I’ve previously discussed how much more difficult Enterococcal infections are to treat when compared to other bacteria such as streptococci. This stems from the fact these bacteria have tend to be more resistant to beta-lactam antibiotics, with synergy being the name of the game for serious infections with these bacteria (in general, ampicillin/ceftriaxone). This is due to the fact their PBPs have lower affinity to beta lactams.
The study of vancomycin resistance is actually out of the scope of this post (read: most of the basic science that goes into their study went over my head). As a result, I will summarize it as briefly as I can and just hit the high points. Prior to this, let’s discuss the mechanism of action of vancomycin/teicoplatin. These affect the late stages of cell-wall production by binding to a peptidoglycan precursor at a D-ala-D-ala residues, leading to stunted cell-wall production (1, 2):
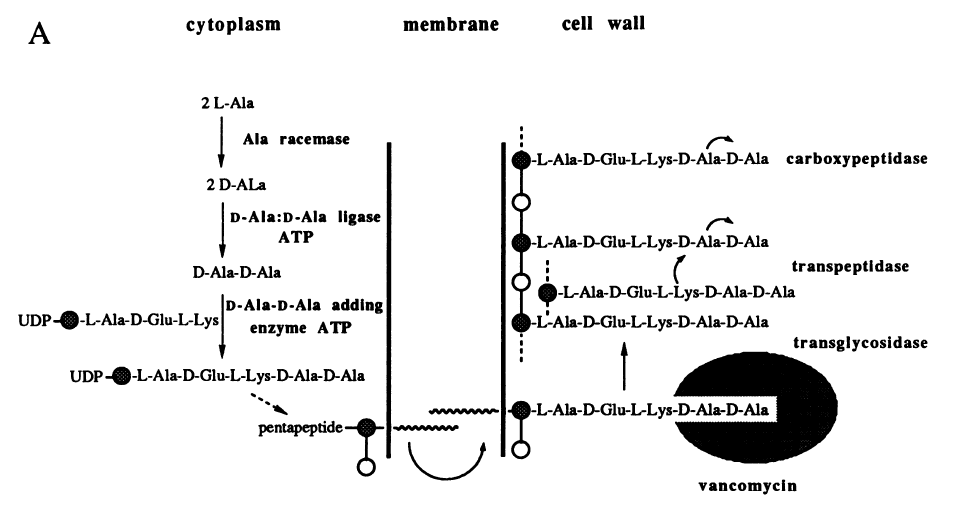
Because of this, the endpoint of any mutation going forward is to change the substrate of the D-ala-D-ala binding site. This is done by the following:
- The presence of a glycopeptide (let’s say vancomycin) is sense by the cell machinery.
- This activates a series of genes which sole purpose is to change that D-ala-D-ala binding site into something else and to ensure that D-ala-D-ala is not made
- Vancomycin and teicoplatin can activate one set of genes (vanA) while teicoplatin cannot activate another set of genes that can be activated by vancomycin (vanB).
Now, a bit more detail. The saying there is a presence of vanA or vanB gene is actually a bit misleading, since they represent a series of genes that work in concert to ensure resistance to vancomycin. To use one of the most studied examples, let’s look at vanA (3,4). This includes a series of genes, including the main regulators (vanS and vanR), which are the ones that dictate resistance, the dispeptide genes (aka the ones that change the required D-ala-D-ala signature, vanA, vanH, and vanX) and others (vanY and vanZ). These all work in concert:

- vanA and vanH produce dipeptides that are different from D-ala-D-ala more efficiently (usually D-ala-D-Lac).
- vanX and vanY cleave any D-ala-D-ala that manages to get away.
Here is a summary of the overall resistance profiles (3):

