
Well, this is new territory. While I typically talk about esoteric/topics infectious diseases docs should be aware of (see: my recent posts on complicated SAB, prior topics tackling dosing of vancomycin and beta-lactamase inhibitors, and acute katayama fever, as examples) I occasionally delve into other more mundane topics (see: neutrophil-lymphocyte ratio). This one is a doozy. It’s all about septic shock. The powers that be tell us we need to meet metrics for billing purposes (i.e. 30cc/kg of IV fluids if you get flagged as “sepsis” by your EMR), the foundation of these recommendations is shaky, to be generous.
Why We Give Fluids:
It should be noted that sepsis and septic shock is not a hypovolemia issue, though there is a component of that due to poor PO intake, GI loss, or insensible losses. Indeed, it appears that a dysregulation of the host immune system (i.e. pro-inflammatory markers are upregulated in response to an organism and tissue injury while anti-inflammatory signals that lead to apoptosis of certain cell lines are decreased) end up in the balance of pro-inflammation (1). Moreover, vascular endothelium, which is composed of an endothelial glycocalyx that is negatively charged and maintains a barrier between the vasculature and the interstitium is shed due to inflammation and ischemia, leading to extravasation of fluid and activation of coagulation. Hemodynamic changes tend to be a combination of hypovolemia, vasodilatation, depressed myocardial function due to acidosis/inflammation, and extravasation that leads to vasoplegia in sepsis. Moreover, in the microcirculation, there is a heterogeneity of vessel density and distribution; ie. Some vessels may be worse off than others, but this does not necessarily mean there is tissue hypoperfusion, but rather a change in oxygen utilization throughout the body (1).
The idea behind the use of IV fluids for sepsis is highlighted in a review by Feihl and Broccard (2). In general, the flow of venous return (i.e. QRV) is correlated to cardiac output. In other words, preload aka venous return = cardiac output. Since it is believed that septic shock is an issue of oxygen delivery, an increase in cardiac output is meant to match the requirement for more oxygen throughout the body (this is not necessarily the case, but it is the foundation behind EGDT). In other words, if we maximize cardiac output, we also increase oxygen delivery. We do so by increasing preload. As we can see, preload aka systemic flow is related to the mean systemic filling pressure minus the right atrial pressure, and inversely proportional to the vascular resistance (RV).
QRV = (MSFP – RAP)/Rv
In other words, the more the filling pressure aka preload and lower atrial pressure results in higher flow of venous return:

In sepsis, activation of endogenous catecholamines lead to increased vascular tone and thus, more stressed volume. The body automatically increases the mean systolic filling pressure on its own, however at some point, the amount of stressed volume will decrease since there is a limited number of volume in the vasculature. Here’s where IVF comes in; if we increase MSFP, we thus increase preload and cardiac output.
But there is a balance, if the venous return increases while the vascular resistance is the same, then this inherently increases right atrial pressure, which leads to a drop in flow, meaning adding more venous return (i.e. more MSFP) in setting of a constant vessel resistance (Rv) means RAP will also increase, leading to a drop in flow rate. Or to put it simply, there is a limit to how much venous return will lead to a rise in preload:

In the above graph (D), point a is someone operating at a lower cardiac output state. Compared to point d, point a has a lower RAP that allows it to maintain venous return flow (see above formula). However, increasing venous return allows that individual to go to point b, where they optimize their preload to augment their cardiac output (i.e. they’re at a better point in their own Frank-Starling curve). All this to say, fluids in sepsis are meant to improve cardiac output in a setting where flow of blood is directed by the difference between the pressure in the right atrium and the superior vena cava, which is related to the vascular resistance. If cardiac function, systemic vascular resistance, and preload are not physiologically deranged, giving IV fluids would increase MSFP and thus, preload and cardiac output. This, of course, assumes all fluids going into vessels stay within the vessels, which is not true in sepsis and septic shock.
The other issue is the fact that in sepsis, the vasculature is not a closed system due to its “leaky” nature and extravasation. Further, there are other physiologic derangements that may factor into the maintenance of mean arterial pressure. For instance, a cohort of 262 patients with septic shock found that diastolic dysfunction, which was measured by the E-wave acceleration time, was fairly prevalent (3). Reduced e-waves (i.e. more diastolic dysfunction) was associated with overall mortality:

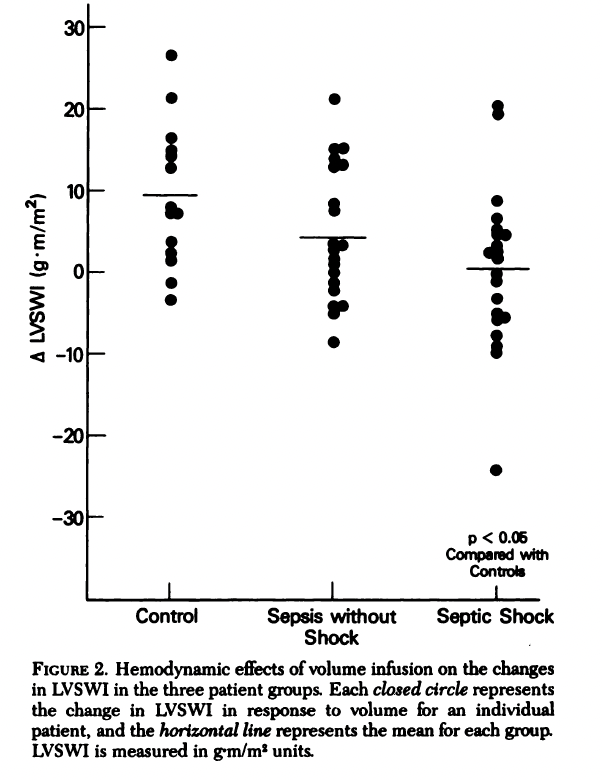
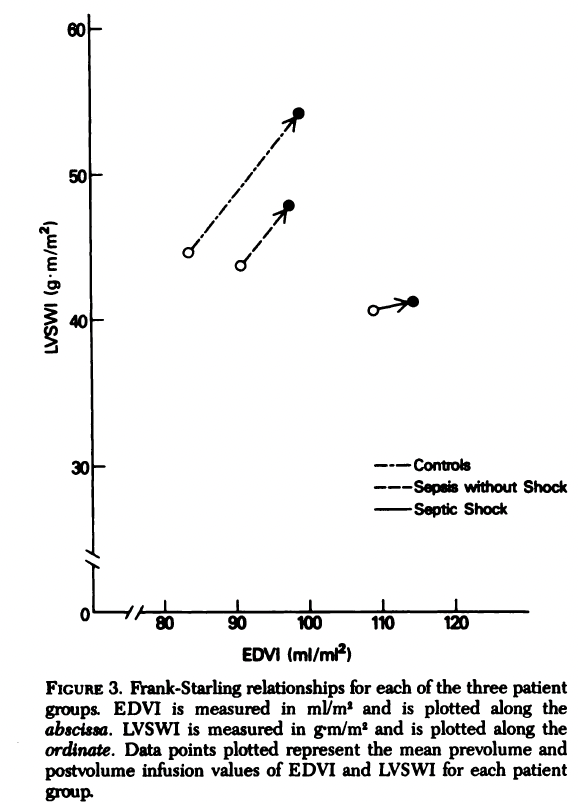
In other words, diastolic dysfunction is correlated with increased mortality in septic shock, which may impact the response to fluid boluses in these patients. This was also confirmed in a study of 56 patients divided into either control subjects, those with sepsis but without shock, and those with septic shock (4). End diastolic blood volume did not increase after fluid infusion in patients with septic shock when compared to control subjects:

Left ventricular systolic work indeed was similarly not different between groups after fluid infusion, suggesting that septic shock patients tend to be on the down and right area of the Frank-Starling curve:
It should be noted most patients with septic shock had more fluids given when enrolled into the study, so the preload already given to the patients may influence how they reacted to the fluid given during the study.
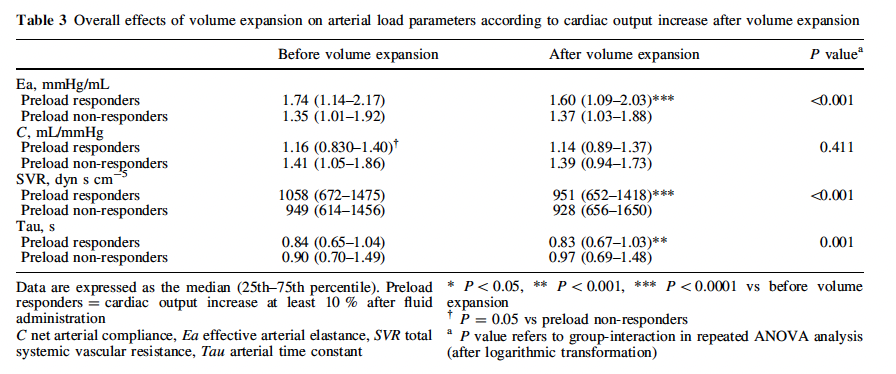
IV fluid boluses also have an impact on the afterload. One retrospective study of 81 patients (5) found that fluid administration was associated with decreased arterial elastance (from 1.68 to 1.57 mmHg/mL) and SVR (from 1035 to 928). In other words, it decreased the increased vascular tone seen in sepsis, which could be a function of improving cardiac output. This is seen in patients who responded adequately to IVF, who tended to have a significant increase in their cardiac output despite nearly equal rise in stroke volume between both groups, though those who did not respond had higher stroke volume prior to volume resuscitation

This suggests the relationship between cardiac output and preload is not as straightforward as we would like it to be, highlighting the complexities of fluid resuscitation in septic shock. Moreover, it also highlights that fluid responsiveness does not necessarily reflect an improvement in MAP, as those responded had a significant drop in SVR:
Lets not forget the increase in vascular permeability that occurs during sepsis. An interesting study used transpulmonary thermodilution to measure extravascular lung water index, intrathoracic blood volume index, and pulmonary blood volume in 18 patients with septic shock and 14 control patients (6). While the numbers and the methods are confusing, the idea is to see how much fluid remains in the vasculature in septic patients vs control patients. For instance, as you can see below, fluid boluses increased the intrathoracic blood volume in non-septic patients but not in septic patients:

It terms of numbers, the intrathoracic blood volume index was significantly lower in the septic shock patients when compared to control patients, as was the extracellular water index suggesting extravasation of fluids in septic patients:
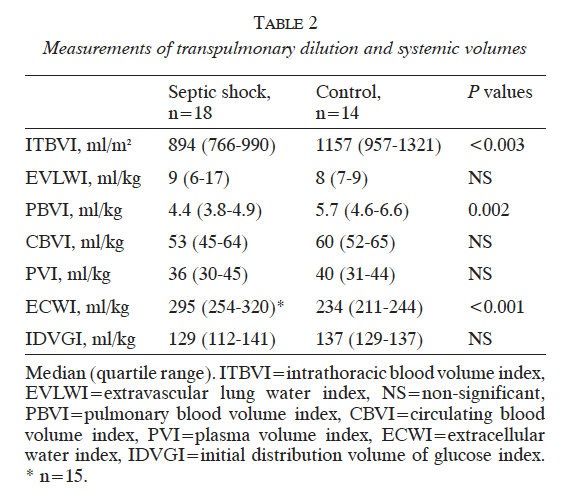
Indeed, the interstitial/plasma volume ratio was significantly higher in the septic population, suggesting more extravasation than in the control group:

Fluid Challenges:
Is there a benefit to fluid challenges? A study of 26 postoperative patients evaluated the changes following 250cc fluid boluses in several parameters, including cardiac output and MAP (7). Responders achieved the maximal effect in cardiac output after around 1 minute (1.16min) compared to around four minutes in the non-responder cohort (3.77min) although both return to near baseline after 10 minutes. A meta-analysis of 17 studies found that cardiac index increases after IV fluid boluses, however these increases would taper down throughout the course of an hour (8). This is exemplified by a quoted study evaluated hemodynamic parameters following IV boluses up to 240min after infusion:

