
What do we want?
More nec fasc!
When do we want it?
Now!
Perhaps not a lot of people really want necrotizing fasciitis (see here), though to be fair, this post is not entirely about necrotizing fasciitis. In fact, this deals more with the “super saiyan” antigens, those toxins that group A strep and some staphylococci release that binds to the MHC, leading to activation of T-cells and subsequent cytokine storm. This generally represents a severe complication of group A streptococcus, especially trains that harbor predominant types 1 and 3 M proteins and secrete pyrogenic exotoxin (aka superantigen) A or B (1). It is the cross-linking of the major histocompatibility class II in antigen presenting cells and T cell receptors that lead to the release of cytokines, and subsequent vasodilatation and severe shock.
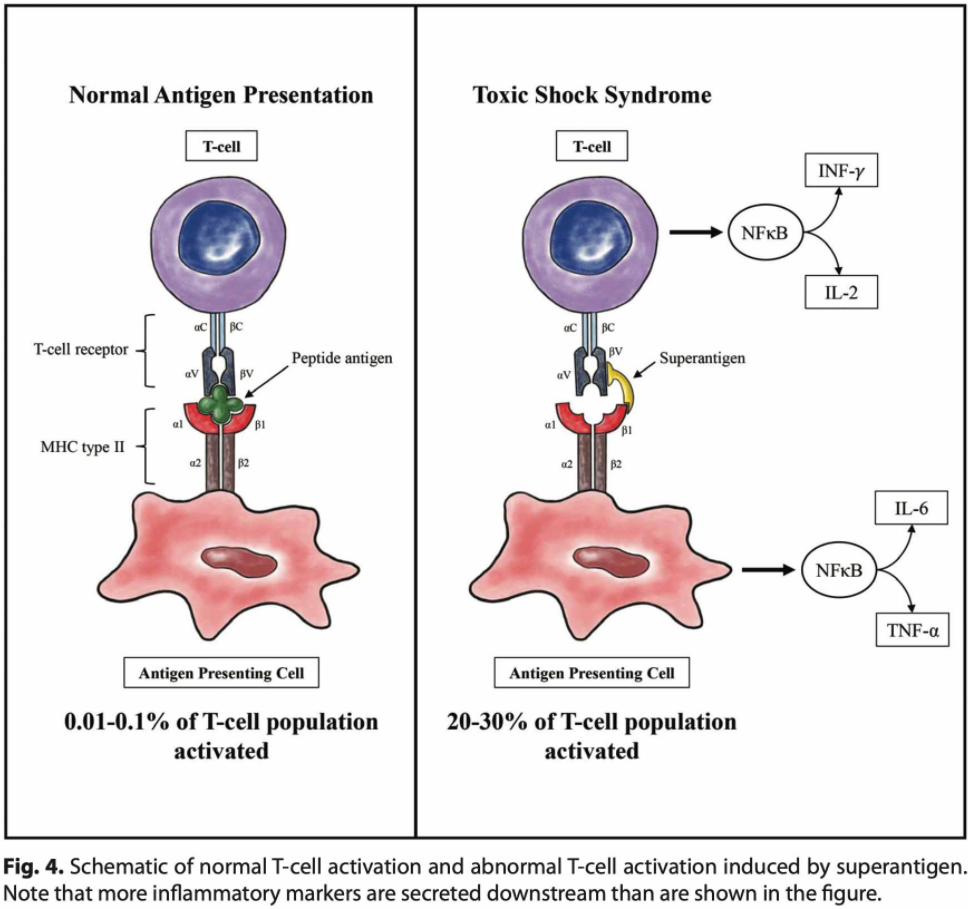
These antigens essentially bypass the normal mechanisms by which APCs activate T-cells. While I won’t go over the clinical manifestations, I think it is helpful to briefly touch on them:
- Phase 1: precedes hypotension by 24-48 hours, usually with non-specific, flu-like symptoms and GI symptoms. Look at skin for bullae and hyperalgesia of skin lesions
- Phase 2: pre-shock -> tachycardia, tachypnea, fever. If skin findings, watch for the POOP (pain out of proportion i.e. they are writing in pain and you touch the affected area and they’re not tender to palpation)
- Phase 3: baad shock.
One tip off here is having acute kidney injury on presentation. Here is the CDC definition:

