop Med Hyg. 2018 Nov;99(5):1346-1349. doi: 10.4269/ajtmh.18-0555. PMID: 30255829; PMCID: PMC6221220.
- McMullan LK, Folk SM, Kelly AJ, MacNeil A, Goldsmith CS, Metcalfe MG, Batten BC, Albariño CG, Zaki SR, Rollin PE, Nicholson WL, Nichol ST. A new phlebovirus associated with severe febrile illness in Missouri. N Engl J Med. 2012 Aug 30;367(9):834-41. doi: 10.1056/NEJMoa1203378. PMID: 22931317.
- Muehlenbachs A, Fata CR, Lambert AJ, Paddock CD, Velez JO, Blau DM, Staples JE, Karlekar MB, Bhatnagar J, Nasci RS, Zaki SR. Heartland virus-associated death in tennessee. Clin Infect Dis. 2014 Sep 15;59(6):845-50. doi: 10.1093/cid/ciu434. Epub 2014 Jun 9. PMID: 24917656; PMCID: PMC4608028.
- Decker MD, Morton CT, Moncayo AC. One Confirmed and 2 Suspected Cases of Heartland Virus Disease. Clin Infect Dis. 2020 Dec 15;71(12):3237-3240. doi: 10.1093/cid/ciaa647. PMID: 32459327.
- Staples JE, Pastula DM, Panella AJ, Rabe IB, Kosoy OI, Walker WL, Velez JO, Lambert AJ, Fischer M. Investigation of Heartland Virus Disease Throughout the United States, 2013-2017. Open Forum Infect Dis. 2020 Apr 11;7(5):ofaa125. doi: 10.1093/ofid/ofaa125. PMID: 32478118; PMCID: PMC7246346.
- Zhang YZ, He YW, Dai YA, Xiong Y, Zheng H, Zhou DJ, Li J, Sun Q, Luo XL, Cheng YL, Qin XC, Tian JH, Chen XP, Yu B, Jin D, Guo WP, Li W, Wang W, Peng JS, Zhang GB, Zhang S, Chen XM, Wang Y, Li MH, Li Z, Lu S, Ye C, de Jong MD, Xu J. Hemorrhagic fever caused by a novel Bunyavirus in China: pathogenesis and correlates of fatal outcome. Clin Infect Dis. 2012 Feb 15;54(4):527-33. doi: 10.1093/cid/cir804. Epub 2011 Dec 5. PMID: 22144540.
- Carlson AL, Pastula DM, Lambert AJ, Staples JE, Muehlenbachs A, Turabelidze G, Eby CS, Keller J, Hess B, Buller RS, Storch GA, Byrnes K, Dehner L, Kirmani N, Kuhlmann FM. Heartland Virus and Hemophagocytic Lymphohistiocytosis in Immunocompromised Patient, Missouri, USA. Emerg Infect Dis. 2018 May;24(5):893-897. doi: 10.3201/eid2405.171802. PMID: 29664369; PMCID: PMC5938783.
- Fill MA, Compton ML, McDonald EC, Moncayo AC, Dunn JR, Schaffner W, Bhatnagar J, Zaki SR, Jones TF, Shieh WJ. Novel Clinical and Pathologic Findings in a Heartland Virus-Associated Death. Clin Infect Dis. 2017 Feb 15;64(4):510-512. doi: 10.1093/cid/ciw766. PMID: 27927857; PMCID: PMC5393941.
- Romer Y, Adcock K, Wei Z, Mead DG, Kirstein O, Bellman S, Piantadosi A, Kitron U, Vazquez-Prokopec GM. Isolation of Heartland Virus from Lone Star Ticks, Georgia, USA, 2019. Emerg Infect Dis. 2022 Apr;28(4):786-792. doi: 10.3201/eid2804.211540. PMID: 35318917; PMCID: PMC8962890.
- Tuten HC, Burkhalter KL, Noel KR, Hernandez EJ, Yates S, Wojnowski K, Hartleb J, Debosik S, Holmes A, Stone CM. Heartland Virus in Humans and Ticks, Illinois, USA, 2018-2019. Emerg Infect Dis. 2020 Jul;26(7):1548-1552. doi: 10.3201/eid2607.200110. PMID: 32568061; PMCID: PMC7323525.
- Dupuis AP 2nd, Prusinski MA, O’Connor C, Maffei JG, Ngo KA, Koetzner CA, Santoriello MP, Romano CL, Xu G, Ribbe F, Campbell SR, Rich SM, Backenson PB, Kramer LD, Ciota AT. Heartland Virus Transmission, Suffolk County, New York, USA. Emerg Infect Dis. 2021 Dec;27(12):3128-3132. doi: 10.3201/eid2712.211426. Epub 2021 Oct 14. PMID: 34648421; PMCID: PMC8632170.
- Lindsey NP, Menitove JE, Biggerstaff BJ, Turabelidze G, Parton P, Peck K, Basile AJ, Kosoy OI, Fischer M, Staples JE. Seroprevalence of Heartland Virus Antibodies in Blood Donors, Northwestern Missouri, USA. Emerg Infect Dis. 2019 Feb;25(2):358-360. doi: 10.3201/eid2502.181288. Epub 2019 Feb 17. PMID: 30511916; PMCID: PMC6346440.