For instance, the cardiac index increased by a median of 800 ml/min/m2 immediately post-infusion, by 300 ml/min/m2 at 30 minutes, and 300ml/min/m2 at 60 minutes. In both these studies, the range of responders was anywhere from 50 to 60%. It appears that, if someone is fluid responsive, you should be able to see within the first minute if they will respond. What’s the ideal fluid bolus then? A single-center study used different bolus doses of IVF (1cc/kg, 2cc/kg, 3cc/kg or 4cc/kg) to establish the minimal dose to produce a change in cardiac output (9). Out of 86 patients evaluated, only 41.3% were deemed fluid-responsive. Notably, the proportion of fluid responders increased with the higher dose of crystalloids:
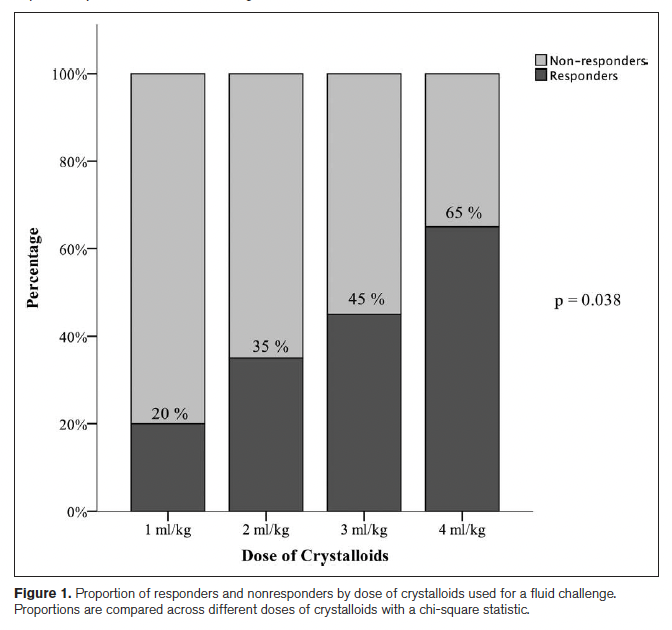
Indeed, when comparing the hemodynamic parameters, those with a 4cc/kg volume of crystalloid infusion had higher changes in MAP, CO, and SV change when compared to the 1cc/kg infusion:


However, all these patients were cardiac surgery patients without sepsis, meaning the applicability of this study is small to the patients of interest.
Early Goal Directed Therapy
I focused on fluids since it is the intervention we take the most for granted and it’s one of the core “compliance” measures people get dinged on, on top of antibiotics, cultures, and lactate measurements. Where did this idea come from? As highlighted above, the idea of IV fluids has been around for a while, prior to the advent of early-goal directed therapy, with the purpose of improving cardiac output. The optimal amount of IVF upfront is unknown, with the 2021 surviving sepsis guidelines recommending 30cc/kg despite it being a “weak recommendation with low quality evidence” (10). Unfortunately, this stems from a prior iteration of the guidelines (11) which cites one of the more controversial papers in critical care history. Yes, it’s time to talk Rivers.
This single-center randomized control trial (12) evaluated the utility of early-goal directed therapy performed within 6 hours of arrival to the ED if you had positive SIRS criteria and a SBP <90 OR lactate >4 after a fluid bolus of 20 to 30cc/kg). The protocol is as follows:
- Insert central venous catheter capable of measuring central venous oxygen saturation
- 500cc bolus every 30 minutes to achieve a goal CVP of 8-12
- Vasopressors to maintain MAP of >65
- Venodilators (i.e. dobutamine) to maintain MAP <90
- Transfuse PRBCs to maintain a HCT of at least 30 if central venous oxygen was <70%
- If the above were optimized and the central venous oxygen was still <70, you gave dobutamine
Patients were assessed every 12 hours for 72hrs, with the primary outcome being in-hospital mortality. 288 patients were evaluated, of which 263 were randomized and 236 completed the initial six-hour period. While the MAP was higher in the EGDT group, lactate measurements were similar between groups up until hour 72 of the study. In-hospital mortality was significantly lower in the EGDT group compared to the standard-of-care group:

Moreover, resuscitation end-points were similar at the end of therapy when it came to total fluids administered, however when it came to vasopressor use, mechanical ventilation, and inotropic agent, this was more often used in the EGDT group with the exception of mechanical ventilation:
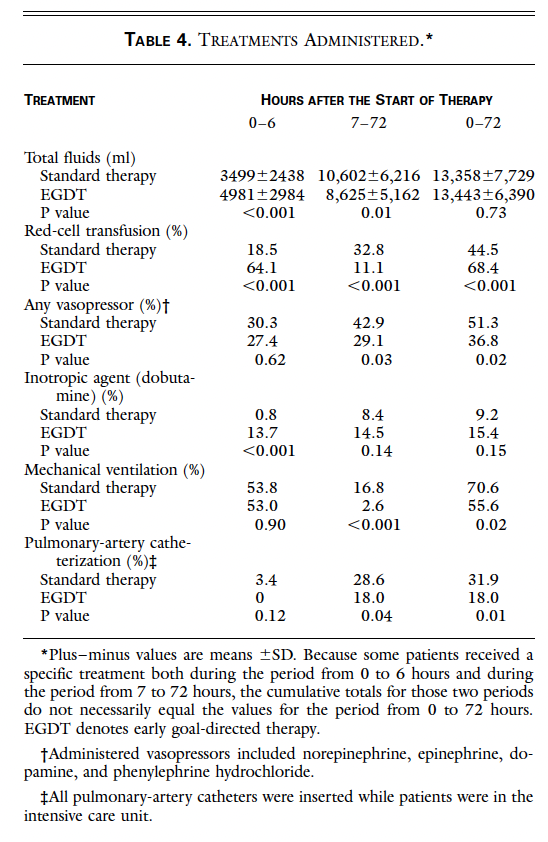
It’s easy to look at this paper in 2023 and see many interventions that do not make sense. Dobutamine? Transfusing to a hemoglobin goal of 10? Using ScvO2? But at the time, this was the best trial on resuscitation, though it is not without controversy. For instance, Rivers is listed as a consultant for the manufacturer of the ScvO2-measuring central line. Moreover, which one of the above interventions was the one that mattered the most? Also the single-center nature of it made it difficult to apply to a broad population and it seemed the usual care group had a higher than normal mortality. Of course, this formed the basis of our aggressive resuscitation guidelines, as can be seen by the absurd number of liters all these patients got.
A holy-trinity of trials seemed to shoot down the idea of early-goal directed therapy, or at least certain aspects of it. The ProCESS trial, which was a US-based multi-center, randomized, control trial that evaluated the utility of EGDT as highlighted above, compared three different groups: protocol-based EGDT (ak the Rivers protocol), protocol-based standard therapy (fluids to reach a goal of MAP or shock index, no PRBCs, no specific fluid or pressor) or standard of care (13). Primary outcome was in-hospital mortality at day 60. 1351 patients were evaluated, and 1341 were analyzed. More patients did not adhere to the protocol in the EGDT group when compared to the standard-therapy group (11.9% vs 4.4%), and fluid administration was also statistically different between groups during the first 6 hours (2.8L in EGDT group, 3.3L in protocol-based standard of care, and 2.3L in the usual care group). In-hospital and 90-day mortality did not differ between groups:

The Australasian ARISE study performed a very similar trial to that of the ProCESS (14). Here, patients who met SIRS criteria and ongoing MAP <65 or SBP <90 or lactate >4 were enrolled in a 1:1 ratio to either EGDT (including that central catheter that can measure central venous oxygen saturation) or standard of care during the first 4 hours. Primary outcome was all-cause mortality at 90 days. 1600 patients were enrolled, with 90-day mortality being similar among both groups:
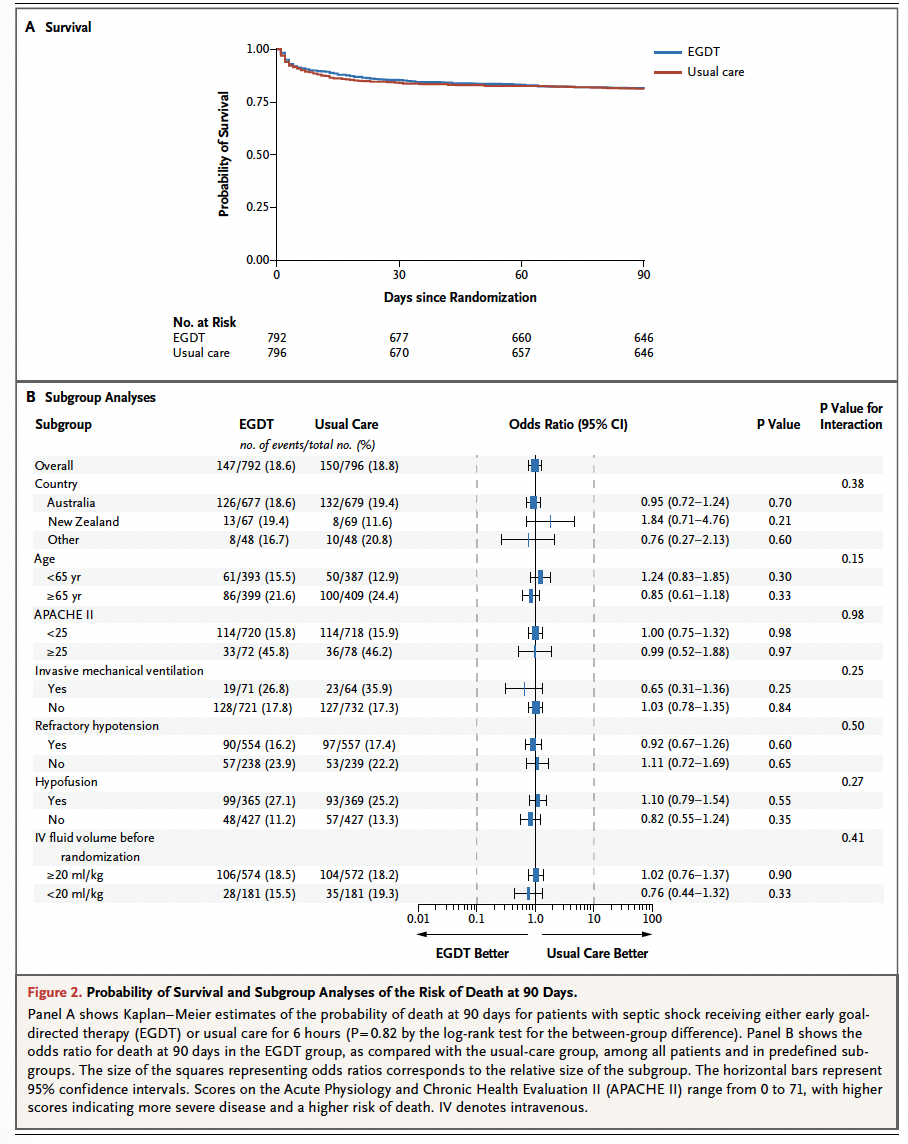
Indeed, as you can see above, there was no difference amongst all different subgroups analyzed. Notably, central venous oxygen saturation was only measured in 61% of the patients in the standard of care group compared to 93% of the EGDT group. The UK-based PROMISE trial, which was an open labe, multi-center, randomized trial, enrolled 1260 patients and found that 90-day mortality was not statistically different between the EGDT group or the standard-care group (15):

Notably, SOFA scores were higher in the EGDT group at hour 6 but this tapered off beyond the first 6 hours. More fluid was given in the first 6 hours for the EGDT group as was RBC transfusion, which is expected. Further, less than 1% of standard-therapy groups had their ScvO2 measured as part of their resuscitation. A meta-analysis of the above 3 trials (16) confirmed there was no difference in 90-day mortality between groups:
For the most part, secondary outcomes did not favor EGDT:

While the above 3 trials debunked a lot of things about EGDT, the optimal fluid resuscitation upfront remains inconclusive. ProMISE patients had a mean of 2L of IVF given prior to randomization, when compared to 2.5L in both groups of ARISE. Some insight into the initial fluid resuscitation can be gleaned from a study by Andrews et al (17). In this African non-blinded RCT of septic patients with hypotension, the authors compared their own sepsis protocol during the first 6 hours of presentation, which consisted of an initial 2L IV fluid bolus during the initial hour followed by an additional 2L over the next 4 hours. If MAP was <65, dopamine was given at 10ug/Kg and titrated. This cohort was compared to a standard of care cohort, with the primary outcome being in-hospital mortality. 212 patients were randomized, with mortality being 48.1% in the sepsis protocol group compared to 33% in the standard of care group (RR 1.46, 95% CI 1.05-2.05).
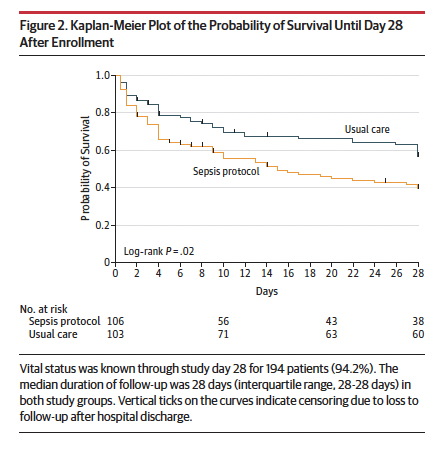
Overall, more IV fluids were given in the sepsis protocol group at hour 6 (5L vs 4L) as well as within the initial hour (3.5L vs 2L). Notably, more patients in the sepsis protocol group were more likely to have respiratory distress despite the lack of difference in lactate or blood pressure between groups, though it should be noted many of the patients in this cohort (nearly 90% in the sepsis protocol group) had HIV and dopamine was used here.

Other retrospective data suggest benefits of aggressive initial fluid resuscitation. For instance, a single-center prospective cohort evaluated the utility of the sepsis bundle when it is completed beyond the 6-hour period (18). Patients were divided as early or delayed compilers at 6 hours and compilers and non-compliers at 18 hours. This included meeting the MAP and/or lactate goal after a fluid challenge.