Therapy involves antibiotics and, in the case of necrotizing fasciitis, surgical intervention (see here for hyperbaric oxygen). Group A streptococcus remains susceptible to penicillins, however monotherapy is associated with high morbidity and mortality. For instance, one review from the early 90s noted a mortality of 30% of reported cases of toxic shock syndrome (2, 3):

Further, there is a concern that, at high inoculum, penicillins may be less efficacious. Remember the Eagles? At least the Eagle effect. Named after Harry Eagle, this describes the phenomena when penicillins are not as effective in settings of high inoculum of bacteria in the micro lab (usually >107 cfu/mL). This is, at least when it comes to Staph aureus, due to expression of blaA and blaZ genes, which are beta-lactamases. This is usually described in cefazolin and may explain a lot of relapses in staphylococcal endocarditis. While this is cited as a concern, the pathophysiology of toxic shock syndrome is driven mostly by the superantigens rather than the bacteria itself. As a result, the name of the game tends to be to either 1) halt production of toxins and 2) inhibit toxins already made. For instance, in rabbits exposed intrabronchial to CA-MRSA (toxin producing) and purified staphylococcal toxin, all but one died from pulmonary hemorrhage (4). This was attenuated with vaccination against toxins:

Another study evaluated exposure of staphylococcal toxic shock syndrome antigen subcutaneously in rabbits over a period of 7 days. Exposed rabbits had high fevers, cachexia, and lethargy and died within a mean of 3.2 days (5). Further, exposure to increasing levels of pyrogenic toxin A was associated with higher mortality in rabbits:

Mechanism of Clindamycin/Linezolid
Since antigens are proteins, any antibiotic that impairs protein secretion may impair the production of these antigens. This is where clindamycin and linezolid come in. Both bind to the 50s subunit of the ribosome, impairing protein synthesis in bacteria and as a result, it inhibits the release of further toxins. Another advantage of these antibiotics is they are not affected by the size of the inoculum and their long post-antibiotic effect. Most of the studies on the impact of clindamycin in toxin production tend to be in vitro, but gives insight into their potential therapeutic impact.
An in vitro study (7) evaluated the efficacy of linezolid, penicillin, clindamycin, and a combination of group A strep growth and pyrogenic exotoxin A release. All antibiotics decreased growth of bacteria at 24 hours, without any statistical significance difference, although penicillin achieved 99.9% killing efficacy within 6 hours. In 2 different strains for group A strep, clindamycin, linezolid, and any combination with either antibiotic decreased pyrogenic toxin levels within 1 hours, though by 6 hours all antibiotics decreased it to a similar level:

In another (8) isolates of ampicillin and penicillin-resistant Staph aureus, clindamycin inhibited toxin productions when exposed to sub-MIC concentrations of clindamycin, despite the fact that bacterial growth was not inhibited:

Further, sub-MIC levels of clindamycin was associated with increased phagocytosis by PMNs and mononuclear cells as well as enhanced killing (9):

Moreover, clindamycin was associated with increased complement consumption as demonstrated by electron microscopy. The cell-surface M protein has been known to resist phagocytosis by inhibiting opsonization by the complement system.
Despite the ability of sub-MIC clindamycin to inhibit protein synthesis, when in the growth phase this is given also has an impact on toxin production. For instance, administration of clindamycin in the early-log phase growth was associated with increased levels of streptolysin O and other proteins, while adding clindamycin in the mid-log-phase of growth was associated with a reduction in exoproteins (10). Clinically, this likely has minimal importance as the combination of beta-lactam and clindamycin will result in fairly efficacious killing of bacteria as well as reduced toxin production.
Clinical Data for Clindamycin
There is not much robust clinical data here. Animal data suggests the impact of clindamycin on abscess size. In mice infected with 3 strains of group A streptococcal infection (one of which was clindamycin-resistant), skin lesion sizes were significantly reduced in those mice treated with clindamycin (GAS Cl529 is the clinda-resistant strain, 11):

Moreover, clindamycin also decreased DNase and SLO activity if above MIC, though these virulence factors were induced in sub-inhibitory concentrations of clindamycin.


