
Unfortunately, i have not being able to figure out how to rotate some of the images on WordPress, despite my google docs being in the correct configuration. Hence, some tables are rotated the wrong way. Do know I tried to fix it.
I have been putting off writing about this since the immunology behind this topic is actually quite complicated. If you look up any infectious disease textbook, tuberculosis is the prototypical disease to understand adaptive immunity. Moreover, the diagnosis of latent tuberculosis, which for the most part was diagnosed with a tuberculin skin test (TST) has no gold standard. In the last few decades, we have dealt away with the TST and brought forth a new generation of tests: the interferon-gamma release assays (IGRAs).
Immunology:
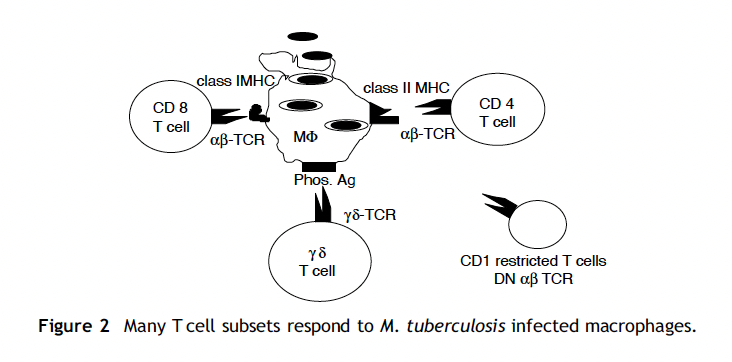
So what is TB? Or how does it happen? Bacilli are inhaled and go to the alveoli where they are eaten up by macrophages, epithelial cells, dendritic cells, and neutrophils aka the innate immune system (1). Some of these cells (macrophages and DCs) drain to the lymph nodes, where the adaptive immune system is turned out. From here, localized alveolitis with activated T-cells, lymphocytes, and macrophages occurs with large amounts of locally secreted IFN-gamma being released, leading to more alveolar neutrophil recruitment as well as activation of macrophages to promote bacterial killing. While this image is super busy, realize the interplay between CD4 and CD8 T-cells, with CD8 T-cells being cytolytic to TB cells:

The implication of the above is actually interesting. The same review highlights that up to 50% of close contacts of microbiologically confirmed tuberculosis cases had no evidence of latent tuberculosis, suggesting that an individual’s innate immunity may prevent the induction of adaptive immune response and explain the persistently negative post-exposure TST results.

Given the difficulty in diagnosing latent tuberculosis, many disease phenotypes that take into account radiographic, clinical, and microbiological correlates have been proposed:

Again, recall we have to use surrogates for the diagnosis of tuberculosis, given how difficult it is to culture it in the first place. In all instances, TST and IGRAs are surrogates of the immune response to tuberculosis, and does not necessarily mean you have bacilli in you; however given the implications of pulmonary tuberculosis, those who have evidence of ever “seen” the bacilli are treated.
It helps to think of tuberculosis, at least pulmonary tuberculosis, as a spectrum of disease rather than one entity (2). The disease exists as a spectrum from infection by inhalation of bacilli, to the control of said bacilli by the innate immune system with elimination of infection and acquisition of memory T-cells leading to protection to subsequent infection. Of course a certain fraction of these folks will not control it and thus, be labeled as latent tuberculosis:

Why is this important? Those who have latent tuberculosis will have viable bacilli within them, with some studies suggesting that 5 to 15% of folks infected with progress to active tuberculosis.
How does tuberculosis progress to latent TB? This is likely a result of the failure of innate immunity (namely, macrophages) to control the slowly replicating bacilli (3). Due to this, the adaptive immunity kicks in in the form of T-cells, which controls, but does not eradicate, the infection:

As highlighted above, after the initial innate phase, adaptive immunity develops to control the rapidly dividing bacilli, followed by chronic memory immune phase to control persistent bacilli. If the adaptive immune system fails, then these folks will progress to pulmonary tuberculosis. Central to this is the CD4-T cell, which secretes interferon-gamma and TNF-alpha/Beta, which are cytotoxic to macrophages infected with tuberculosis. While IFN-gamma in and of itself doesn’t kill macrophages infected with TB, it enhances antigen-presenting cell function amongst other roles. Activation of CD8- T cells leads to also secretion of IFN-gamma, although less than that of CD4, but more importantly have other tools such as granulysin and perforin, which allow it to lyse infected macrophages.
Despite this, MTB has two mechanisms to interfere with innate immunity; namely, inducing cytokines to inhibit T cell function, as well as apoptosis of mycobacterial antigen-specific T-cells. There is some animal data to suggest that antigen processing is also affected by MTB infection.
Rationale behind IGRAs:
Before moving into IGRAs, it is helpful to look at the test that started it all: the tuberculin skin test (TST). This test is based on the delayed-type hypersensitivity reaction that occurs when patients that are infected with MTB are exposed to “TB antigens” in extracts of culture filtrates, aka the tuberculins (4). This is a crude mixture of antigens that are shared amongst several types of mycobacteria, including M. bovis, MTB, NTMs, and BCG (7):
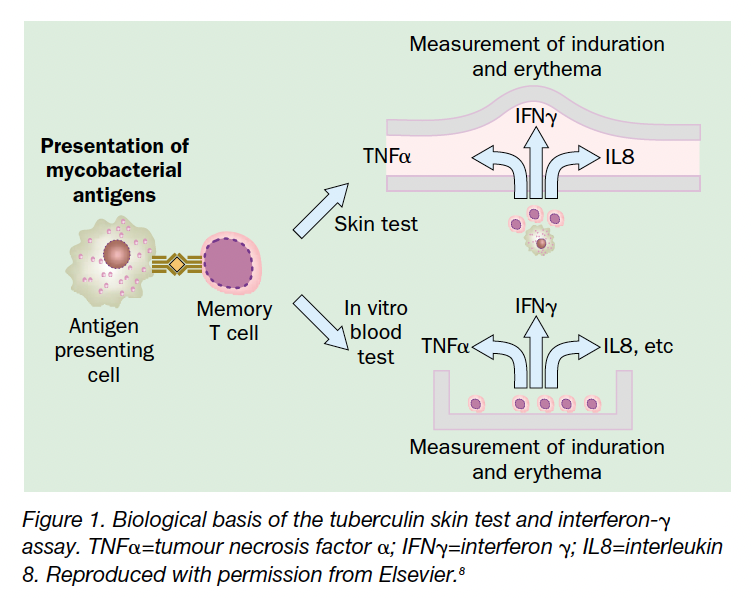
T-cells that have been exposed to the main organism are primed to respond to these antigens, and upon injection of tuberculins into the skin, these T-cells are recruited to the site, leading to secretion of interferon gamma, and an induration at the site of injection. Depending on the cut-off, the response can be quantified as positive or negative.
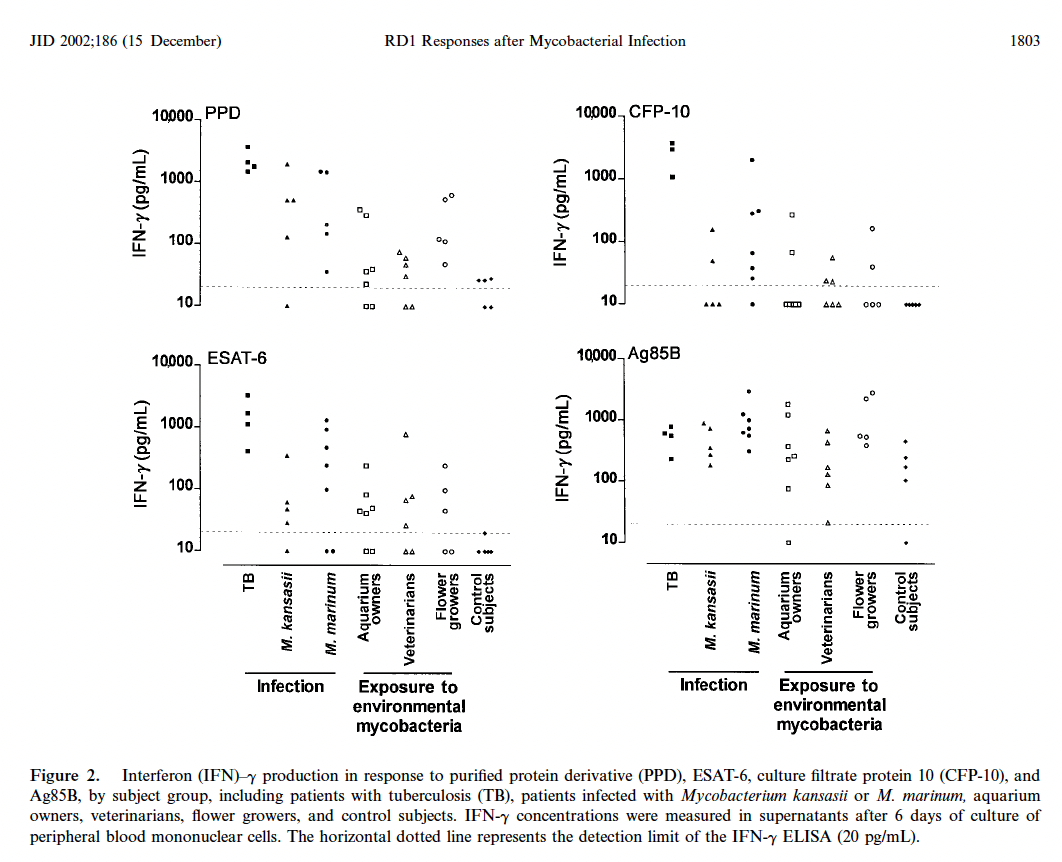
Yet, there are a lot of disadvantages. First, it requires 2 healthcare visits. Second, the purified protein derivative seems to be shared by MTB and BCG, leading to false positive results in those who have received the vaccine. Using comparative genomic methods, the region of difference, RD1, was discovered and found to be present in both MTB and M. bovis but not BCG (5). As a result, M. tuberculosis and M.bovis have 2 different proteins that are encoded by RD1, the early secretory antigenic target 6 (ESAT-6) and culture filtrate protein 10 (CFP-10). Despite this, these agents have been found in other strains of Mycobacteria such as M. marinum or M. kansasii. A cohort of 42 patients who had been exposed to M. marinum, M. kansassi infected with NTM, pulmonary tuberculosis, or non-infected found that IFN-gamma can be stimulated by ESAT-6 and CFP-10 M. kansasii or M. marinum, however responses were not as vigorous as that for MTB:
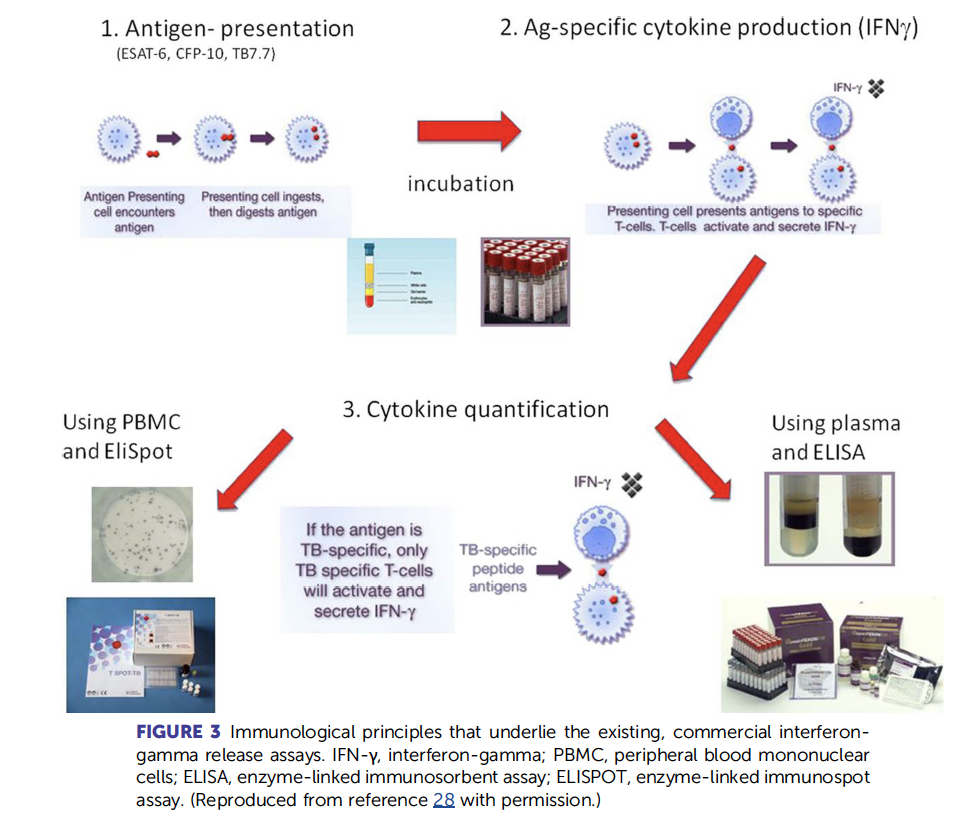
What if, let’s say, we use a test that targets these 2 antigens. And what if, lets say, this can be done in vitro aka within a test-tube. This is the rationale behind IGRAs. These are blood tests that measure T-cell immune response to a TB antigen by quantifying the amount of interferon-gamma released (2). The higher the response, the more likely someone has been exposed to tuberculosis. he two known tests are the T-spot and the Quantiferon, the latter of which has had several iterations, the latest one which is called the Quantiferon-TB Gold plus:
The original quantiferon used the original PPD antigens, so it was not the best. Since then, we’ve had at least 4 generations of Quantiferon, with the latest one being the Quantiferon GOLD – Plus:

Of course, the test itself is not perfect, with other strains of mycobacteria also having ESAT-6 and CFP-10, which include M. kansasii, M. szulgai, and M. marinum (6). I’ll go over the idea of the fourth generation in a bit, since its where a lot of the confusion tends to be in. This test actually has 4 tubes in it:
- The Nil – put blood in there to measure baseline IFN-gamma. Essentially, the idea is you should have little to no IFN-gamma here since there is no stimulus
- TB1 – antigens to stimulate CD4, typically made up of long peptides
- TB2 – antigens to stimulate CD8, made up of short and long peptides
- Mitogen – stimulates your cells to release IFN-gamma. Essentially, this is the IFN-gamma positive control
To get a positive test, you subtract the amount of interferon from either tube (only one has to be positive) by the background IFN-gamma (aka the nil). This gives you the IFN-gamma released by the TB antigens:
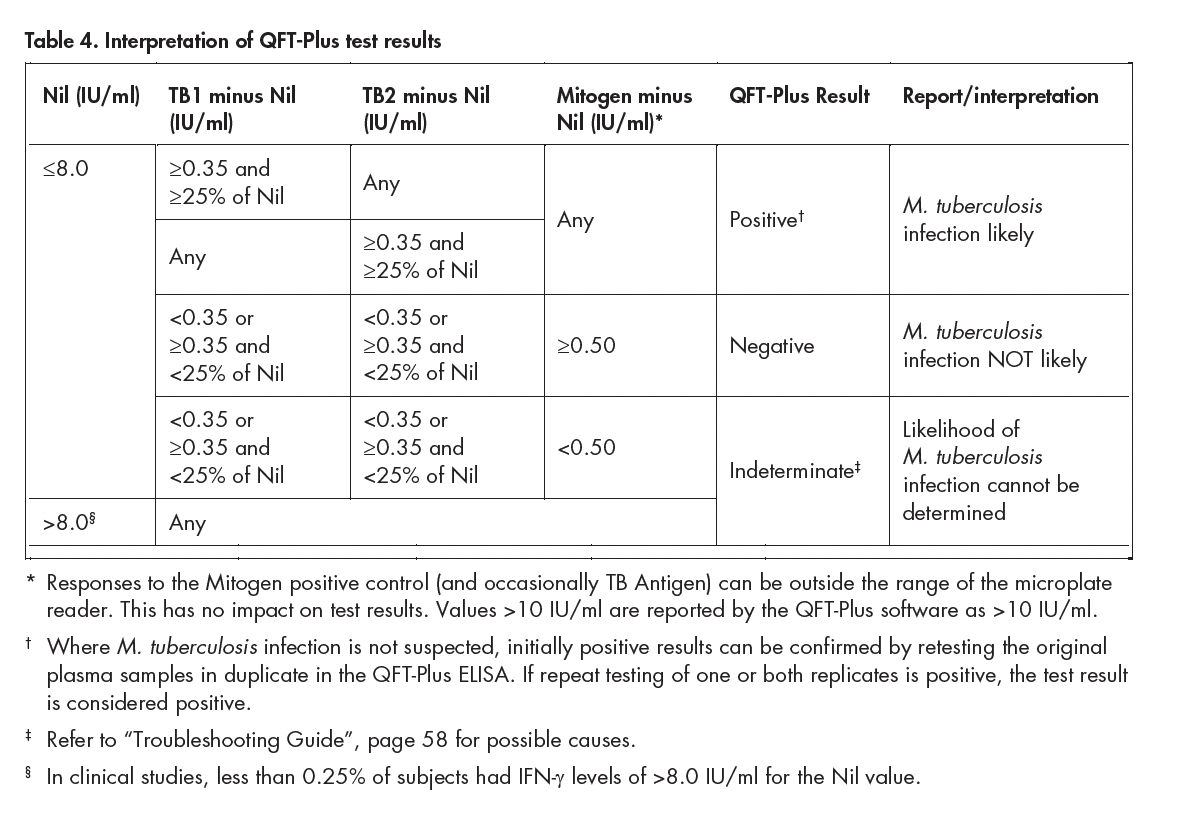
You may have noticed the “indeterminate” interpretation. Essentially, if this is the result, one of two things happened:
- You have too much IFN being released without stimulus, suggesting a chronic illness and makes interpretation difficult, as the TB stimulation may not matter in this scenario (aka the nil is too high)
- You are immunosuppressed and cannot mount a response (aka the mitogen was negative)
In other words, if you have an indeterminate result, it may be a sign of a bad immune system for whatever reason.
What is the deal with CD8?
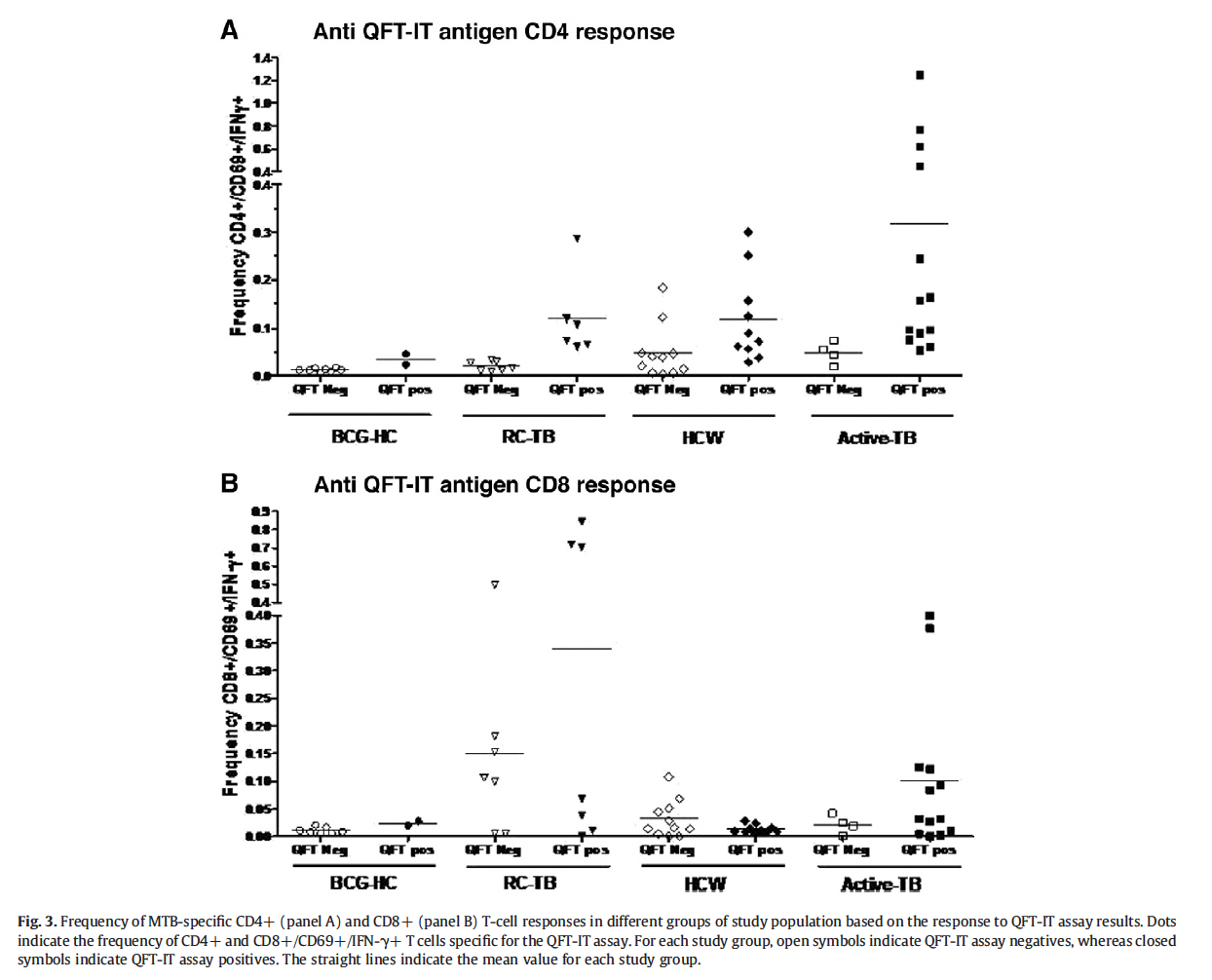
The idea of the Quantiferon-Gold Plus (plus, since it has that extra tube) is to improve the sensitivity by specifically targeting CD8- T-cells. As highlighted above, both CD4 and CD8 play a crucial role in the control of bacillary burden, which unfortunately goes over my understanding. Nevertheless, it is an interesting literature. In a cross sectional study, analysis of CD4+ T cells revealed that response to QFT-IT antigens was directly correlated to antigen burden, with frequency of response being higher in active TB patients compared to family contacts of patients with tuberculosis (8):
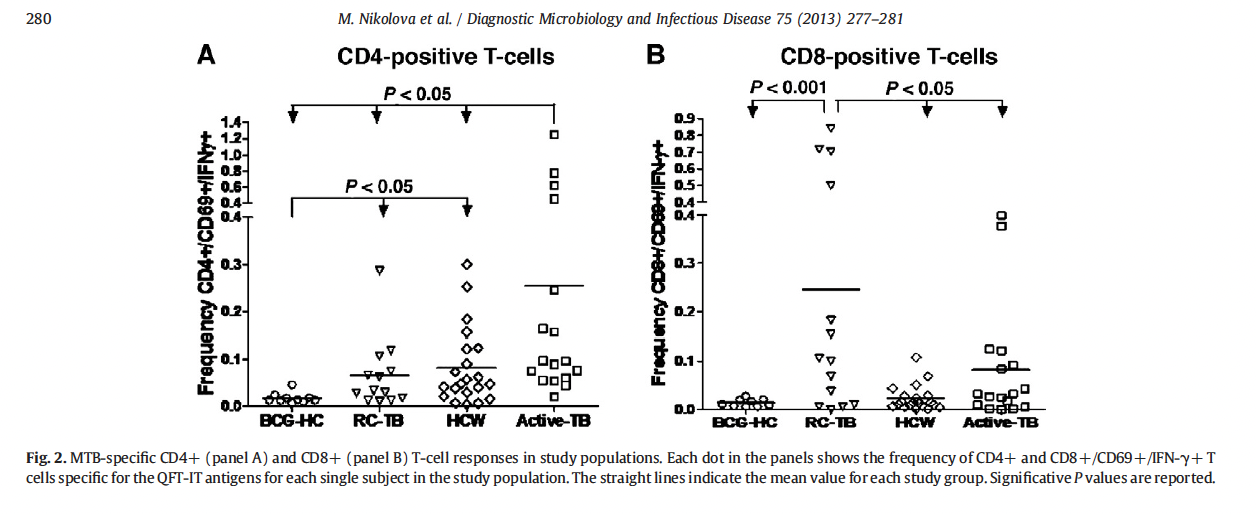
As above, this was in contrast to the proportion of CD8 positive cells that reacted in the family contact cohort, suggesting CD8 may be a marker of exposure. Indeed, the CD8 response was more vigorous in the recently exposed cohort when compared to the CD4, which is more active for active TB:
In another cohort study, CD8 T-cell response was higher in patients who had active tuberculosis (9):