498 patients were evaluated, with those who compiled at 18hrs with the bundle having lower overall in-hospital mortality and 28-day mortality:
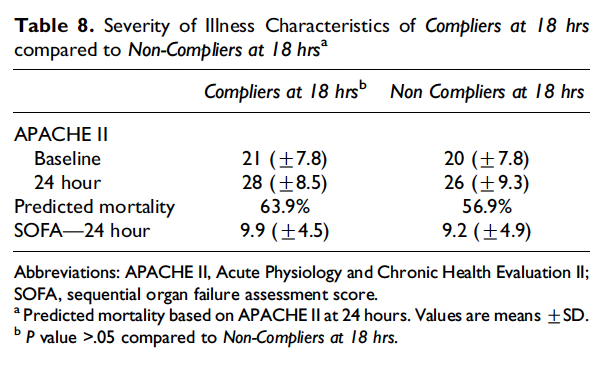
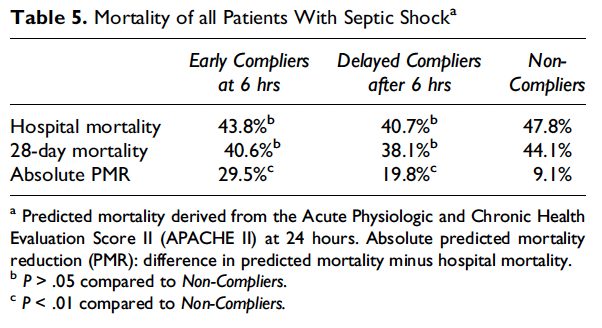
Notably, compilers had a significant higher fluid administration during the first 18 hours (7.7 vs 5.96L), and more patients achieved the goal MAP (100% vs 88%), however when looking at the compliance at 6 hours it appears that early compliance at 6 hours was associated with an absolute risk reduction, despite the fact that early compliance group had the highest APACHE II score (23 vs 20.4 in the delayed compliance vs 19 in the non-compliance group):
A historical cohort analysis evaluated the influence of IVF rate on mortality (19). 1052 patients were enrolled, and stratified amongst 4 groups. Time to shock reversal was faster in the cohort of patients who had IVF infusion of at least 25cc/kg/min:
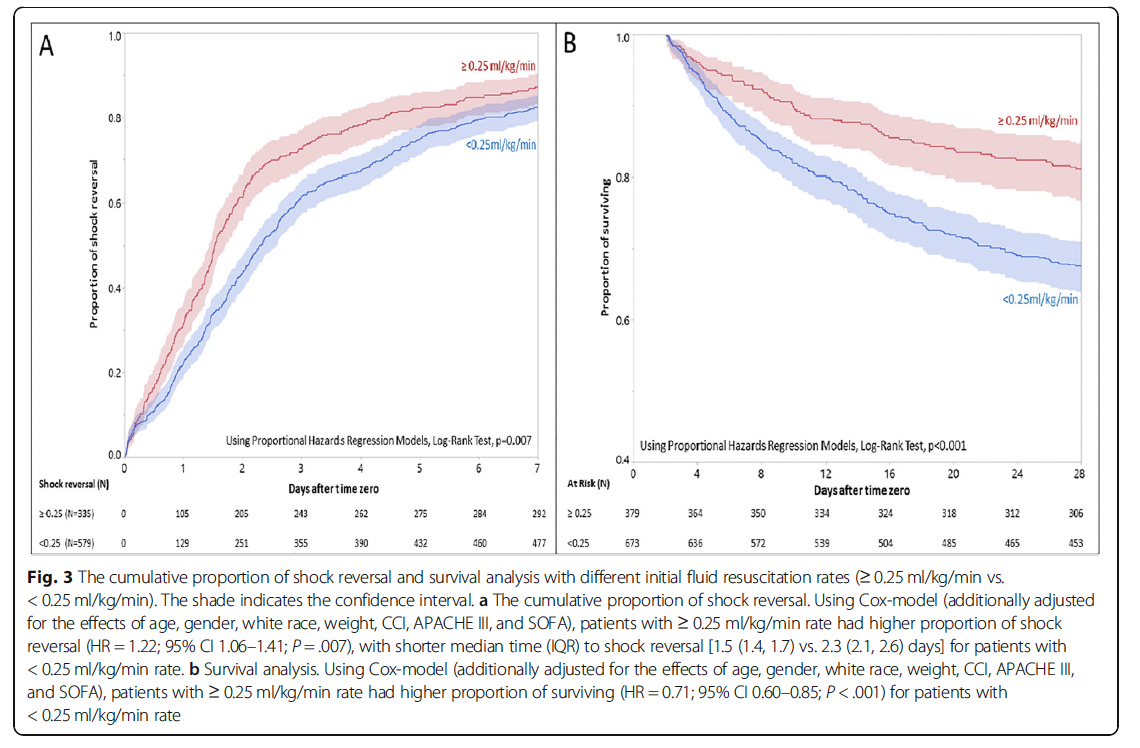
Not only that, but it appears that faster fluid boluses were associated with improved 28-day mortality though more patients in the <0.17cc/kg/min rate had pulmonary infection when compared to the > 0.5cc/kg/min (37% vs 47%). Despite this, however, it appears some retrospective data does not seem to support that initial fluid bolus. For instance, a retrospective study of 1027 patients with septic shock evaluated those patients who were compliant with the initial fluid bolus (20). After adjustment, compliance with the fluid metric was not associated with in-hospital mortality (OR 1.03, 95% CI 0.76-1.41). Similarly, among 49331 patients evaluated in another cohort (21), adherence to the 3 hour sepsis bundle was correlated with lower mortality, though this was driven mostly by timely administration of antibiotics:

Moreover, odds of in-hospital death among patients who had completed their fluid bolus within 12 hours was similar to those who had it within 6 hours (OR 1.02, 95% CI 0.92 to 1.14). The closets. The closes insight into this question comes from a single-center retrospective study of 367 patients, which found that standard fluid resuscitation was not associated with improved mortality in septic patients who had a DNI order placed (30):
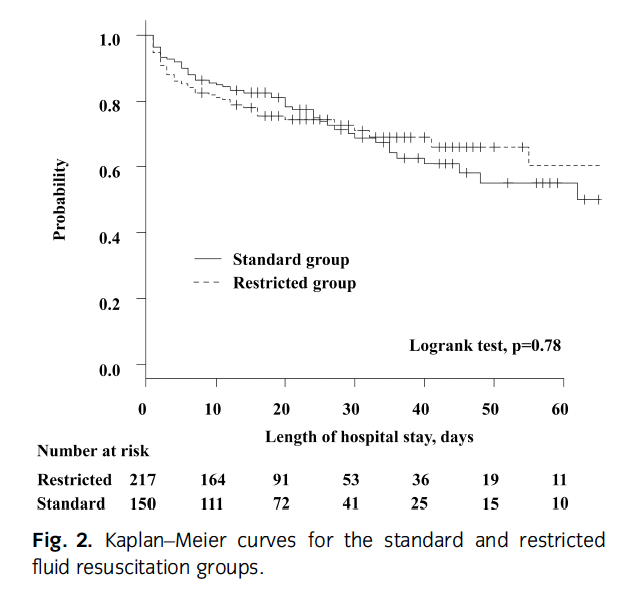
Notably, the median fluid in the restricted volume group was 15cc/kg compared to 48cc/kg in the standard group.
How much fluid is too much?
Given the influence of the initial Rivers trial, most of the data obtained on fluid resuscitation describes patients who have already received at least 30cc/kg of IVF prior to enrolling, and as a result we do not know if we could get away with giving less fluids and still have a therapeutic benefit. Based on the pathophysiology of sepsis, it would stand to reason that limited IVF and early pressors may be more physiologic than pure fluids. While the initial fluid resuscitation regimen is a matter of opinion, the harms of too much fluids in sepsis has been reported recently. Several retrospective cohorts have found a negative correlation with positive fluid balance and mortality. A retrospective cohort of 350 patients found that higher fluid balance was associated with higher mortality (22):


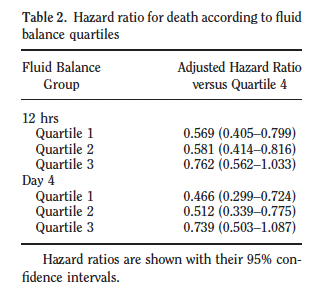
In a single-center prospective study of 173 patients (23), positive fluid balance was associated with higher risk of ICU mortality (HR 1.014, 95% CI 1.008-1.021 per ml/kg increase), which persisted after multivariate modeling (aHR 1.014, 95% CI 1.007-1.022). A data-set analysis of over 35,000 ICU patients found that high volume resuscitation during the first day of ICU stay was correlated with increased mortality the sicker the patient was i.e. someone with a high fluid resuscitation during the first day who had both shock and mechanical ventilation had an added 3.4% odds of death per additional liter of IV (24):

The observational SOAP study evaluated a total of 3147 critically ill patients in European ICUs, with multivariate logistic regression analysis finding that a positive fluid balance as associated with increased mortality (25):

The VASST study, a retrospective cohort that analyzed the impact of a positive fluid balance in the first 12 hours of resuscitation found that mortality was correlated with higher positive fluid balance (26):
Moreover, it appears that CVP measurement were also associated with increased mortality during the first 12 hours but the relationship was not significant at 4 days:

Interestingly, a CVP <8 was correlated with mortality if their net fluid balance was positive:

A cohort study of 405 patients found that volume overload at day 1 and day 3 after EGDT was associated with higher rate of interventions such as thoracentesis and diuretic use as well as increased rate of in-hospital mortality (27):

Slowing Down Fluids after initial resuscitation:
Given we do not know the ideal volume of initial resuscitation, what about the aftermath. Can we do with less fluids once septic patients are admitted? Perhaps. A randomized trial of 104 patients with sepsis evaluated a restricted fluid strategy (28). Here, a 1L bolus was given to the standard care group followed by 500cc boluses given as needed to maintain a MAP of 65, compared to the restricted fluid where vasopressors were initiated to maintain the MAP goal. While both groups received a substantial amount of fluids prior to randomization, the total volume was significantly lower in the restricted volume group:

Mortality was not statistically different between both groups:

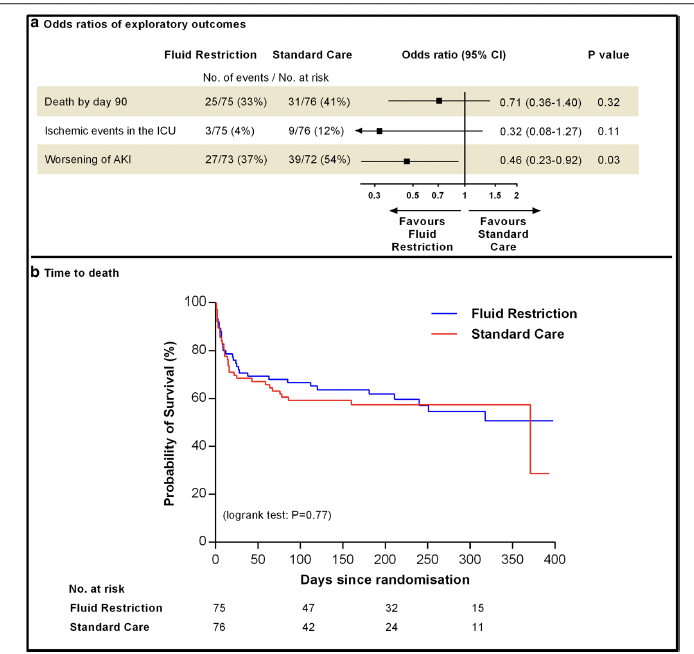
The CLASSIC trial, which was a multicenter, parallel-group trial evaluated a fluid restricted strategy during the ICU stay (29). Those in the restricted group were given IVF boluses of 250-500cc. 153 patients were enrolled, with both groups being fairly comparable, though more patients in the restriction group had AKI (51% vs 38%),and both groups had at least 4L of IVF given prior to randomization. Patients in the standard of care group had more fluids given when compared to the restriction group (difference -1407, 95% CI -2358 to -456), however exploratory secondary outcomes did not show a difference in mortality:
TL;DR
- Sepsis and septic shock is more than just “hypovolemia”
- Vasoplegia, decreased cardiac function, and increased vascular permeability are also key factors in the pathophysiology of sepsis
- The mandate of 30cc/kg initial bolus is based on little data, meaning the benefit of that initial bolus is difficult to ascertain though retrospective data suggests that the initial resuscitation is not just about an absolute fluid volume goal
- There is a mortality increase with a net positive fluid balance
References:
- Macdonald S, Peake SL, Corfield AR, Delaney A. Fluids or vasopressors for the initial resuscitation of septic shock. Front Med (Lausanne). 2022 Nov 24;9:1069782. doi: 10.3389/fmed.2022.1069782. PMID: 36507525; PMCID: PMC9729725.
- Feihl F, Broccard AF. Interactions between respiration and systemic hemodynamics. Part I: basic concepts. Intensive Care Med. 2009 Jan;35(1):45-54. doi: 10.1007/s00134-008-1297-z. Epub 2008 Sep 30. PMID: 1882536
- Landesberg G, Gilon D, Meroz Y, Georgieva M, Levin PD, Goodman S, Avidan A, Beeri R, Weissman C, Jaffe AS, Sprung CL. Diastolic dysfunction and mortality in severe sepsis and septic shock. Eur Heart J. 2012 Apr;33(7):895-903. doi: 10.1093/eurheartj/ehr351. Epub 2011 Sep 11. PMID: 21911341; PMCID: PMC3345552.
- Ognibene FP, Parker MM, Natanson C, Shelhamer JH, Parrillo JE. Depressed left ventricular performance. Response to volume infusion in patients with sepsis and septic shock. Chest. 1988 May;93(5):903-10. doi: 10.1378/chest.93.5.903. PMID: 3359845.
- Monge García MI, Guijo González P, Gracia Romero M, Gil Cano A, Oscier C, Rhodes A, Grounds RM, Cecconi M. Effects of fluid administration on arterial load in septic shock patients. Intensive Care Med. 2015 Jul;41(7):1247-55. doi: 10.1007/s00134-015-3898-7. Epub 2015 Jun 11. PMID: 26077088.
- Sánchez M, Jiménez-Lendínez M, Cidoncha M, Asensio MJ, Herrerot E, Collado A, Santacruz M. Comparison of fluid compartments and fluid responsiveness in septic and non-septic patients. Anaesth Intensive Care. 2011 Nov;39(6):1022-9. doi: 10.1177/0310057X1103900607. PMID: 22165353.
- Aya HD, Ster IC, Fletcher N, Grounds RM, Rhodes A, Cecconi M. Pharmacodynamic Analysis of a Fluid Challenge. Crit Care Med. 2016 May;44(5):880-91. doi: 10.1097/CCM.0000000000001517. PMID: 26683506.
- Glassford NJ, Eastwood GM, Bellomo R. Physiological changes after fluid bolus therapy in sepsis: a systematic review of contemporary data. Crit Care. 2014 Dec 27;18(6):696. doi: 10.1186/s13054-014-0696-5. PMID: 25673138; PMCID: PMC4331149.
- Aya HD, Rhodes A, Chis Ster I, Fletcher N, Grounds RM, Cecconi M. Hemodynamic Effect of Different Doses of Fluids for a Fluid Challenge: A Quasi-Randomized Controlled Study. Crit Care Med. 2017 Feb;45(2):e161-e168. doi: 10.1097/CCM.0000000000002067. PMID: 27655325.
- Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C, Machado FR, Mcintyre L, Ostermann M, Prescott HC, Schorr C, Simpson S, Wiersinga WJ, Alshamsi F, Angus DC, Arabi Y, Azevedo L, Beale R, Beilman G, Belley-Cote E, Burry L, Cecconi M, Centofanti J, Coz Yataco A, De Waele J, Dellinger RP, Doi K, Du B, Estenssoro E, Ferrer R, Gomersall C, Hodgson C, Hylander Møller M, Iwashyna T, Jacob S, Kleinpell R, Klompas M, Koh Y, Kumar A, Kwizera A, Lobo S, Masur H, McGloughlin S, Mehta S, Mehta Y, Mer M, Nunnally M, Oczkowski S, Osborn T, Papathanassoglou E, Perner A, Puskarich M, Roberts J, Schweickert W, Seckel M, Sevransky J, Sprung CL, Welte T, Zimmerman J, Levy M. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit Care Med. 2021 Nov 1;49(11):e1063-e1143. doi: 10.1097/CCM.0000000000005337. PMID: 34605781.
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally ME, Rochwerg B, Rubenfeld GD, Angus DC, Annane D, Beale RJ, Bellinghan GJ, Bernard GR, Chiche JD, Coopersmith C, De Backer DP, French CJ, Fujishima S, Gerlach H, Hidalgo JL, Hollenberg SM, Jones AE, Karnad DR, Kleinpell RM, Koh Y, Lisboa TC, Machado FR, Marini JJ, Marshall JC, Mazuski JE, McIntyre LA, McLean AS, Mehta S, Moreno RP, Myburgh J, Navalesi P, Nishida O, Osborn TM, Perner A, Plunkett CM, Ranieri M, Schorr CA, Seckel MA, Seymour CW, Shieh L, Shukri KA, Simpson SQ, Singer M, Thompson BT, Townsend SR, Van der Poll T, Vincent JL, Wiersinga WJ, Zimmerman JL, Dellinger RP. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017 Mar;43(3):304-377. doi: 10.1007/s00134-017-4683-6. Epub 2017 Jan 18. PMID: 28101605.
- Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, Peterson E, Tomlanovich M; Early Goal-Directed Therapy Collaborative Group. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001 Nov 8;345(19):1368-77. doi: 10.1056/NEJMoa010307. PMID: 11794169.
- ProCESS Investigators; Yealy DM, Kellum JA, Huang DT, Barnato AE, Weissfeld LA, Pike F, Terndrup T, Wang HE, Hou PC, LoVecchio F, Filbin MR, Shapiro NI, Angus DC. A randomized trial of protocol-based care for early septic shock. N Engl J Med. 2014 May 1;370(18):1683-93. doi: 10.1056/NEJMoa1401602. Epub 2014 Mar 18. PMID: 24635773; PMCID: PMC4101700.