You’ll notice that vanB (which works the same way as vanA) remains susceptible to teicoplatin. As I mentioned previously, teicoplatin does not induce vanB genes, so there is no resistance here. If you see VAN resistance but not teicoplatin, then you’re dealing with a vanB phenotype.
Pharmacodynamics/Pharmacokinetics of Daptomycin and Linezolid
Yes, another bit before actually diving into the clinical data. If you need a refresher on some of the pharmacology basics, click here. If you need one on bacteristatic vs bactericidal, then click here. This will make sense as we explore the rationale behind daptomycin dosage and why, as we move forward, you may start considering using higher doses rather than standard 6mg/kg, at least for enterococci. In general, linezolid tends to be more of a bactericidal antibiotic while daptomycin is a bactericidal antibiotic. To bring everyone to speed, daptomycin induces changes into the cell wall that causes bacteria to lose ions (similar to amphotericin) while linezolid/tedizolid bind to the 30s ribosomal subunit. Data supports these pharmacodynamic models. For instance, a study of 8 VRE strains, linezolid displayed a bacteriostatic pharmacokinetic effect against all these strains (defined as a reduction in <1.5log10 CFU/g), with higher doses (higher than 16mg/kg) displaying more effective killing (5):

In a simulated model of VRE endocardial vegetations (6), daptomycin at any dose displayed a more “bactericidal” profile when compared to linezolid (drop in 3 log10 CFU/g):

Further, in this pharmacodynamic model, the AUC was significantly higher for all daptomycin doses, with bactericidal activity being longer in the daptomycin 10mg/kg up to 96hr:

Furthermore, it seems the pharmacodynamic value to look at is AUC/MIC as a marker of efficacy. For instance, a neutropenic model using mice thighs (7) evaluated daptomycin pharmacodynamics and found that peak over MIC and AUC/MIC were best correlated with in vitro efficacy:

While there is more data that I can comb over, I think i’ll leave it at that. Suffice to say, with serious infections, seems that daptomycin, especially at higher doses may be the way to go.
Clinical Data:
Most data here tends to be cohort, usually retrospective, though many studies attempt to control for confounding with propensity score matching. Given this, take the following summary with a pillar of salt substitute. Some data on linezolid come from a non-matched compassionate use retrospective study (without any matching, 8). Linezolid achieved an 81.4% overall cure rate in VRE related infections, with VRE-BSI achieving a cure rate of 78% vs 63% for MRSA. Another study of solid organ transplant patients (again, with compassionate use linezolid) found a 63% cure rate of VRE. Keep in mind this is without a good comparator, but given these resistant enterococci, it is looking fairly good. So how does it fare for our friend/buddy/dude, daptomycin?
A multicenter retrospective study from the VA (10) compared 644 patients treated with daptomycin and linezolid for VRE-related bacteremia. Daptomycin was associated with better outcomes at 7 days and 30 days when compared to linezolid:

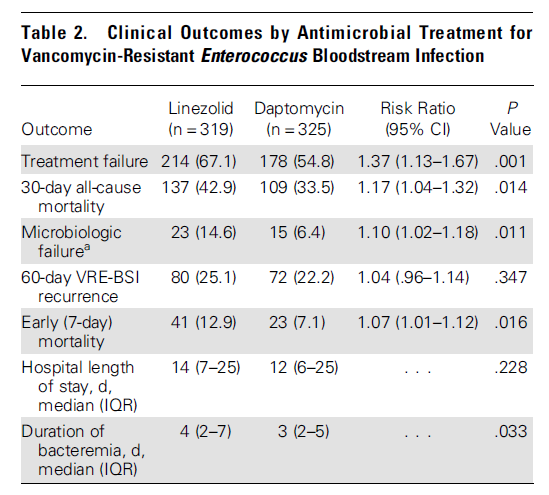
This held true even after propensity score matching:

Notably, in this study the median dose of daptomycin was a bit below 6mg/kg. Another retrospective study (11) of 101 patients did not find a statistical significant difference between treatments, though a trend was found towards linezolid (daptomycin, 46.3% vs linezolid 29.4%; P = NS). Two meta-analyses found that linezolid was associated with improved mortality In a meta-analysis of 9 studies (12) found a trend towards linezolid being favorable for enterococcal bacteremia, though it did not reach statistical significance.


