
Ehrlichiosis is the name of infections caused by obligate intracellular bacteria that are part of the Anaplasmatacae family (1). 3 different genera tend to cause disease: Ehrlichia chaffeensis, E. ewingii, and Anaplasma phagocytophilum. These organisms tend to be part of the Rickettsiacae family which require eukaryotic cells to grow (4). Leukocytes tend to be the target for these bacteria, with E. chaffeensis infecting monocytes and A. phagocytophilum/E.ewingii infecting granulocytes. Previously, the organism was known as the HGE agent however early studies demonstrated this organism is similar to E. equi and E. phagocytophila, however now it is now classified into a single species, A. phagocytophilum (2):

The bacteria is maintained in a transmission cycle with Ixodes persulcatus ticks, with reservoirs including the white-footed mouse and the white-tailed deer. These species of bacteria are small, intracellular bacteria with a gram negative wall but no lipopolysaccharide biosynthetic machinery. Infection by A. phagocytophilum results in disruption of normal neutrophil function, including endothelial cell wall adhesion and transmigration, motility, degranulation, respiratory burst, and phagocytosis.
One of the confusing aspects of Ehrlichia and Anaplasmosis, besides the name, is its endemicity. To make things confusing, it tends to hang around the same places where babesia and RSMF hangs out, and co-infections are common enough that you should always consider them. One review compares the three diseases in a neat table (3):
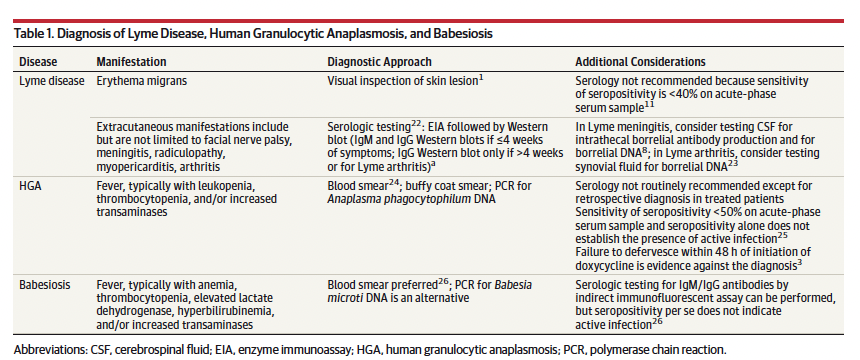
While in the United States it is found in the areas of endemicity of babesia or lyme, similar illnesses have been described throughout the world, including Europe, China, Siberian Russia, and Korea (1). For instance, a cohort of 8 patients in a Spanish clinic with similar symptoms found patients returned from southeast Asia, usually Thailand or Malaysia (9). The highlight of the disease is the morulae, little inclusions within neutrophils that represent the organism itself:

Presentation
Surveillance data from 2008 to 2012 suggest the incidence rate to be 6.3 cases per million person-years, with mortality rate being 0.3% and hospitalization rate being 31% (5). In a cohort from Wisconsin (6), seroprevalence rates increased with age (8.3% for those under 35; 17.4% for those aged 35-75, and 26% for those >75). Presentation in these patients tends to be fairly non-specific, with initial presentation being that of flu-like illnesses. An early cohort of 12 male patients with HGE provided the first description of the usual clinical course. All patients had a fever, malaise, shaking chills, headaches, and myalgias. All engaged in frequent outdoor activities, with an incubation period from known tick-bite to illness was a median 10.5 days.