One of the earliest clinical studies came from the pediatric literature. This retrospective, unblinded chart review (12) evaluated patients who presented with invasive group A streptococcal infections. Patients with deep infections who received clindamycin in combination with beta-lactams were more likely to have a favorable outcome (83% vs 14%, p=0.006). This was not seen in those with superficial infections, though the overall study was retrospective and small in terms of patient numbers/size. Another prospective observational study (13) of 67 patients with streptococcal toxic shock syndrome evaluated the effect of IVIG on 28 day mortality. 23 patients received IVIG compared to 44 who did not, with those receiving IVIG being more likely to have necrotizing fasciitis. Further, those in the IVIG group were younger and were more likely to receive clindamycin (91% vs 70%). In both simple and multiple logistic regression, clindamycin and IVIG were significantly associated with improved 28 day mortality:

Clindamycin also improved mortality in those who did not have necrotizing fasciitis (OR 4.6, 95% CI 1.2-17.8), though IVIG did not reach statistical significance for either non-nec fasc and nec fasc. Finally, a prospective surveillance study of 84 patients with invasive group A streptococcal infections evaluating the impact of IVIG and clindamycin (14). In univariate analysis, clindamycin was associated with reduced case fatality rate and the combination of clindamycin and IVIG was associated with lower mortality still, though this did not reach statistical significance:

Notably, only 53 patients received clindamycin while 14 received IVIG, so definitive conclusions could not be drawn.
The limited data makes it difficult to draw definitive conclusions, and the last 2 studies cited are confounded by the addition of IVIG. Despite this, there is a compelling argument to be made for the addition of clindamycin for patients who are suspected of having toxic shock syndrome, based on animal data suggesting the role toxins play in the pathophysiology as well as how clindamycin affects concentration of secreted toxins. Further, given the overwhelming shock these patients tend to be in, the addition of another antibiotic seems to be a fairly benign management decision.
Intravenous Immunoglobulin
The idea behind this is simple; if the superantigens work by cross-linking antigen presenting cells and T-cells, then neutralizing them by having them bind with other antibodies will prevent further cytokine storms. As mentioned above (13), multivariate analysis found that IVIG was associated with increased survival (OR 8.6, 95% CI 1.8-40.4), while there was a trend in another retrospective study (14).
A randomized, blinded, placebo-controlled trial evaluated patients with necrotizing soft tissue infection to either IVIG or placebo (15). Patients received IVIG or saline for 3 consecutive days, with primary outcome being patient-reported physical function based on the score of the Medical Outcomes Study 36-item short form health survey. 100 patients were randomized in a 1:1 fashion (50 each group, with more patients with group A strep being in the IVIG group), with median scores inthe PCS being non-statistical significantly different (36 in IVIG vs 31, p=0.81). There was no difference in mortality at 28 days, 90 days, or 180 days. Of course, despite this being a RCT, the primary outcome is not necessarily clinically relevant and it could be argued this study was underpowered to show mortality. Either way, the raw data does not suggest any differences in any result. A multicenter, randomized, double-blind, placebo controlled trial also evaluated the impact of IVIG in 28 day mortality (16). Only 21 patients were recruited, with mortality being 3.6-fold higher in the placebo group, though this did not reach statistical significance.