Notably, primary outcomes ranged from 30 day mortality to 14 day mortality, to all cause mortality, though there was relatively low level of heterogeneity found in these studies. Furthermore, the daptomycin dose ranged from 3.4mg/kg to 10.4mg/kg. Another meta-analysis of 13 studies (13) found that daptomycin was associated with higher mortality in VRE-bacteremia patients, which held true in adjusted OR as well:

Though there is no mention of the average doses of daptomycin of the meta-analysis, the doses ranged from 3.4-10 in one study, with 4 not reporting any doses. It is difficult to make out this data. For instance one multicenter prospective study of 212 patients with VRE infections evaluated different doses of daptomycin vs linezolid at 600mg q12h (14). 71 got linezolid while 141 got daptomycin. Univariate analysis found that daptomycin use was associated with higher all-cause 14 day mortality compared to linezolid (aOR 0.45, 95% CI 0.21-0.96), further linezolid also was associated with lower infection-related mortality compared to daptomycin.

Notably, higher dose daptomycin per 1mg/kg above 6mg/kg was associated with lower all cause 14d mortality (OR 0.76, 95% CI 0.59-0.98), with both linezolid (OR 0.38, 95% CI 0.19-0.76) and daptomycin >9mg/kg (OR 0.44, 95% CI 0.18-1.07) when compared to lower daptomycin dose (6-9mg/kg) in univariate analysis. This also held true in multivariate analysis, with higher daptomycin dose having no advantage over linezolid (aOR 1.40, 95% CI 0.45-4.37). This seems to suggest that, at least at doses greater than the approved 6mg/kg, at least daptomycin is comparable to linezolid, though data is not abundant for higher doses of daptomycin vs linezolid.
Indeed, most of the studies I found compared daptomycin doses with themselves. For instance, a retrospective study evaluated 112 patients with VRE bacteremia and found that patients who were treated with high doses of daptomycin (>9mg/kg) had lower mortality when compared to those treated with 6-9mg/kg (13.6% vs 30.7%, p-value 0.11, 15). In multivariate logistic regression analysis, higher doses were associated with lower 14 day mortality:

Furthermore, there was no difference in patient mortality with daptomycin MIC = 4mg/L compared to MIC <2mg/L (aOR 0.55, 95% CI 0.001-268). Higher daptomycin doses were associated with lower mortality, regardless of daptomycin MIC:

Notably, there were no differences between group in elevated CK. The largest multicenter retrospective study evaluated 3 different dose ranges of daptomycin in 911 cases of VRE bacteremia (16). The vast majority were treated with a standard dose of 6mg/kg (77.8%). Higher doses were used in the latter parts of the study, and usually doses ~10mg/kg were combined with aminoglycosides. High doses were associated with improved mortality at 30 days:

With both medium and high doses being associated with similar microbiological cure rates:

Subgroup analysis in this study also favored higher doses (10mg/kg vs 6-8mg/kg):

Here, no patients in the high dose had CK elevation (0/51) compared to standard dose (6/441) or medium dose group (1/103).
What to make of these data? It is difficult to make out the meta-analyses, as these use different doses of daptomycin, but seems that daptomycin doses that are above 6mg/kg (at least 8mg/kg) tend to be effective. Given the severity of some of the side effects of linezolid (bone marrow suppression, peripheral neuropathy, serotonin syndrome) and the fact that daptomycin tends to be bactericidal, my preference is to give daptomycin at least 8mg/kg or even higher if someone is able to tolerate it (read: elevated CK). Especially since the side-effect profile is more favorable here (read: linezolid = repeat of the Libby Zion case).
Dual Therapy
Similar to dual therapy with CTX-AMP, people have been trying to exploit synergy here. Unfortunately, most of the “data” is based on case reports, so take this as a grain of salt-substitute (i.e. you can probably do this on a case-by-case basis, but know there is no data guiding you here). Though, there is some animal/basic science data to back up some of the decisions. For instance, in one model of VRE, the combination of daptomycin and gentamicin achieved better killing than either antibiotic alone (17):

This also held true in another model for ampicillin and daptomycin (18):

More robust data comes from a prospective cohort study that evaluated 309 patients with VRE-bacteremia who got either daptomycin alone compared with daptomycin-beta lactam combination (19). In a multivariate cox proportional model, daptomycin dose >9mg/kg with beta-lactam was associated with improved survival:

This held true in a time-dependent Cox regression outcome to control immortal time bias:

Other combinations have been tried, but as mentioned previously, this is limited to case reports. For instance, VRE endocarditis has been treated with a combination of daptomycin/tigecycline (20) and linezolid/daptomycin (21). In another instance, a neutropenic patient with VRE bacteremia was treated with a combination of ampicillin/quinupristin-dalfopristin (22) and another patient with VRE endocarditis and DDKT was treated with the same combination (23). A case report (24) found that combination therapy was more efficacious in vitro, with synercid combinations having a more significant drop in CFU than single therapies in vitro:

The “New Toys”
Out of the scope of this this post, but will be on an MRSA post coming whenever I get to it. Further, I will not go into detail about these, but i’ll cite some data. In general, there are a few:
- Tigecycline (Sagat’s favorite drug) – a derivative of minocycline, it has some in vitro activity with VRE (25, 26).
- Orativancin – the once-weekly infusion. One complicated case with multiple recurrences achieved clearance following therapy with orativancin (27).
- “Synercid” or syner-sick – why do I call it this? My experience with using this has not been very positive.
- Telavancin/Dalvabancin – some in vitro data suggest activity against VRE (28)
If you find yourself using these drugs, either your patient failed multiple therapies and you need to look for that vegetation, or we are in a post-antibiotic era where these are the new “vancomycin”, with the exception of probably tedizolid.
TL;DR
- Daptomycin and linezolid are both reasonable options for VRE.
- Daptomycin at higher doses (usually 8mg/kg) has equal efficacy as linezolid
- Despite higher doses, CK elevation does not seem to be an issue
- Dual therapy for severe infections has been tried, with some clinical suggesting that beta-lactam/daptomycin is better than daptomycin alone. Some case reports suggest favorable outcomes with other combinations
References:
- Patel S, Preuss CV, Bernice F. Vancomycin. [Updated 2020 Sep 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459263/
- [edited by] John E. Bennett, Raphael Dolin, Martin J. Blaser. (2015). Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. Philadelphia, PA :Elsevier/Saunders,
- Arthur M, Courvalin P. Genetics and mechanisms of glycopeptide resistance in enterococci. Antimicrob Agents Chemother. 1993 Aug;37(8):1563-71. doi: 10.1128/aac.37.8.1563. PMID: 8215264; PMCID: PMC188020.
- Reynolds PE, Depardieu F, Dutka-Malen S, Arthur M, Courvalin P. Glycopeptide resistance mediated by enterococcal transposon Tn1546 requires production of VanX for hydrolysis of D-alanyl-D-alanine. Mol Microbiol. 1994 Sep;13(6):1065-70. doi: 10.1111/j.1365-2958.1994.tb00497.x. PMID: 7854121.
- Tsuji BT, Bulitta JB, Brown T, Forrest A, Kelchlin PA, Holden PN, Peloquin CA, Skerlos L, Hanna D. Pharmacodynamics of early, high-dose linezolid against vancomycin-resistant enterococci with elevated MICs and pre-existing genetic mutations. J Antimicrob Chemother. 2012 Sep;67(9):2182-90. doi: 10.1093/jac/dks201. Epub 2012 Jun 8. PMID: 22685161.