All patients had morulae on their peripheral smear, with an inverse relationship between WBC count and the number of infected neutrophils being found (r -0.82):

One of the earliest reports from 228 patients with HGE demonstrated a lot of the important characteristics of the disease (7). Of these, 41 had confirmed or probable HGE, with 25 admitting to regular animal contact (20 with dogs), and 37 patients reported frequent tick exposure prior to illness. The incubation period from bite to illness ranged from one day to 60 days, with a median of 8 days. Of these, most had non-specific symptoms of fevers, malaise, and headaches:
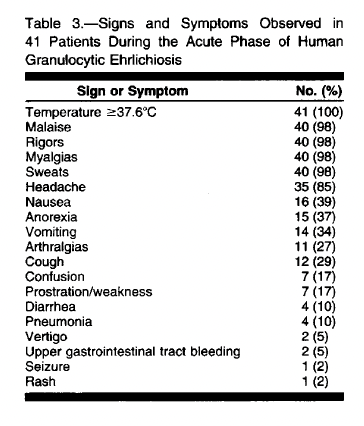
Labs were notable for transaminitis and thrombocytopenia, with the average percentage of infected neutrophils ranging from 1% to 42%.

A prospective study of 30 patients found the most common symptoms of HGE included fever, chills, headache, nausea, and myalgias (8):

Obviously, not super specific. Labs were notable for lymphopenia, thrombocytopenia, and transaminitis:

Another pair of reviews (1, 2) highlights the typical disease pattern of Anaplasmosis:


While not typically fatal, a case report has described a fatal case of HGE in a patient who failed to respond to doxycycline, whose course was complicated by congestive heart failure and subendocardial infarct (10). Interestingly, autopsy revealed invasive pulmonary aspergillosis suggesting maybe the relative immunosuppression from HGE lead to the development of this opportunistic infection. While CNS involvement is not typical, a cohort of 15 patients with CNS symptoms prompted lumbar puncture investigations (11). Manifestations included confusion, severe headache, lethargy, hyperreflexia, clonus, photophobia, and cranial nerve palsy. Of these, 8 had abnormal CNS with an additional 13 patients being evaluated after review of the literature. CSF WBC ranged from 0 to 1400 x 106/L, with protein ranging from 0.39 to 2.06 (g/L), and glucose ranged from 2.0-6 (mmol/L). 79% had lymphocytosis, and morulae was only observed in one patient’s CSF.

Four of these had positive PCR results. Pericarditis with pathological evidence of HGE has also been described in the literature (12). This is to say there may be more atypical presentations of HGE that we are not aware of, though how clinically relevant it becomes to management remains to be seen.
Diagnosis and Antibody Response
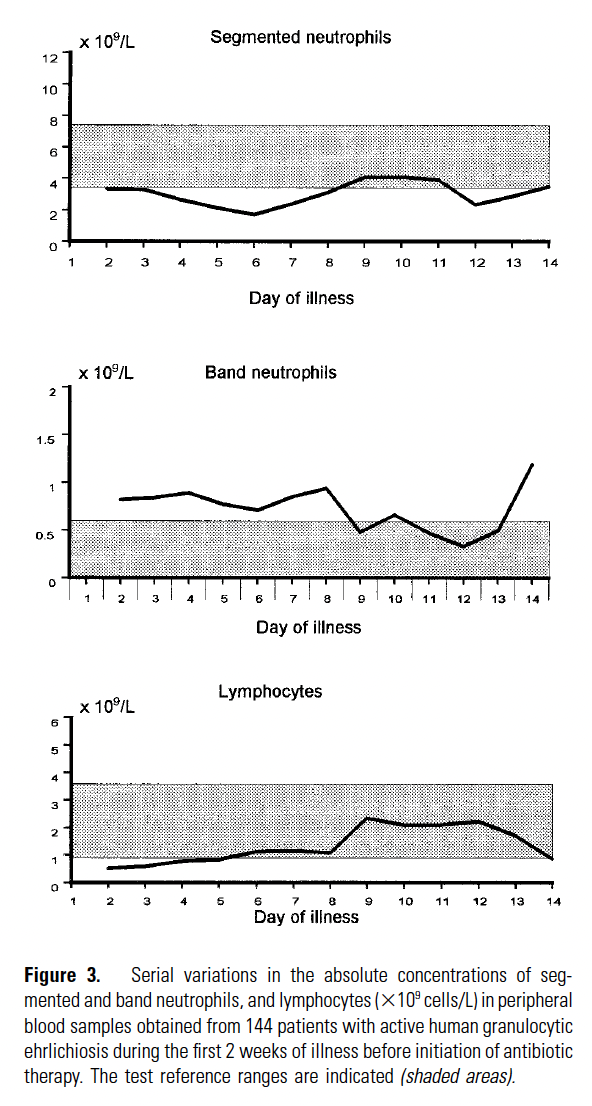
HGE and Anaplasmosis is one of those diseases that we look for LFTs and CBC to look at a trend. Specifically, we are looking at transaminitis and thrombocytopenia. Indeed, a cohort of 144 patients evaluated the trend in their CBC during their first 14 days of illness (13). Only 18% of patients had normal WBC and platelet numbers. The nadir of WBC tended to be around day 5, while for platelets was on day 6:

Moreover, while most patients had relative neutrophilia, many had absolute lymphopenia throughout the duration of illness:
When comparing patients with HGE with control patients, patients were more likely to have leukopenia, absolute lymphopenia, and thrombocytopenia:

Further, the absolute risk of HGE was significantly higher when platelets were <100, suggesting this is a more powerful predictor in comparison to WBC:

While complete metabolic profile and complete blood counts could suggest a diagnosis, smear and serologies are the way to make a definitive diagnosis. Detection of morulae is fairly specific, with evaluation of 200 granulocytes on smear being able to detect all patients in one retrospective cohort (14). Development of antibodies against HGE is fairly quick, with one cohort with known timeframe of illness becoming seropositive within a week of illness (15):

Titers rose within the next few weeks and remained fairly high even after 3 months of illness. Notably, however, 74 out of 142 patients infected with HGE had significant cross-reactivity with other ehrlichia and rickettsial antigens:

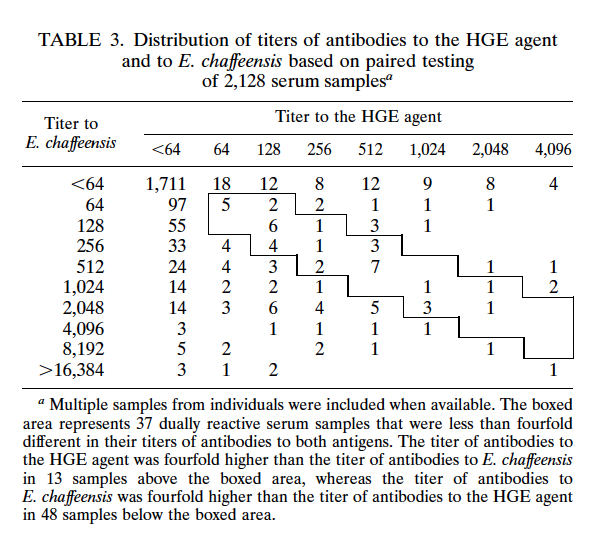
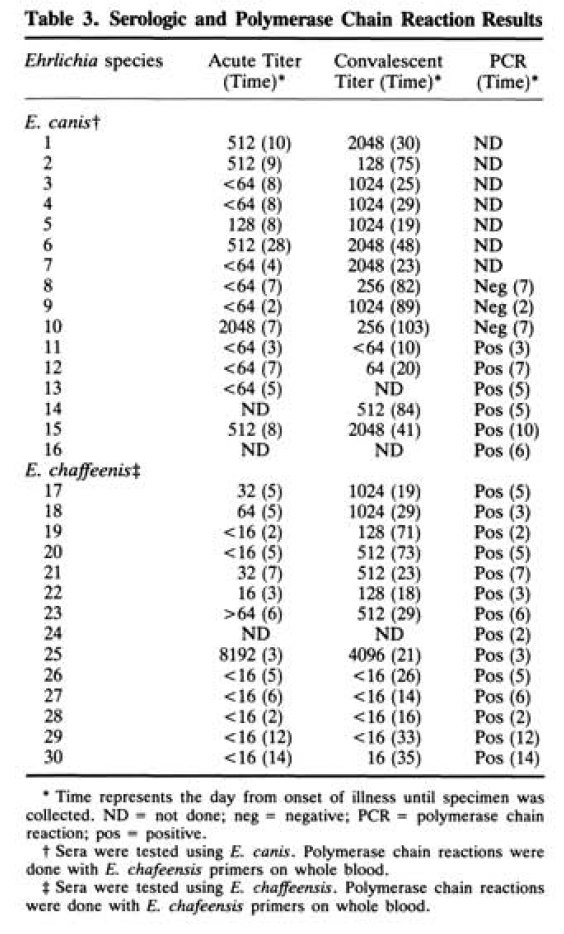
34 patients with human monocytic ehrlichiosis due to E. chaffeensis also had antibodies to HGE, suggesting the use of the two antibodies may be required for diagnosis. Moreover, it appears there is cross-reactivity with other antibodies, including to those of E.canis. In this cohort, acute and convalescent serologies to E. canis were used for diagnosis prior to those of E. chaffeenis becoming available:
The titers may be influenced by doxycycline therapy, with antibody response being evaluated in a cohort of 152 patients over a 42 month period (17). Patients in the “early group” had therapy with doxycycline within 7 days, while those in the “late group” had therapy started after 7 days of illness. In both early and late groups, the rates of positivity for the peripheral blood smear, PCR, and culture were the same. The IFA was positive only in 24% of those in the early group, with all having a four-fold rise in their IFA titers in convalescent samples:

When looking at the GMT, those in the early group had lower GMT than in the late group:
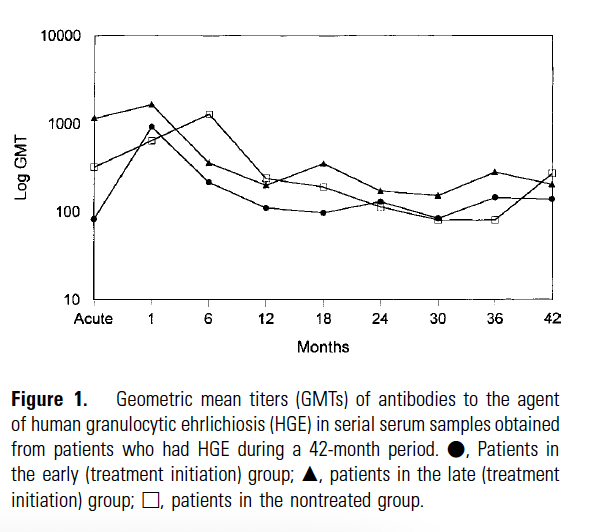
At 42 months, only 7.2% of patients remained seropositive with a steep drop off at one year:

Utility of PCR:
This is probably the one test that we have that is the most sensitive and specific in the initial stages of the illness, with serologies being useful when paired with convalescent serologies. One aforementioned review (1) compares the sensitivity and specificity of blood smear, PCR, and serologies and found that PCR tended to be the most useful in the first week:
Serology tends to suffer from being unable to tell chronic from acute infection and its lower utility in areas of high seroprevalence. In acute illness PCR is quite sensitive, with one review noting that it was able to pick up less than 2.5 infected cells (18). Multiplex PCR assays have also been used, which detect A. phagocytophilum, E. chaffeensis, E. ewingii, E. muris eauclarensis, Borrelia miyamotoi, Babesia, Rickettsia spp, amongst other Borrelia spp (19). A review of 371 samples found that tick-borne pathogen panel call rate was 99.7%, and it was found to have high agreement when compared to individual PCR complexes:


Similarly, another multiplex PCR found that for A. phagocytophilum, the sensitivity and specificity was 100% for both. For E. chaffeensis, the sensitivity was 95% and specificity was 99% (20).
TL;DR
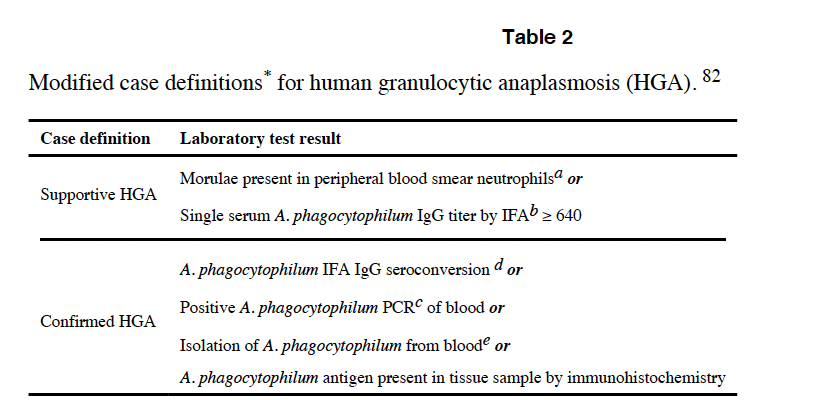
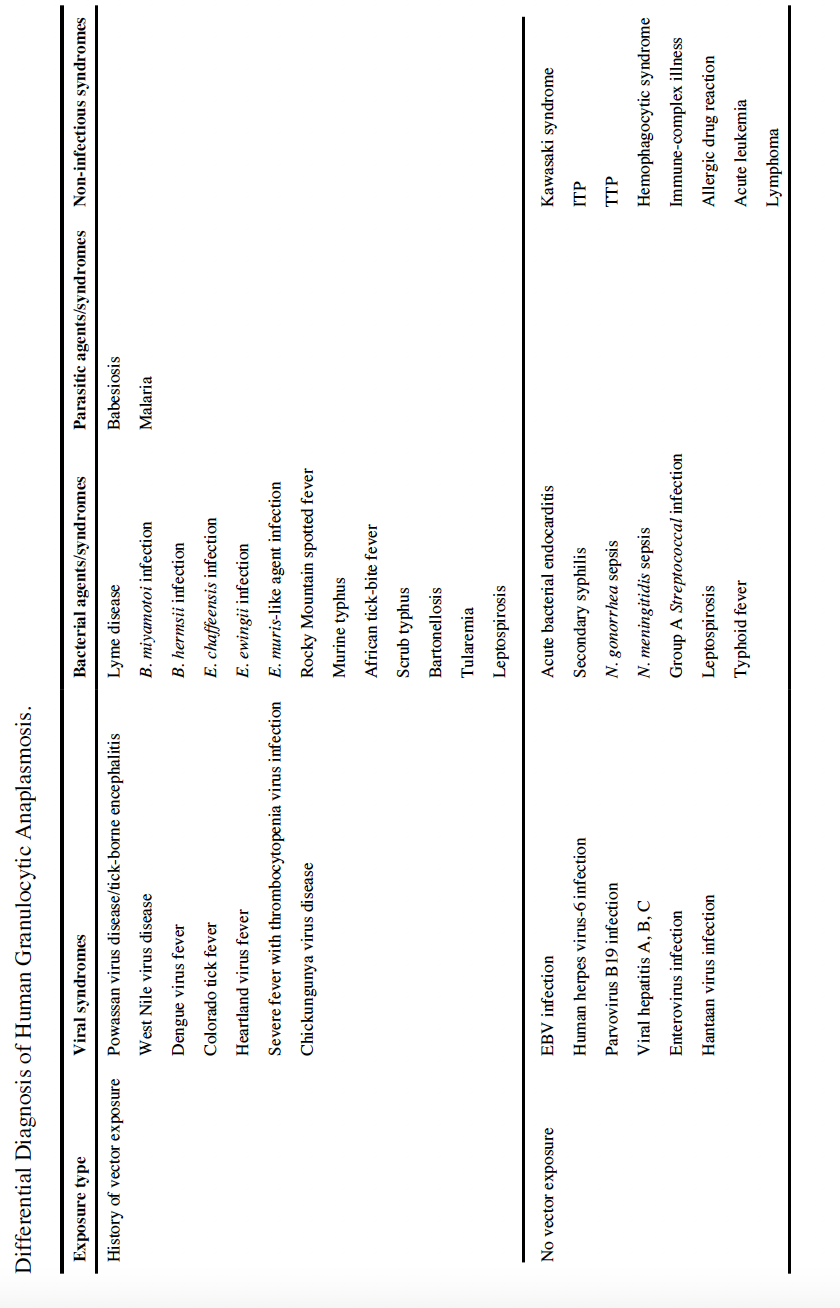
- A review (2) highlights case definitions and differential diagnosis for HGE
- Usually CBC with microscopy to look at morulae (at least look at 200 cells), paired serologies, or multiplex PCR is helpful
- No surprise, treatment here is doxycycline for 10-14 days
References:
- Dumler JS, Madigan JE, Pusterla N, Bakken JS. Ehrlichioses in humans: epidemiology, clinical presentation, diagnosis, and treatment. Clin Infect Dis. 2007 Jul 15;45 Suppl 1:S45-51. doi: 10.1086/518146. PMID: 17582569.
- Dumler JS, Choi KS, Garcia-Garcia JC, Barat NS, Scorpio DG, Garyu JW, Grab DJ, Bakken JS. Human granulocytic anaplasmosis and Anaplasma phagocytophilum. Emerg Infect Dis. 2005 Dec;11(12):1828-34. doi: 10.3201/eid1112.050898. PMID: 16485466; PMCID: PMC3367650.
- Sanchez E, Vannier E, Wormser GP, Hu LT. Diagnosis, Treatment, and Prevention of Lyme Disease, Human Granulocytic Anaplasmosis, and Babesiosis: A Review. JAMA. 2016 Apr 26;315(16):1767-77. doi: 10.1001/jama.2016.2884. PMID: 27115378; PMCID: PMC7758915.
- [edited by] John E. Bennett, Raphael Dolin, Martin J. Blaser. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Philadelphia, PA :Elsevier/Saunders, 2015.
- Dahlgren FS, Heitman KN, Drexler NA, Massung RF, Behravesh CB. Human granulocytic anaplasmosis in the United States from 2008 to 2012: a summary of national surveillance data. Am J Trop Med Hyg. 2015 Jul;93(1):66-72. doi: 10.4269/ajtmh.15-0122. Epub 2015 Apr 13. PMID: 25870428; PMCID: PMC4497906.