- Liu S, Kannan S, Meeks M, Sanchez S, Girone KW, Broyhill JC, Martines RB, Bernick J, Flammia L, Murphy J, Hills SL, Burkhalter KL, Laven JJ, Gaines D, Hoffmann CJ. Fatal Case of Heartland Virus Disease Acquired in the Mid-Atlantic Region, United States. Emerg Infect Dis. 2023 Feb 23;29(5). doi: 10.3201/eid2905.221488. Epub ahead of print. PMID: 36821867.
- Ahlers CG, Matthews H, Perez R, Naggie S. Secondary hemophagocytic lymphohistiocytosis due to Heartland virus. BMJ Case Rep. 2022 Dec 8;15(12):e253082. doi: 10.1136/bcr-2022-253082. PMID: 36593621; PMCID: PMC9743278.
- Liu Q, He B, Huang SY, Wei F, Zhu XQ. Severe fever with thrombocytopenia syndrome, an emerging tick-borne zoonosis. Lancet Infect Dis. 2014 Aug;14(8):763-772. doi: 10.1016/S1473-3099(14)70718-2. Epub 2014 May 15. PMID: 24837566.
- Yu XJ, Liang MF, Zhang SY, Liu Y, Li JD, Sun YL, Zhang L, Zhang QF, Popov VL, Li C, Qu J, Li Q, Zhang YP, Hai R, Wu W, Wang Q, Zhan FX, Wang XJ, Kan B, Wang SW, Wan KL, Jing HQ, Lu JX, Yin WW, Zhou H, Guan XH, Liu JF, Bi ZQ, Liu GH, Ren J, Wang H, Zhao Z, Song JD, He JR, Wan T, Zhang JS, Fu XP, Sun LN, Dong XP, Feng ZJ, Yang WZ, Hong T, Zhang Y, Walker DH, Wang Y, Li DX. Fever with thrombocytopenia associated with a novel bunyavirus in China. N Engl J Med. 2011 Apr 21;364(16):1523-32. doi: 10.1056/NEJMoa1010095. Epub 2011 Mar 16. PMID: 21410387; PMCID: PMC3113718.
- Xu B, Liu L, Huang X, Ma H, Zhang Y, Du Y, Wang P, Tang X, Wang H, Kang K, Zhang S, Zhao G, Wu W, Yang Y, Chen H, Mu F, Chen W. Metagenomic analysis of fever, thrombocytopenia and leukopenia syndrome (FTLS) in Henan Province, China: discovery of a new bunyavirus. PLoS Pathog. 2011 Nov;7(11):e1002369. doi: 10.1371/journal.ppat.1002369. Epub 2011 Nov 17. PMID: 22114553; PMCID: PMC3219706.
- Choi SJ, Park SW, Bae IG, Kim SH, Ryu SY, Kim HA, Jang HC, Hur J, Jun JB, Jung Y, Chang HH, Kim YK, Yi J, Kim KH, Hwang JH, Kim YS, Jeong HW, Song KH, Park WB, Kim ES, Oh MD; for Korea SFTS Clinical Network. Severe Fever with Thrombocytopenia Syndrome in South Korea, 2013-2015. PLoS Negl Trop Dis. 2016 Dec 29;10(12):e0005264. doi: 10.1371/journal.pntd.0005264. PMID: 28033338; PMCID: PMC5226827.
- Gong L, Zhang L, Wu J, Lu S, Lyu Y, Zhu M, Liu B, Zhu Y, Song D, Su B, Liu Z. Clinical Progress and Risk Factors for Death from Severe Fever with Thrombocytopenia Syndrome: A Multihospital Retrospective Investigation in Anhui, China. Am J Trop Med Hyg. 2021 Feb 16;104(4):1425-1431. doi: 10.4269/ajtmh.20-0270. PMID: 33591933; PMCID: PMC8045620.
- Jin C, Liang M, Ning J, Gu W, Jiang H, Wu W, Zhang F, Li C, Zhang Q, Zhu H, Chen T, Han Y, Zhang W, Zhang S, Wang Q, Sun L, Liu Q, Li J, Wang T, Wei Q, Wang S, Deng Y, Qin C, Li D. Pathogenesis of emerging severe fever with thrombocytopenia syndrome virus in C57/BL6 mouse model. Proc Natl Acad Sci U S A. 2012 Jun 19;109(25):10053-8. doi: 10.1073/pnas.1120246109. Epub 2012 Jun 4. PMID: 22665769; PMCID: PMC3382536.
- Liu Y, Li Q, Hu W, Wu J, Wang Y, Mei L, Walker DH, Ren J, Wang Y, Yu XJ. Person-to-person transmission of severe fever with thrombocytopenia syndrome virus. Vector Borne Zoonotic Dis. 2012 Feb;12(2):156-60. doi: 10.1089/vbz.2011.0758. Epub 2011 Sep 28. PMID: 21955213.