- Hall AD, Steed ME, Arias CA, Murray BE, Rybak MJ. Evaluation of standard- and high-dose daptomycin versus linezolid against vancomycin-resistant Enterococcus isolates in an in vitro pharmacokinetic/pharmacodynamic model with simulated endocardial vegetations. Antimicrob Agents Chemother. 2012 Jun;56(6):3174-80. doi: 10.1128/AAC.06439-11. Epub 2012 Apr 2. PMID: 22470111; PMCID: PMC3370794.
- Safdar N, Andes D, Craig WA. In vivo pharmacodynamic activity of daptomycin. Antimicrob Agents Chemother. 2004 Jan;48(1):63-8. doi: 10.1128/aac.48.1.63-68.2004. PMID: 14693519; PMCID: PMC310158.
- Birmingham MC, Rayner CR, Meagher AK, Flavin SM, Batts DH, Schentag JJ. Linezolid for the treatment of multidrug-resistant, gram-positive infections: experience from a compassionate-use program. Clin Infect Dis. 2003 Jan 15;36(2):159-68. doi: 10.1086/345744. Epub 2003 Jan 3. PMID: 12522747.
- El-Khoury J, Fishman JA. Linezolid in the treatment of vancomycin-resistant Enterococcus faecium in solid organ transplant recipients: report of a multicenter compassionate-use trial. Transpl Infect Dis. 2003 Sep;5(3):121-5. doi: 10.1034/j.1399-3062.2003.00024.x. PMID: 14617299.
- Britt NS, Potter EM, Patel N, Steed ME. Comparison of the Effectiveness and Safety of Linezolid and Daptomycin in Vancomycin-Resistant Enterococcal Bloodstream Infection: A National Cohort Study of Veterans Affairs Patients. Clin Infect Dis. 2015 Sep 15;61(6):871-8. doi: 10.1093/cid/civ444. Epub 2015 Jun 10. PMID: 26063715; PMCID: PMC4551009.
- Crank CW, Scheetz MH, Brielmaier B, Rose WE, Patel GP, Ritchie DJ, Segreti J. Comparison of outcomes from daptomycin or linezolid treatment for vancomycin-resistant enterococcal bloodstream infection: A retrospective, multicenter, cohort study. Clin Ther. 2010 Sep;32(10):1713-9. doi: 10.1016/j.clinthera.2010.09.008. PMID: 21194593.
- Whang DW, Miller LG, Partain NM, McKinnell JA. Systematic review and meta-analysis of linezolid and daptomycin for treatment of vancomycin-resistant enterococcal bloodstream infections. Antimicrob Agents Chemother. 2013 Oct;57(10):5013-8. doi: 10.1128/AAC.00714-13. Epub 2013 Jul 29. PMID: 23896468; PMCID: PMC3811395.
- Chuang YC, Wang JT, Lin HY, Chang SC. Daptomycin versus linezolid for treatment of vancomycin-resistant enterococcal bacteremia: systematic review and meta-analysis. BMC Infect Dis. 2014 Dec 13;14:687. doi: 10.1186/s12879-014-0687-9. PMID: 25495779; PMCID: PMC4269951.
- Chuang YC, Lin HY, Chen PY, Lin CY, Wang JT, Chang SC. Daptomycin versus linezolid for the treatment of vancomycin-resistant enterococcal bacteraemia: implications of daptomycin dose. Clin Microbiol Infect. 2016 Oct;22(10):890.e1-890.e7. doi: 10.1016/j.cmi.2016.07.018. Epub 2016 Jul 27. PMID: 27475738.
- Chuang YC, Lin HY, Chen PY, Lin CY, Wang JT, Chen YC, Chang SC. Effect of Daptomycin Dose on the Outcome of Vancomycin-Resistant, Daptomycin-Susceptible Enterococcus faecium Bacteremia. Clin Infect Dis. 2017 Apr 15;64(8):1026-1034. doi: 10.1093/cid/cix024. PMID: 28329222.
- Britt NS, Potter EM, Patel N, Steed ME. Comparative Effectiveness and Safety of Standard-, Medium-, and High-Dose Daptomycin Strategies for the Treatment of Vancomycin-Resistant Enterococcal Bacteremia Among Veterans Affairs Patients. Clin Infect Dis. 2017 Mar 1;64(5):605-613. doi: 10.1093/cid/ciw815. PMID: 28011602.