- Bakken JS, Goellner P, Van Etten M, Boyle DZ, Swonger OL, Mattson S, Krueth J, Tilden RL, Asanovich K, Walls J, Dumler JS. Seroprevalence of human granulocytic ehrlichiosis among permanent residents of northwestern Wisconsin. Clin Infect Dis. 1998 Dec;27(6):1491-6. doi: 10.1086/515048. PMID: 9868666.
- Bakken JS, Dumler JS, Chen SM, Eckman MR, Van Etta LL, Walker DH. Human granulocytic ehrlichiosis in the upper Midwest United States. A new species emerging? JAMA. 1994 Jul 20;272(3):212-8. PMID: 8022040.
- Bakken JS, Krueth J, Wilson-Nordskog C, Tilden RL, Asanovich K, Dumler JS. Clinical and laboratory characteristics of human granulocytic ehrlichiosis. JAMA. 1996 Jan 17;275(3):199-205. PMID: 8604172.
- Camprubí-Ferrer D, Portillo A, Santibáñez S, Almuedo-Riera A, Rodriguez-Valero N, Subirà C, Martinez MJ, Navero-Castillejos J, Fernandez-Pardos M, Genton B, Cobuccio L, Van Den Broucke S, Bottieau E, Muñoz J, Oteo JA. Incidence of human granulocytic anaplasmosis in returning travellers with fever. J Travel Med. 2021 Jun 1;28(4):taab056. doi: 10.1093/jtm/taab056. PMID: 33839778.
- Hardalo CJ, Quagliarello V, Dumler JS. Human granulocytic ehrlichiosis in Connecticut: report of a fatal case. Clin Infect Dis. 1995 Oct;21(4):910-4. doi: 10.1093/clinids/21.4.910. PMID: 8645839.
- Ratnasamy N, Everett ED, Roland WE, McDonald G, Caldwell CW. Central nervous system manifestations of human ehrlichiosis. Clin Infect Dis. 1996 Aug;23(2):314-9. doi: 10.1093/clinids/23.2.314. PMID: 8842270.
- Jahangir A, Kolbert C, Edwards W, Mitchell P, Dumler JS, Persing DH. Fatal pancarditis associated with human granulocytic Ehrlichiosis in a 44-year-old man. Clin Infect Dis. 1998 Dec;27(6):1424-7. doi: 10.1086/515014. PMID: 9868655.
- Bakken JS, Aguero-Rosenfeld ME, Tilden RL, Wormser GP, Horowitz HW, Raffalli JT, Baluch M, Riddell D, Walls JJ, Dumler JS. Serial measurements of hematologic counts during the active phase of human granulocytic ehrlichiosis. Clin Infect Dis. 2001 Mar 15;32(6):862-70. doi: 10.1086/319350. Epub 2001 Mar 7. PMID: 11247709.