Notably, those who got IVIG had significantly lower SOFA scores, suggesting improvements in organ function:

In critically ill patients with vasopressor dependent shock and necrotizing fasciitis, 161 patients receiving IVIG were matched with 161 non-IVIG patients (17). IVIG had no impact on in-hospital mortality (OR 1, 95% CI 0.55-1.83). In matched patients, clindamycin also had no effect on mortality (IVIG mortality 26.8% vs 24.8%).
These data do not support the use of IVIG for toxic shock syndrome, however given the rarity of the disease, these studies are not adequately powered to show mortality benefit. A meta-analysis of 5 studies (one randomized), restricted to patients who received concurrent clindamycin, found that IVIG was associated with reduced mortality, from 33.7% to 15.7% (18)::

The authors do note a high risk of bias, and the reduction in mortality was seen when the data was pooled, likely reflecting the small sizes of individual studies (70 IVIG and 90 controls).
TL;DR
- Toxic shock syndrome, seen with group A streptococcus and some strains of staphylococcus aureus, is primarily a “superantigen” disease where these antigens cross-link antigen presenting cells with T-cells, leading to a massive release of cytokines
- These antigens drive the overwhelming shock seen here
- Clindamycin and linezolid suppress the production of toxin by inhibiting protein production
- Upfront therapy with a combination of a beta-lactam and clindamycin/linezolid is a reasonable approach for empiric therapy
- IVIG may have a role in lowering in-hospital mortality, though the data is not as robust and it is expensive.
- Despite this, therapy should also involve surgical intervention if necrotizing fasciitis is the source.
References:
- Schmitz, M., Roux, X., Huttner, B., & Pugin, J. (2018). Streptococcal toxic shock syndrome in the intensive care unit. Annals of intensive care, 8(1), 88. https://doi.org/10.1186/s13613-018-0438-y
- Stevens DL. Invasive group A streptococcus infections. Clin Infect Dis. 1992 Jan;14(1):2-11. doi: 10.1093/clinids/14.1.2. PMID: 1571429.
- Stevens DL, Tanner MH, Winship J, Swarts R, Ries KM, Schlievert PM, Kaplan E. Severe group A streptococcal infections associated with a toxic shock-like syndrome and scarlet fever toxin A. N Engl J Med. 1989 Jul 6;321(1):1-7. doi: 10.1056/NEJM198907063210101. PMID: 2659990.
- Strandberg KL, Rotschafer JH, Vetter SM, Buonpane RA, Kranz DM, Schlievert PM. Staphylococcal superantigens cause lethal pulmonary disease in rabbits. J Infect Dis. 2010 Dec 1;202(11):1690-7. doi: 10.1086/657156. Epub 2010 Oct 27. PMID: 20979456; PMCID: PMC2974057.
- Parsonnet J, Gillis ZA, Richter AG, Pier GB. A rabbit model of toxic shock syndrome that uses a constant, subcutaneous infusion of toxic shock syndrome toxin 1. Infect Immun. 1987 May;55(5):1070-6. doi: 10.1128/IAI.55.5.1070-1076.1987. PMID: 3570455; PMCID: PMC260470.
- Lee PK, Schlievert PM. Quantification and toxicity of group A streptococcal pyrogenic exotoxins in an animal model of toxic shock syndrome-like illness. J Clin Microbiol. 1989 Aug;27(8):1890-2. doi: 10.1128/JCM.27.8.1890-1892.1989. PMID: 2504778; PMCID: PMC267693.
- Coyle EA, Cha R, Rybak MJ. Influences of linezolid, penicillin, and clindamycin, alone and in combination, on streptococcal pyrogenic exotoxin a release. Antimicrob Agents Chemother. 2003 May;47(5):1752-5. doi: 10.1128/aac.47.5.1752-1755.2003. PMID: 12709354; PMCID: PMC153301.