Moreover, those who had smear positive sputum also had a higher magnitude of CD8 T-cell response, which was also seen in patients who had pulmonary tuberculosis:
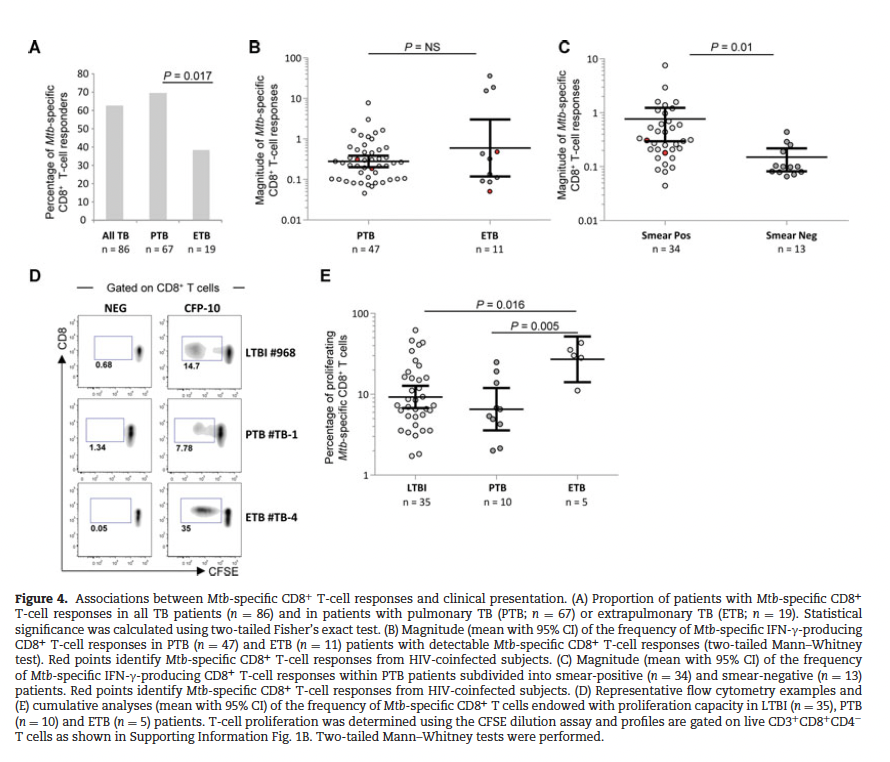
In other words, those with active pulmonary tuberculosis who may have immunodeficiency and those who were recently exposed, who may not have enough time to mount that classic response, may be picked up by the IGRA. It should be noted, however, these tests do not tell active from latent tuberculosis.
So how well do these perform?
There are multiple meta-analyses that suggest both the T-spot and quantiferon actually perform fairly well throughout several populations. One review notes high sensitivity and specificity for both types of tests (10):
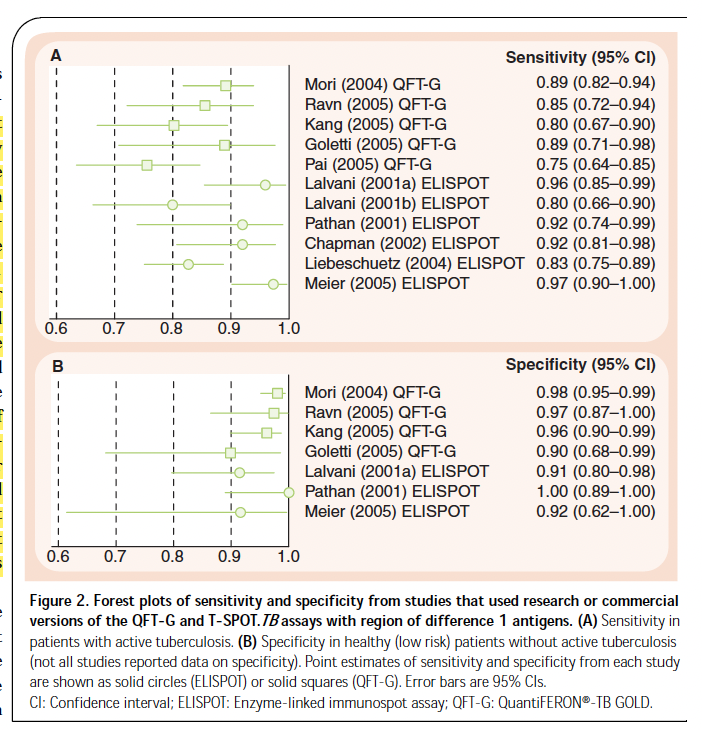
In looking at latent tuberculosis, another meta-analysis by Pai et al (11) of 22 studies evaluated their diagnostic ability in low-risk countries. Pooled sensitivity for Quantiferon studies was 76%. When looking at the specific assays, the TB-Gold assay had a sensitivity of 78% and TB-Gold in Tube had a sensitivity of 70% and T-spot had a sensitivity of 90%:

Despite this, the specificity was high throughout all studies, regardless of whether the population was BCG-vaccinated or not:

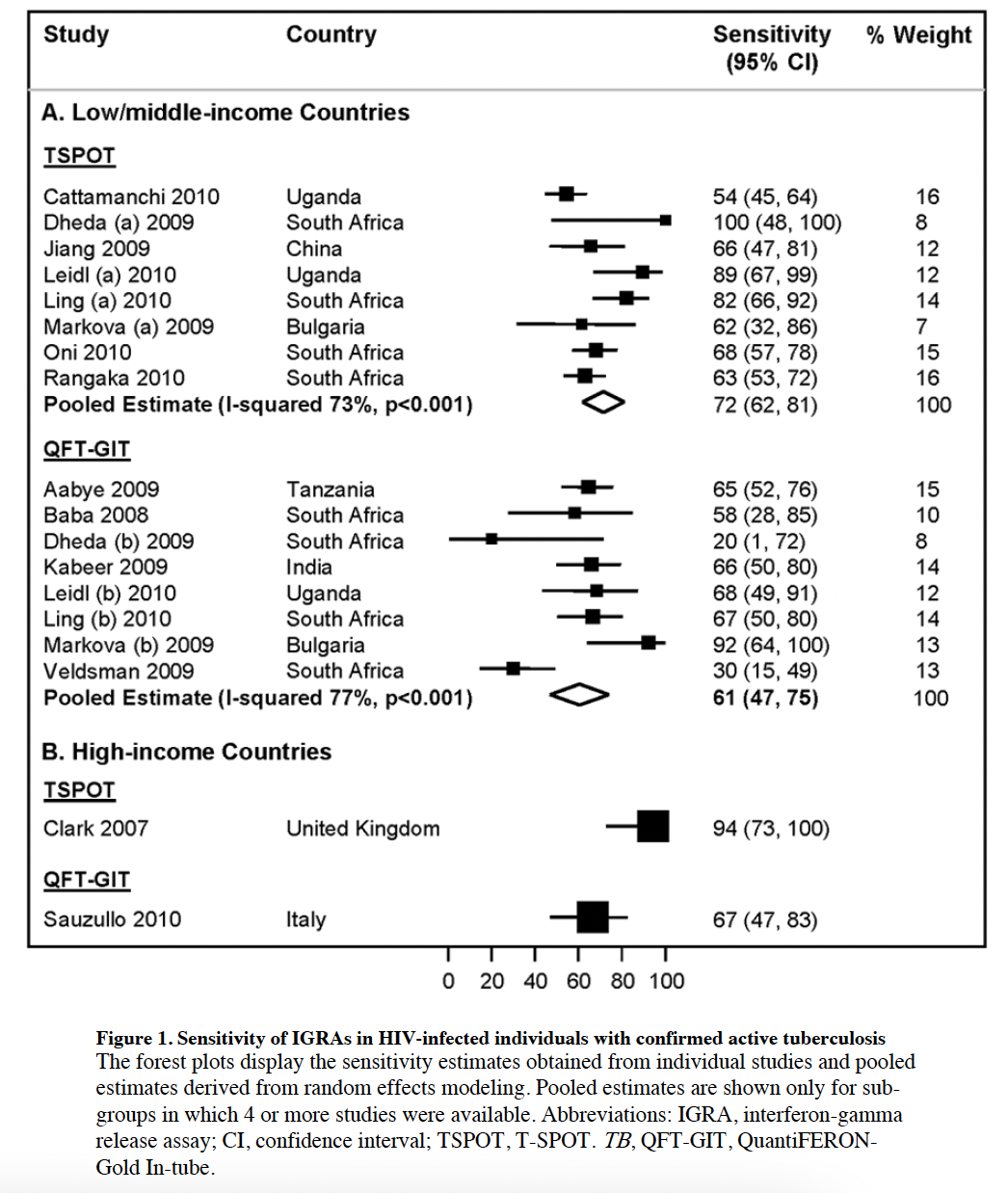
29 studies in latent TB testing for HIV patients (12) found that sensitivity for T-spot was higher in low/middle income studies when compared to the QFT-GIT (72% vs 60%), as well as in high-income countries (94% vs 67%).
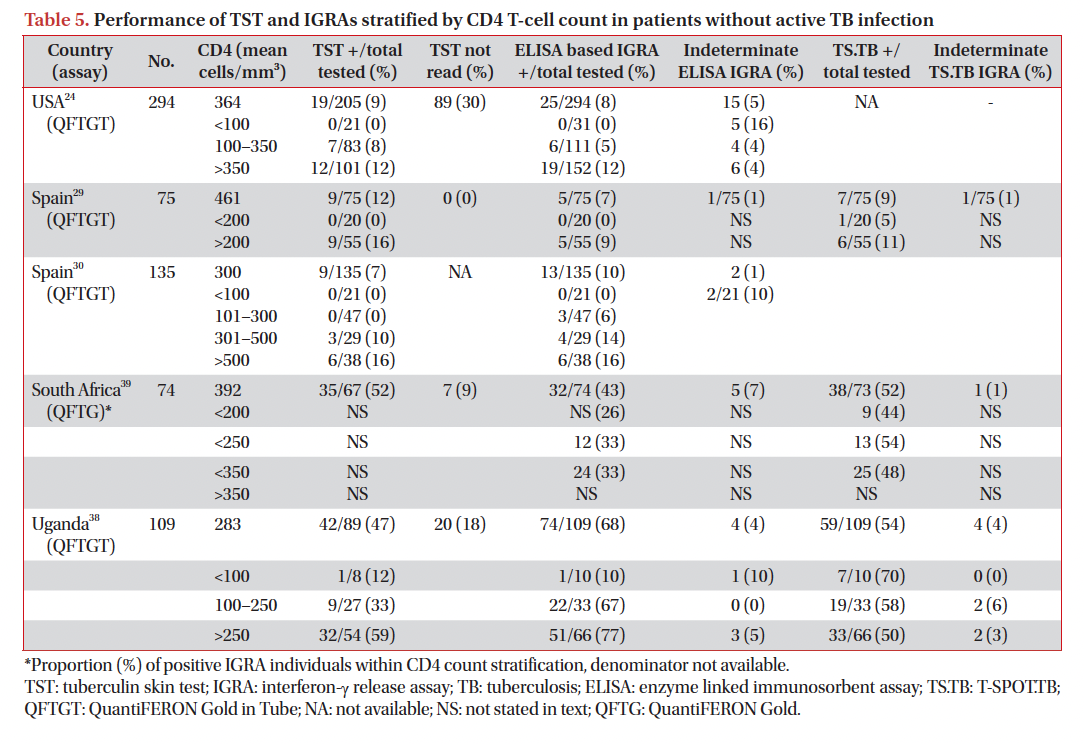
Interestingly, this meta-analysis evaluated the impact of immunosuppression on IGRA results. Overall, the proportion of positive tests were significantly lower when CD4 counts were under 200. Here, the studies compare the difference in proportion of positive IGRAs when comparing those with CD4 >200 and those whose is <100:

A review of 35 studies found that both T-spot and QTF-G had high sensitivities in areas of low-risk (13):

Similarly, using non-TB patients as controls, both test performed fairly well for latent TBI:

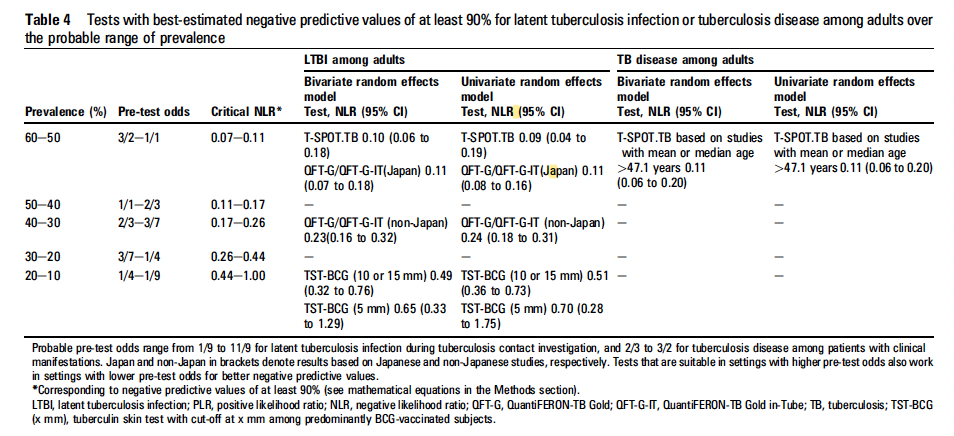
It appears the best utility for this test is within its NLR, with the T-spot test being able to rule out TB in 90% of patients, provided the prevalence of disease is anywhere from 50-60%:
So it does fairly well in latent TB, all things considered. Can it be used for active tuberculosis, however? The sensitivity of IGRAs in active tuberculosis was evaluated in a review by Pai and Colford. TST-based IGRAs tended to have a higher sensitivity than the more specific IGRAs (7):

Moreover, the agreement between TST and IGRAs was roughly 60-80% in the studies reviewed. A meta-analysis of 19 studies found the sensitivity and specificity for the T-spot test in active pulmonary tuberculosis to be 83% and 61%, respectively in low to middle-income countries, compared to a sensitivity of 69% and specificity of 52% for the QFT-GIT (14). In HIV patients, the T-spot had a higher sensitivity than QTF-GIT (76% vs 60%). Not surprisingly, both tests performed better in terms of sensitivity when looking at HIV-uninfected patients:

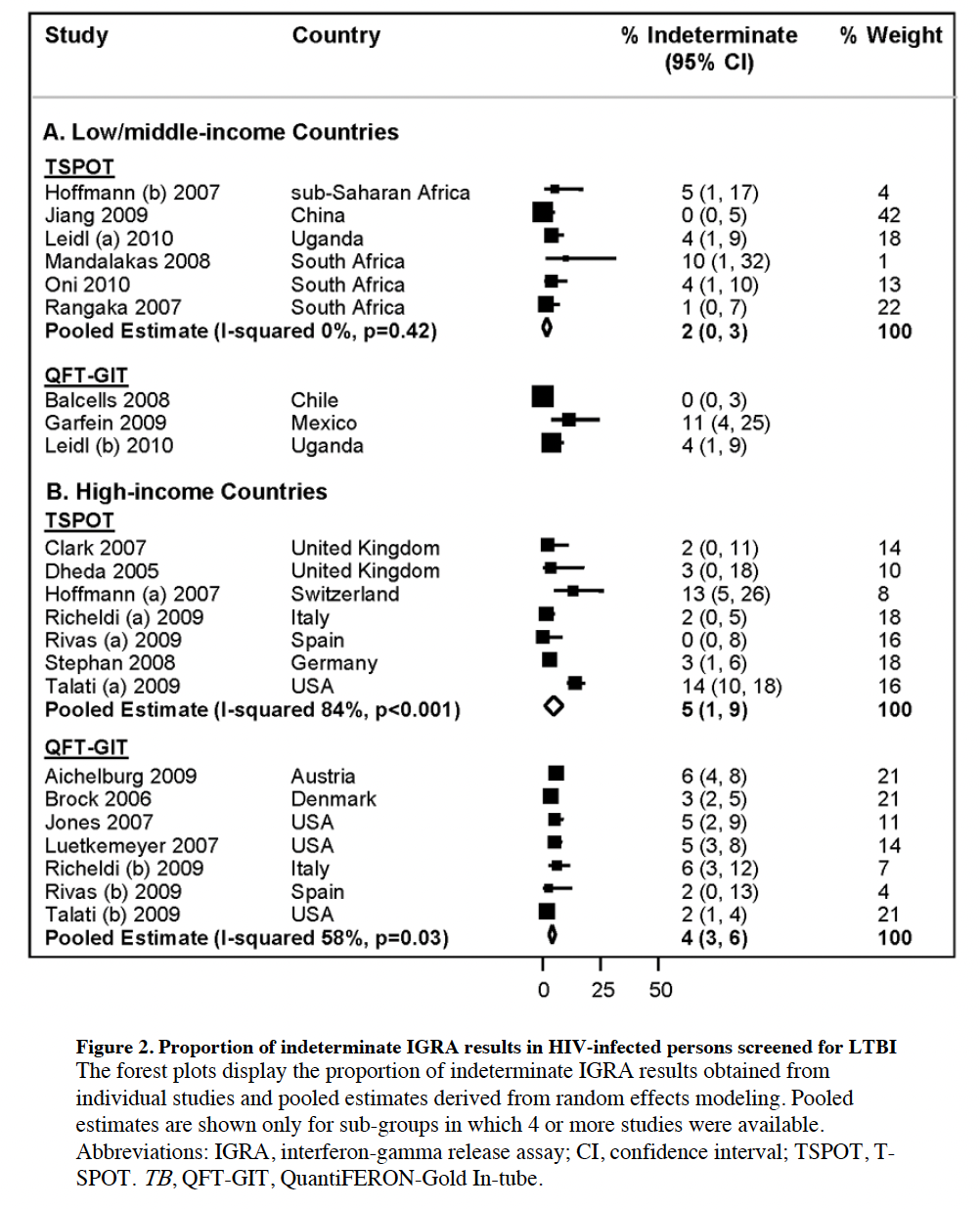
Further, indeterminate results were more prevalent in HIV-positive patients (15% for QTF-GIT vs 9% for T-spot).
A similar meta-analysis of 27 studies evaluating IGRAs for active TB actually evaluated its use in other specimens including ascites, BAL, CSF, and pericardial fluid (15). For blood QTF-G-IT, the pooled sensitivity and specificity was 80% and 79%, respectively, with pooled OR 11.5 (95% CI 5.1-27.7). For the blood T-spot, the pooled sensitivity/specificity was 81% and 83%, respectively, with pooled OR of 18.86 (95% CI 8.7-40.7), suggesting that T-spot in blood samples were more sensitive for the diagnosis of active TB. When looking at extrapulmonary samples, both sensitivity/specificity were significantly lower than that for blood samples, at least for QTF-G-IT:
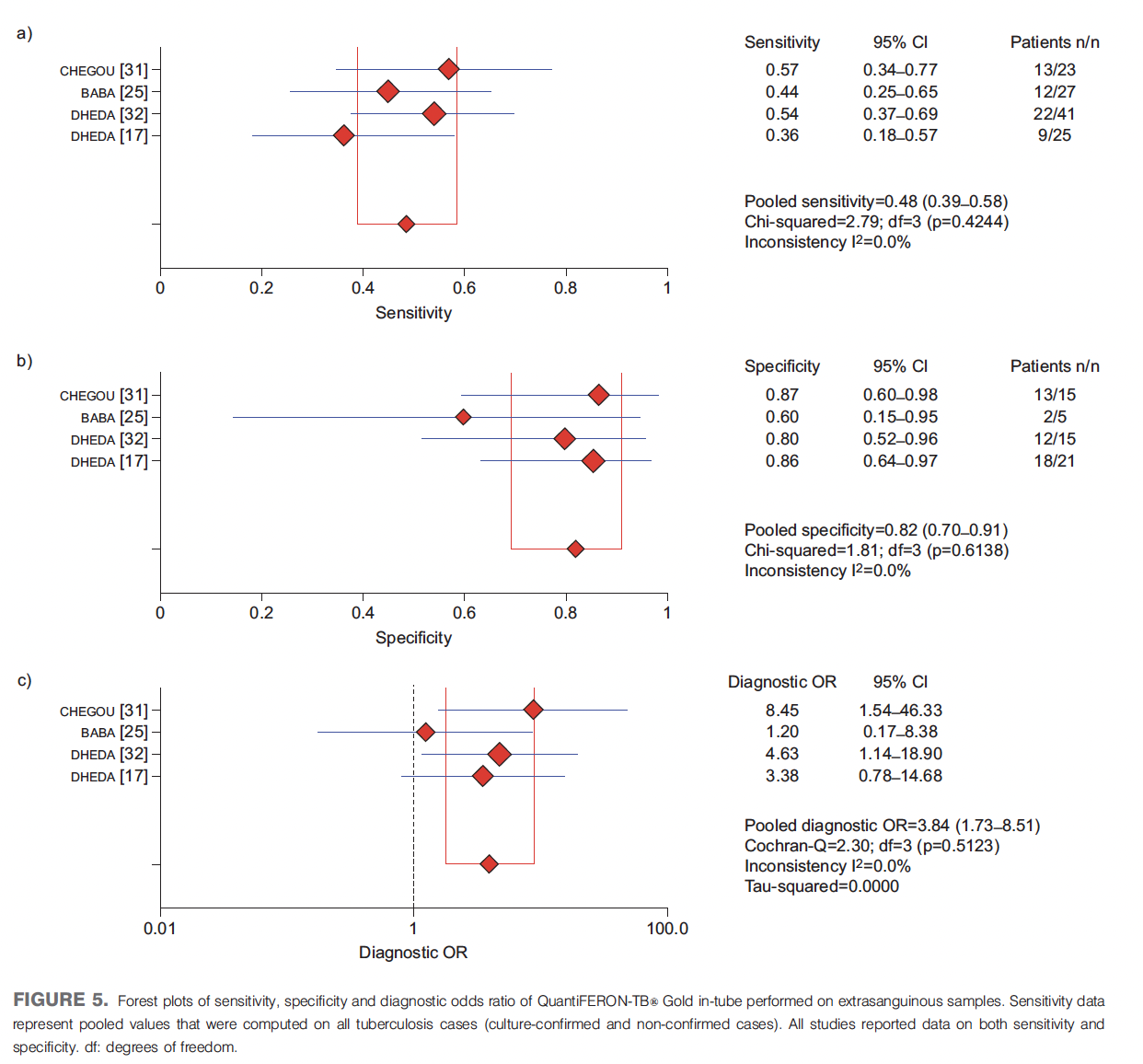
In this area, T-spot actually has a higher sensitivity than QTF-G-IT, as well as higher pooled diagnostic OR:

Performance in HIV
Not surprisingly, this has also been looked at in several meta-analysis and cohort studies.
In a cohort of 108 patients with pulmonary tuberculosis (16), the sensitivity of QTF-plus was similar in HIV-positive patients and HIV negative patients (85% for negative vs 80% for positive, p=0.59). The sensitivity, however, was correlated with CD4 counts as the sensitivity dropped to 50% with CD4 <100. Univariate analysis found that low BMI and CD4 <100 were associated with decreased odds of a positive result:

A meta-analysis of 32 studies with 4856 HIV patients found that QTF-GIT had a similar rate of reactivity to TST for active tuberculosis, however when it came to latent TB, there was little agreement between TST and IGRAs (17). Notably, the sensitivity of IGRAs was based on the degree of immunosuppression as evidenced by the CD4 count at the time of diagnosis:
In a cohort of 465 patients, of which 167 had active HIV infection, QTF-plus achieved a sensitivity of 80% for LTBI, however while sensitivity was not different between HIV-positive and HIV-negative folks, more people in the former group had indeterminate results (18):
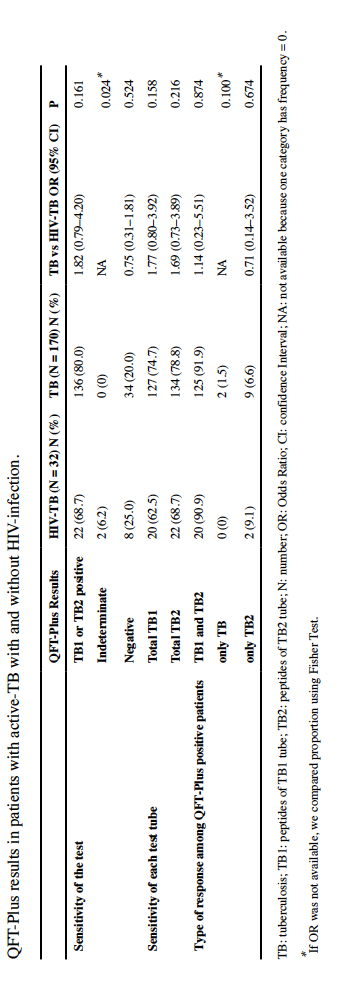
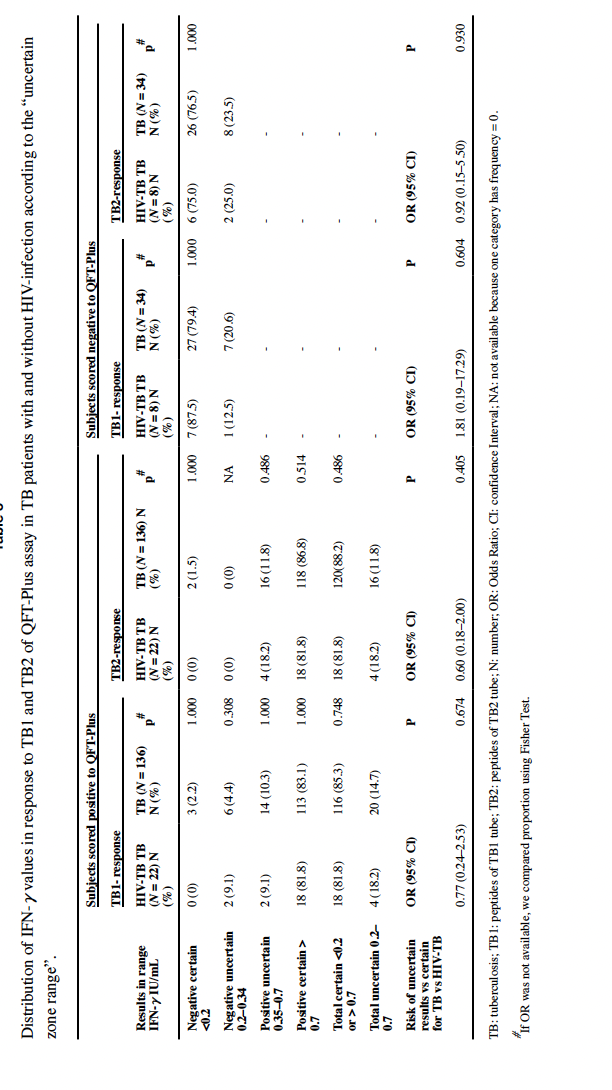
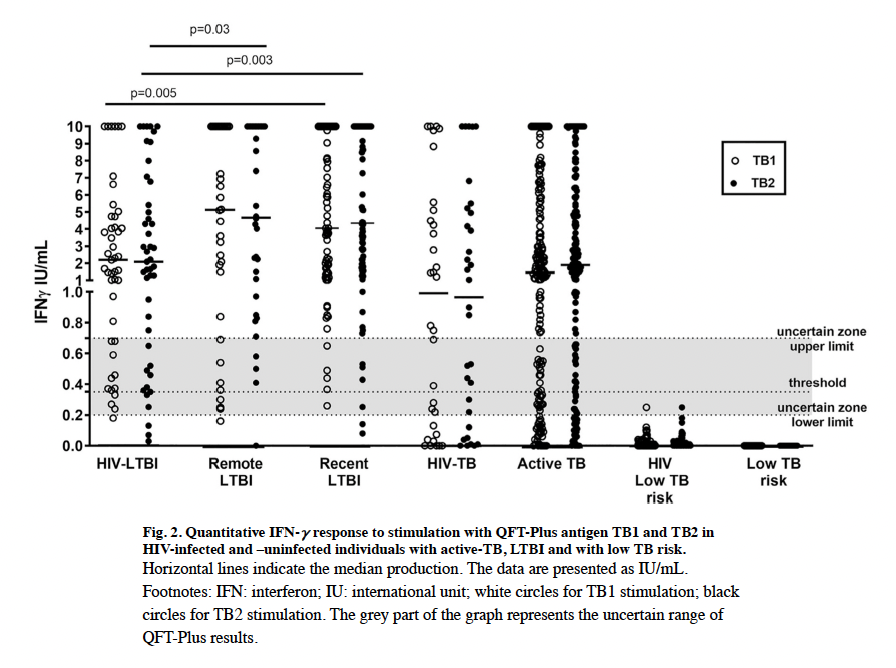
Moreover, HIV infection had no impact on the rate of positive responses for IFN-gamma values:
Interestingly, this study did not find any impact on CD4 counts and the IGRA results, either by univariate logistic regression or a Spearman correlation.

For latent TB, both recent and remote acquisition demonstrated similar responses as those who had HIV, however timing and HIV infection does play a role in whether or not a test was discordant or not:
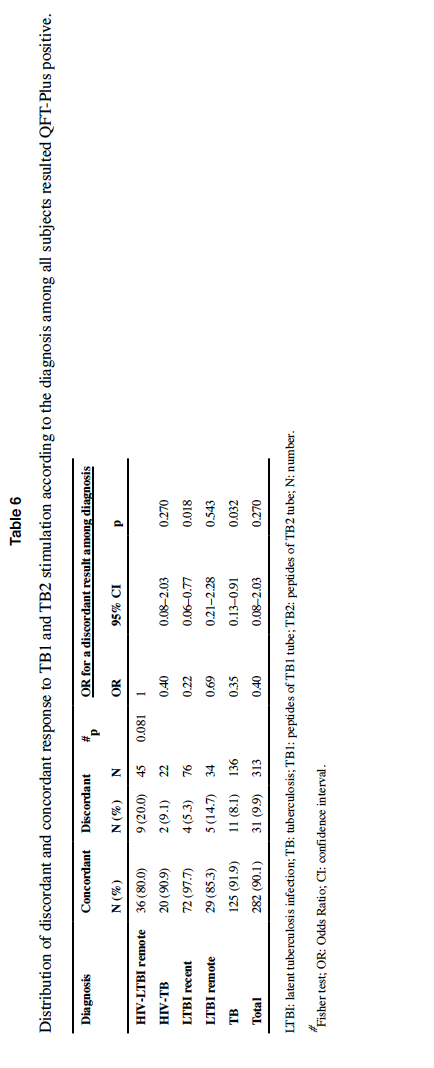
Moreover, it appears that HIV-LTBI individuals produced lower IFN-gamma when compared to LTBI patients:
The Fourth Generation:
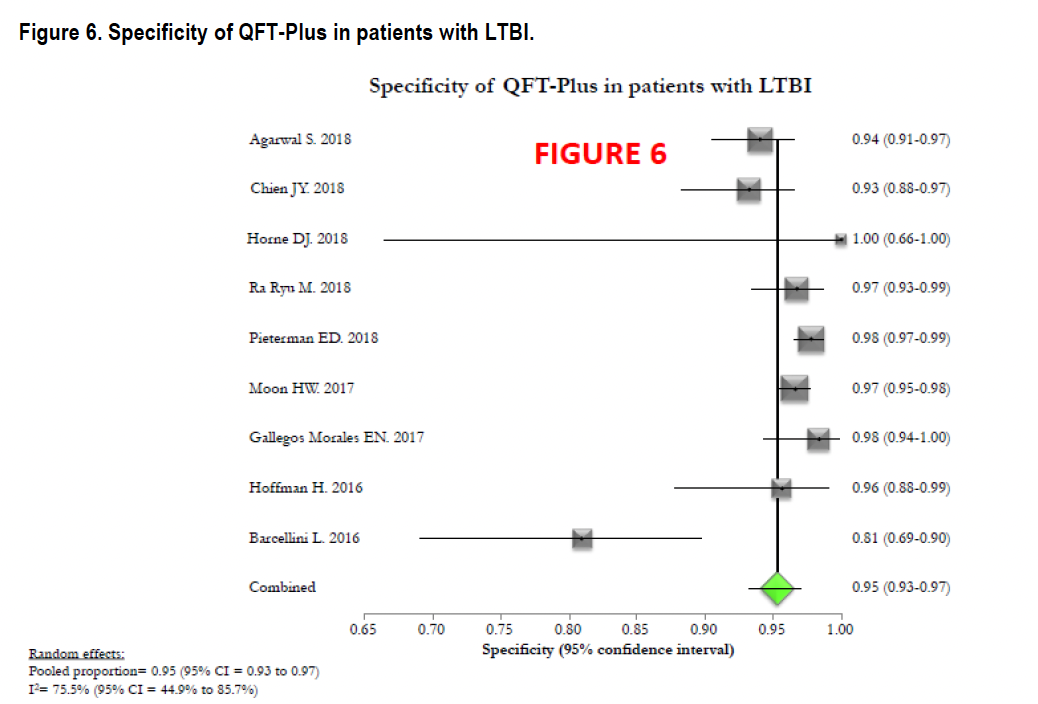
If your shop doesn’t have a T-spot, then it is likely carrying the QTF-TB GOLD PLUS, or QTF-Plus. Again, this is the test with the four tubes I mentioned earlier. Across multiple scenarios, it seems to perform as well as the previous generations, though it lags behind T-spot. A meta-analysis of 15 studies evaluated the 4th generation Quantiferon, QTF-TB Gold Plus (19). The sensitivity of QTF-Plus for both active TB and LTBI was high, above 90%:


A meta-analysis of 12 studies compared both QFT vs QFT-plus in multiple scenarios (20). Not surprisingly, more patients who got the QTF-plus were positive than QTF-GIT in cured TB cases (82% vs 73%), as well as the proportion resulting positive for TB, though this was not statistically significant (95% vs 93%). Moreover, QTF-Plus had higher sensitivity in those over the age of 75. Overall, QTF-plus had a fairly high sensitivity and specificity when looking at all the studies within this meta-analysis:

In immunocompromised patients, the agreement between QTF-plus and QFT-GIT assays was fairly high (21):