- Rand JV, Tarasen AJ, Kumar J, Homan SM, Tobin E. Intracytoplasmic granulocytic morulae counts on confirmed cases of ehrlichiosis/anaplasmosis in the Northeast. Am J Clin Pathol. 2014 May;141(5):683-6. doi: 10.1309/AJCP6Q2BOKYALDYZ. PMID: 24713739.
- Comer JA, Nicholson WL, Olson JG, Childs JE. Serologic testing for human granulocytic ehrlichiosis at a national referral center. J Clin Microbiol. 1999 Mar;37(3):558-64. doi: 10.1128/JCM.37.3.558-564.1999. PMID: 9986812; PMCID: PMC84468.
- Everett ED, Evans KA, Henry RB, McDonald G. Human ehrlichiosis in adults after tick exposure. Diagnosis using polymerase chain reaction. Ann Intern Med. 1994 May 1;120(9):730-5. doi: 10.7326/0003-4819-120-9-199405010-00002. PMID: 8147545.
- Bakken JS, Haller I, Riddell D, Walls JJ, Dumler JS. The serological response of patients infected with the agent of human granulocytic ehrlichiosis. Clin Infect Dis. 2002 Jan 1;34(1):22-7. doi: 10.1086/323811. Epub 2001 Nov 21. PMID: 11731941.
- Massung RF, Slater KG. Comparison of PCR assays for detection of the agent of human granulocytic ehrlichiosis, Anaplasma phagocytophilum. J Clin Microbiol. 2003 Feb;41(2):717-22. doi: 10.1128/JCM.41.2.717-722.2003. PMID: 12574272; PMCID: PMC149680.
- Shakir SM, Mansfield CR, Hays ED, Couturier MR, Hillyard DR. Evaluation of a Novel High-Definition PCR Multiplex Assay for Simultaneous Detection of Tick-Borne Pathogens in Human Clinical Specimens. J Clin Microbiol. 2020 Feb 24;58(3):e01655-19. doi: 10.1128/JCM.01655-19. PMID: 31852765; PMCID: PMC7041590.
- Reller ME, Dumler JS. Development and Clinical Validation of a Multiplex Real-Time Quantitative PCR Assay for Human Infection by Anaplasma phagocytophilum and Ehrlichia chaffeensis. Trop Med Infect Dis. 2018 Jan 29;3(1):14. doi: 10.3390/tropicalmed3010014. PMID: 30274412; PMCID: PMC6136628.]