- ARISE Investigators; ANZICS Clinical Trials Group; Peake SL, Delaney A, Bailey M, Bellomo R, Cameron PA, Cooper DJ, Higgins AM, Holdgate A, Howe BD, Webb SA, Williams P. Goal-directed resuscitation for patients with early septic shock. N Engl J Med. 2014 Oct 16;371(16):1496-506. doi: 10.1056/NEJMoa1404380. Epub 2014 Oct 1. PMID: 25272316.
- Mouncey PR, Osborn TM, Power GS, Harrison DA, Sadique MZ, Grieve RD, Jahan R, Harvey SE, Bell D, Bion JF, Coats TJ, Singer M, Young JD, Rowan KM; ProMISe Trial Investigators. Trial of early, goal-directed resuscitation for septic shock. N Engl J Med. 2015 Apr 2;372(14):1301-11. doi: 10.1056/NEJMoa1500896. Epub 2015 Mar 17. PMID: 25776532.
- PRISM Investigators; Rowan KM, Angus DC, Bailey M, Barnato AE, Bellomo R, Canter RR, Coats TJ, Delaney A, Gimbel E, Grieve RD, Harrison DA, Higgins AM, Howe B, Huang DT, Kellum JA, Mouncey PR, Music E, Peake SL, Pike F, Reade MC, Sadique MZ, Singer M, Yealy DM. Early, Goal-Directed Therapy for Septic Shock – A Patient-Level Meta-Analysis. N Engl J Med. 2017 Jun 8;376(23):2223-2234. doi: 10.1056/NEJMoa1701380. Epub 2017 Mar 21. PMID: 28320242.
- Andrews B, Semler MW, Muchemwa L, Kelly P, Lakhi S, Heimburger DC, Mabula C, Bwalya M, Bernard GR. Effect of an Early Resuscitation Protocol on In-hospital Mortality Among Adults With Sepsis and Hypotension: A Randomized Clinical Trial. JAMA. 2017 Oct 3;318(13):1233-1240. doi: 10.1001/jama.2017.10913. PMID: 28973227; PMCID: PMC5710318.
- Coba V, Whitmill M, Mooney R, Horst HM, Brandt MM, Digiovine B, Mlynarek M, McLellan B, Boleski G, Yang J, Conway W, Jordan J; (The Henry Ford Hospital Sepsis Collaborative Group). Resuscitation bundle compliance in severe sepsis and septic shock: improves survival, is better late than never. J Intensive Care Med. 2011 Sep-Oct;26(5):304-13. doi: 10.1177/0885066610392499. Epub 2011 Jan 10. PMID: 21220270.
- Hu B, Chen JCY, Dong Y, Frank RD, Passe M, Portner E, Peng Z, Kashani K. Effect of initial infusion rates of fluid resuscitation on outcomes in patients with septic shock: a historical cohort study. Crit Care. 2020 Apr 7;24(1):137. doi: 10.1186/s13054-020-2819-5. PMID: 32264936; PMCID: PMC7140334.
- Truong TN, Dunn AS, McCardle K, Glasser A, Huprikar S, Poor H, Raucher B, Poeran J. Adherence to fluid resuscitation guidelines and outcomes in patients with septic shock: Reassessing the “one-size-fits-all” approach. J Crit Care. 2019 Jun;51:94-98. doi: 10.1016/j.jcrc.2019.02.006. Epub 2019 Feb 5. PMID: 30784983.
- Seymour CW, Gesten F, Prescott HC, Friedrich ME, Iwashyna TJ, Phillips GS, Lemeshow S, Osborn T, Terry KM, Levy MM. Time to Treatment and Mortality during Mandated Emergency Care for Sepsis. N Engl J Med. 2017 Jun 8;376(23):2235-2244. doi: 10.1056/NEJMoa1703058. Epub 2017 May 21. PMID: 28528569; PMCID: PMC5538258.
- Sadaka F, Juarez M, Naydenov S, O’Brien J. Fluid resuscitation in septic shock: the effect of increasing fluid balance on mortality. J Intensive Care Med. 2014 Jul-Aug;29(4):213-7. doi: 10.1177/0885066613478899. Epub 2013 Feb 27. PMID: 23753235.
- Acheampong A, Vincent JL. A positive fluid balance is an independent prognostic factor in patients with sepsis. Crit Care. 2015 Jun 15;19(1):251. doi: 10.1186/s13054-015-0970-1. PMID: 26073560; PMCID: PMC4479078.
- Marik PE, Linde-Zwirble WT, Bittner EA, Sahatjian J, Hansell D. Fluid administration in severe sepsis and septic shock, patterns and outcomes: an analysis of a large national database. Intensive Care Med. 2017 May;43(5):625-632. doi: 10.1007/s00134-016-4675-y. Epub 2017 Jan 27. PMID: 28130687.
- Vincent JL, Sakr Y, Sprung CL, Ranieri VM, Reinhart K, Gerlach H, Moreno R, Carlet J, Le Gall JR, Payen D; Sepsis Occurrence in Acutely Ill Patients Investigators. Sepsis in European intensive care units: results of the SOAP study. Crit Care Med. 2006 Feb;34(2):344-53. doi: 10.1097/01.ccm.0000194725.48928.3a. PMID: 16424713.
- Boyd JH, Forbes J, Nakada TA, Walley KR, Russell JA. Fluid resuscitation in septic shock: a positive fluid balance and elevated central venous pressure are associated with increased mortality. Crit Care Med. 2011 Feb;39(2):259-65. doi: 10.1097/CCM.0b013e3181feeb15. PMID: 20975548.
- Kelm DJ, Perrin JT, Cartin-Ceba R, Gajic O, Schenck L, Kennedy CC. Fluid overload in patients with severe sepsis and septic shock treated with early goal-directed therapy is associated with increased acute need for fluid-related medical interventions and hospital death. Shock. 2015 Jan;43(1):68-73. doi: 10.1097/SHK.0000000000000268. PMID: 25247784; PMCID: PMC4269557.
- Macdonald SPJ, Keijzers G, Taylor DM, Kinnear F, Arendts G, Fatovich DM, Bellomo R, McCutcheon D, Fraser JF, Ascencio-Lane JC, Burrows S, Litton E, Harley A, Anstey M, Mukherjee A; REFRESH trial investigators. Restricted fluid resuscitation in suspected sepsis associated hypotension (REFRESH): a pilot randomised controlled trial. Intensive Care Med. 2018 Dec;44(12):2070-2078. doi: 10.1007/s00134-018-5433-0. Epub 2018 Oct 31. PMID: 30382308.
- Hjortrup PB, Haase N, Bundgaard H, Thomsen SL, Winding R, Pettilä V, Aaen A, Lodahl D, Berthelsen RE, Christensen H, Madsen MB, Winkel P, Wetterslev J, Perner A; CLASSIC Trial Group; Scandinavian Critical Care Trials Group. Restricting volumes of resuscitation fluid in adults with septic shock after initial management: the CLASSIC randomised, parallel-group, multicentre feasibility trial. Intensive Care Med. 2016 Nov;42(11):1695-1705. doi: 10.1007/s00134-016-4500-7. Epub 2016 Sep 30. PMID: 27686349.
- Matsuda W, Funato Y, Miyazaki M, Tomiyama K. Fluid resuscitation of at least 30 mL/kg was not associated with decreased mortality in patients with infection, signs of hypoperfusion, and a do-not-intubate order. Acute Med Surg. 2022 Sep 30;9(1):e795. doi: 10.1002/ams2.795. PMID: 36203853; PMCID: PMC9525617.