TL;DR
- Diagnosis for latent TB is based on complicated immunology
- TST is based on delayed-hypersensitivity reaction using a purified protein derivative that shares antigens with multiple other mycobacteria as well as BCG and requires two visits
- IGRAs measure amount of interferon released after your blood is exposed to TB antigens
- IGRAs use “cleaner” antigens, ESAT-6 and CFP-10, but it is shared among other antigens such as M. bovis, M. kansasii, and M.marinum

References:
- Dheda K, Schwander SK, Zhu B, van Zyl-Smit RN, Zhang Y. The immunology of tuberculosis: from bench to bedside. Respirology. 2010 Apr;15(3):433-50. doi: 10.1111/j.1440-1843.2010.01739.x. PMID: 20415982; PMCID: PMC5463744.
- Pai M, Behr M. Latent Mycobacterium tuberculosis Infection and Interferon-Gamma Release Assays. Microbiol Spectr. 2016 Oct;4(5). doi: 10.1128/microbiolspec.TBTB2-0023-2016. PMID: 27763261.
- Boom WH, Canaday DH, Fulton SA, Gehring AJ, Rojas RE, Torres M. Human immunity to M. tuberculosis: T cell subsets and antigen processing. Tuberculosis (Edinb). 2003;83(1-3):98-106. doi: 10.1016/s1472-9792(02)00054-9. PMID: 12758197.
- Trajman A, Steffen RE, Menzies D. Interferon-Gamma Release Assays versus Tuberculin Skin Testing for the Diagnosis of Latent Tuberculosis Infection: An Overview of the Evidence. Pulm Med. 2013;2013:601737. doi: 10.1155/2013/601737. Epub 2013 Feb 7. PMID: 23476763; PMCID: PMC3582085.
- Arend SM, van Meijgaarden KE, de Boer K, de Palou EC, van Soolingen D, Ottenhoff TH, van Dissel JT. Tuberculin skin testing and in vitro T cell responses to ESAT-6 and culture filtrate protein 10 after infection with Mycobacterium marinum or M. kansasii. J Infect Dis. 2002 Dec 15;186(12):1797-807. doi: 10.1086/345760. Epub 2002 Nov 19. PMID: 12447766.
- QuantiFERON-TB Gold Plus (QFT-Plus) Package Insert 06/2022
- Pai M, Riley LW, Colford JM Jr. Interferon-gamma assays in the immunodiagnosis of tuberculosis: a systematic review. Lancet Infect Dis. 2004 Dec;4(12):761-76. doi: 10.1016/S1473-3099(04)01206-X. PMID: 15567126.
- Nikolova M, Markova R, Drenska R, Muhtarova M, Todorova Y, Dimitrov V, Taskov H, Saltini C, Amicosante M. Antigen-specific CD4- and CD8-positive signatures in different phases of Mycobacterium tuberculosis infection. Diagn Microbiol Infect Dis. 2013 Mar;75(3):277-81. doi: 10.1016/j.diagmicrobio.2012.11.023. Epub 2012 Dec 28. PMID: 23276770.
- Rozot V, Vigano S, Mazza-Stalder J, Idrizi E, Day CL, Perreau M, Lazor-Blanchet C, Petruccioli E, Hanekom W, Goletti D, Bart PA, Nicod L, Pantaleo G, Harari A. Mycobacterium tuberculosis-specific CD8+ T cells are functionally and phenotypically different between latent infection and active disease. Eur J Immunol. 2013 Jun;43(6):1568-77. doi: 10.1002/eji.201243262. PMID: 23456989; PMCID: PMC6535091.
- Pai M, Kalantri S, Dheda K. New tools and emerging technologies for the diagnosis of tuberculosis: part I. Latent tuberculosis. Expert Rev Mol Diagn. 2006 May;6(3):413-22. doi: 10.1586/14737159.6.3.413. PMID: 16706743.
- Pai M, Zwerling A, Menzies D. Systematic review: T-cell-based assays for the diagnosis of latent tuberculosis infection: an update. Ann Intern Med. 2008 Aug 5;149(3):177-84. doi: 10.7326/0003-4819-149-3-200808050-00241. Epub 2008 Jun 30. PMID: 18593687; PMCID: PMC2951987.
- Cattamanchi A, Smith R, Steingart KR, Metcalfe JZ, Date A, Coleman C, Marston BJ, Huang L, Hopewell PC, Pai M. Interferon-gamma release assays for the diagnosis of latent tuberculosis infection in HIV-infected individuals: a systematic review and meta-analysis. J Acquir Immune Defic Syndr. 2011 Mar 1;56(3):230-8. doi: 10.1097/QAI.0b013e31820b07ab. PMID: 21239993; PMCID: PMC3383328.
- Chang KC, Leung CC. Systematic review of interferon-gamma release assays in tuberculosis: focus on likelihood ratios. Thorax. 2010 Mar;65(3):271-6. doi: 10.1136/thx.2009.126771. PMID: 20335301.
- Metcalfe JZ, Everett CK, Steingart KR, Cattamanchi A, Huang L, Hopewell PC, Pai M. Interferon-γ release assays for active pulmonary tuberculosis diagnosis in adults in low- and middle-income countries: systematic review and meta-analysis. J Infect Dis. 2011 Nov 15;204 Suppl 4(Suppl 4):S1120-9. doi: 10.1093/infdis/jir410. PMID: 21996694; PMCID: PMC3192542.
- Sester M, Sotgiu G, Lange C, Giehl C, Girardi E, Migliori GB, Bossink A, Dheda K, Diel R, Dominguez J, Lipman M, Nemeth J, Ravn P, Winkler S, Huitric E, Sandgren A, Manissero D. Interferon-γ release assays for the diagnosis of active tuberculosis: a systematic review and meta-analysis. Eur Respir J. 2011 Jan;37(1):100-11. doi: 10.1183/09031936.00114810. Epub 2010 Sep 16. Erratum in: Eur Respir J. 2012 Mar;39(3):793. PMID: 20847080.
- Telisinghe L, Amofa-Sekyi M, Maluzi K, Kaluba-Milimo D, Cheeba-Lengwe M, Chiwele K, Kosloff B, Floyd S, Bailey SL, Ayles H. The sensitivity of the QuantiFERON®-TB Gold Plus assay in Zambian adults with active tuberculosis. Int J Tuberc Lung Dis. 2017 Jun 1;21(6):690-696. doi: 10.5588/ijtld.16.0764. PMID: 28482964; PMCID: PMC5424670.
- Overton K, Varma R, Post JJ. Comparison of Interferon-γ Release Assays and the Tuberculin Skin Test for Diagnosis of Tuberculosis in Human Immunodeficiency Virus: A Systematic Review. Tuberc Respir Dis (Seoul). 2018 Jan;81(1):59-72. doi: 10.4046/trd.2017.0072. Epub 2017 Dec 13. PMID: 29256218; PMCID: PMC5771747.
- Petruccioli E, Chiacchio T, Navarra A, Vanini V, Cuzzi G, Cimaglia C, Codecasa LR, Pinnetti C, Riccardi N, Palmieri F, Antinori A, Goletti D. Effect of HIV-infection on QuantiFERON-plus accuracy in patients with active tuberculosis and latent infection. J Infect. 2020 May;80(5):536-546. doi: 10.1016/j.jinf.2020.02.009. Epub 2020 Feb 22. PMID: 32097688; PMCID: PMC8862140.
- Sotgiu G, Saderi L, Petruccioli E, Aliberti S, Piana A, Petrone L, Goletti D. QuantiFERON TB Gold Plus for the diagnosis of tuberculosis: a systematic review and meta-analysis. J Infect. 2019 Nov;79(5):444-453. doi: 10.1016/j.jinf.2019.08.018. Epub 2019 Aug 29. PMID: 31473271.
- Pourakbari B, Mamishi S, Benvari S, Mahmoudi S. Comparison of the QuantiFERON-TB Gold Plus and QuantiFERON-TB Gold In-Tube interferon-γ release assays: A systematic review and meta-analysis. Adv Med Sci. 2019 Sep;64(2):437-443. doi: 10.1016/j.advms.2019.09.001. Epub 2019 Oct 3. PMID: 31586819.
- Xu Y, Yang Q, Zhou J, Zhou F, Hezhang Y, Gao Y, Shao L, Shi J, Ruan Q, Zhang W. Comparison of QuantiFERON-TB Gold In-Tube and QuantiFERON-TB Gold-Plus in the Diagnosis of Mycobacterium tuberculosis Infections in Immunocompromised Patients: a Real-World Study. Microbiol Spectr. 2022 Apr 27;10(2):e0187021. doi: 10.1128/spectrum.01870-21. Epub 2022 Mar 2. PMID: 35234509; PMCID: PMC9045206.