- Schlievert PM, Kelly JA. Clindamycin-induced suppression of toxic-shock syndrome–associated exotoxin production. J Infect Dis. 1984 Mar;149(3):471. doi: 10.1093/infdis/149.3.471. PMID: 6715902.
- Gemmell CG, Peterson PK, Schmeling D, Kim Y, Mathews J, Wannamaker L, Quie PG. Potentiation of opsonization and phagocytosis of Streptococcus pyogenes following growth in the presence of clindamycin. J Clin Invest. 1981 May;67(5):1249-56. doi: 10.1172/jci110152. PMID: 7014632; PMCID: PMC370690.
- Sawai J, Hasegawa T, Kamimura T, Okamoto A, Ohmori D, Nosaka N, Yamada K, Torii K, Ohta M. Growth phase-dependent effect of clindamycin on production of exoproteins by Streptococcus pyogenes. Antimicrob Agents Chemother. 2007 Feb;51(2):461-7. doi: 10.1128/AAC.00539-06. Epub 2006 Nov 13. PMID: 17101685; PMCID: PMC1797754.
- Andreoni F, Zürcher C, Tarnutzer A, Schilcher K, Neff A, Keller N, Marques Maggio E, Poyart C, Schuepbach RA, Zinkernagel AS. Clindamycin Affects Group A Streptococcus Virulence Factors and Improves Clinical Outcome. J Infect Dis. 2017 Jan 15;215(2):269-277. doi: 10.1093/infdis/jiw229. PMID: 27247345.
- Zimbelman J, Palmer A, Todd J. Improved outcome of clindamycin compared with beta-lactam antibiotic treatment for invasive Streptococcus pyogenes infection. Pediatr Infect Dis J. 1999 Dec;18(12):1096-100. doi: 10.1097/00006454-199912000-00014. PMID: 10608632.
- Linnér A, Darenberg J, Sjölin J, Henriques-Normark B, Norrby-Teglund A. Clinical efficacy of polyspecific intravenous immunoglobulin therapy in patients with streptococcal toxic shock syndrome: a comparative observational study. Clin Infect Dis. 2014 Sep 15;59(6):851-7. doi: 10.1093/cid/ciu449. Epub 2014 Jun 13. PMID: 24928291.
- Carapetis JR, Jacoby P, Carville K, Ang SJ, Curtis N, Andrews R. Effectiveness of clindamycin and intravenous immunoglobulin, and risk of disease in contacts, in invasive group a streptococcal infections. Clin Infect Dis. 2014 Aug 1;59(3):358-65. doi: 10.1093/cid/ciu304. Epub 2014 Apr 29. PMID: 24785239.
- Madsen MB, Hjortrup PB, Hansen MB, Lange T, Norrby-Teglund A, Hyldegaard O, Perner A. Immunoglobulin G for patients with necrotising soft tissue infection (INSTINCT): a randomised, blinded, placebo-controlled trial. Intensive Care Med. 2017 Nov;43(11):1585-1593. doi: 10.1007/s00134-017-4786-0. Epub 2017 Apr 18. PMID: 28421246.
- Darenberg J, Ihendyane N, Sjölin J, Aufwerber E, Haidl S, Follin P, Andersson J, Norrby-Teglund A; StreptIg Study Group. Intravenous immunoglobulin G therapy in streptococcal toxic shock syndrome: a European randomized, double-blind, placebo-controlled trial. Clin Infect Dis. 2003 Aug 1;37(3):333-40. doi: 10.1086/376630. Epub 2003 Jul 17. PMID: 12884156.
- Kadri SS, Swihart BJ, Bonne SL, Hohmann SF, Hennessy LV, Louras P, Evans HL, Rhee C, Suffredini AF, Hooper DC, Follmann DA, Bulger EM, Danner RL. Impact of Intravenous Immunoglobulin on Survival in Necrotizing Fasciitis With Vasopressor-Dependent Shock: A Propensity Score-Matched Analysis From 130 US Hospitals. Clin Infect Dis. 2017 Apr 1;64(7):877-885. doi: 10.1093/cid/ciw871. PMID: 28034881; PMCID: PMC5850528.
- Parks T, Wilson C, Curtis N, Norrby-Teglund A, Sriskandan S. Polyspecific Intravenous Immunoglobulin in Clindamycin-treated Patients With Streptococcal Toxic Shock Syndrome: A Systematic Review and Meta-analysis. Clin Infect Dis. 2018 Oct 15;67(9):1434-1436. doi: 10.1093/cid/ciy401. PMID: 29788397; PMCID: PMC6186853.