- Caron F, Kitzis MD, Gutmann L, Cremieux AC, Maziere B, Vallois JM, Saleh-Mghir A, Lemeland JF, Carbon C. Daptomycin or teicoplanin in combination with gentamicin for treatment of experimental endocarditis due to a highly glycopeptide-resistant isolate of Enterococcus faecium. Antimicrob Agents Chemother. 1992 Dec;36(12):2611-6. doi: 10.1128/aac.36.12.2611. PMID: 1336339; PMCID: PMC245515.
- Sakoulas G, Bayer AS, Pogliano J, Tsuji BT, Yang SJ, Mishra NN, Nizet V, Yeaman MR, Moise PA. Ampicillin enhances daptomycin- and cationic host defense peptide-mediated killing of ampicillin- and vancomycin-resistant Enterococcus faecium. Antimicrob Agents Chemother. 2012 Feb;56(2):838-44. doi: 10.1128/AAC.05551-11. Epub 2011 Nov 28. PMID: 22123698; PMCID: PMC3264218.
- Chuang YC, Chen PY, Lin CY, Chen YC, Wang JT, Chang SC. A retrospective clinical comparison of daptomycin vs daptomycin and a beta-lactam antibiotic for treating vancomycin-resistant Enterococcus faecium bloodstream infections. Sci Rep. 2018 Jan 26;8(1):1632. doi: 10.1038/s41598-018-19986-8. PMID: 29374204; PMCID: PMC5786011.
- Schutt AC, Bohm NM. Multidrug-resistant Enterococcus faecium endocarditis treated with combination tigecycline and high-dose daptomycin. Ann Pharmacother. 2009 Dec;43(12):2108-12. doi: 10.1345/aph.1M324. Epub 2009 Nov 3. PMID: 19887592.
- Jenkins I. Linezolid- and vancomycin-resistant Enterococcus faecium endocarditis: successful treatment with tigecycline and daptomycin. J Hosp Med. 2007 Sep;2(5):343-4. doi: 10.1002/jhm.236. PMID: 17935250.
- Bethea JA, Walko CM, Targos PA. Treatment of vancomycin-resistant enterococcus with quinupristin/dalfopristin and high-dose ampicillin. Ann Pharmacother. 2004 Jun;38(6):989-91. doi: 10.1345/aph.1D377. Epub 2004 Apr 20. PMID: 15100393.
- Thompson RL, Lavin B, Talbot GH. Endocarditis due to vancomycin-resistant Enterococcus faecium in an immunocompromised patient: cure by administering combination therapy with quinupristin/dalfopristin and high-dose ampicillin. South Med J. 2003 Aug;96(8):818-20. doi: 10.1097/01.SMJ.0000047962.61701.57. PMID: 14515928
- Matsumura S, Simor AE. Treatment of endocarditis due to vancomycin-resistant Enterococcus faecium with quinupristin/dalfopristin, doxycycline, and rifampin: a synergistic drug combination. Clin Infect Dis. 1998 Dec;27(6):1554-6. doi: 10.1086/517755. PMID: 9868693.
- Murphy TM, Deitz JM, Petersen PJ, Mikels SM, Weiss WJ. Therapeutic efficacy of GAR-936, a novel glycylcycline, in a rat model of experimental endocarditis. Antimicrob Agents Chemother. 2000 Nov;44(11):3022-7. doi: 10.1128/aac.44.11.3022-3027.2000. PMID: 11036017; PMCID: PMC101597.
- Lefort A, Lafaurie M, Massias L, Petegnief Y, Saleh-Mghir A, Muller-Serieys C, Le Guludec D, Fantin B. Activity and diffusion of tigecycline (GAR-936) in experimental enterococcal endocarditis. Antimicrob Agents Chemother. 2003 Jan;47(1):216-22. doi: 10.1128/aac.47.1.216-222.2003. PMID: 12499194; PMCID: PMC148965.
- Johnson JA, Feeney ER, Kubiak DW, Corey GR. Prolonged Use of Oritavancin for Vancomycin-Resistant Enterococcus faecium Prosthetic Valve Endocarditis. Open Forum Infect Dis. 2015 Oct 29;2(4):ofv156. doi: 10.1093/ofid/ofv156. PMID: 26677455; PMCID: PMC4677157.
- Krause KM, Renelli M, Difuntorum S, Wu TX, Debabov DV, Benton BM. In vitro activity of telavancin against resistant gram-positive bacteria. Antimicrob Agents Chemother. 2008 Jul;52(7):2647-52. doi: 10.1128/AAC.01398-07. Epub 2008 Apr 28. PMID: 18443122; PMCID: PMC2443888.
