
Staphylococcus Aureus is a tough disease to treat, but luckily for MSSA we have pretty good antibiotics to treat this beast. The choice is usually between cefazolin, a first-generation cephalosporin, and Nafcillin, an anti-staphylococcal penicillin. My experience has been that cefazolin is usually the go to antibiotic for MSSA bacteremia, with nafcillin having a niche in MSSA infections where you need high CNS penetration. For a while, however, there was a debate as to the risk of relapse in certain infections with the use of cefazolin due to the inoculum effect.
The Eagle Effect:
This was described originally in 1948 by Harry Eagle (yeah, surprising). The original Eagle Effect, however, deals with increasing doses of penicillin having lower efficacy (1) and not necessarily that high bacterial inoculum leads to decreased efficacy of antibiotics. Where would one see high concentration of bacteria? Typically, in severe infection such as osteomyelitis, line associated infections, and infective endocarditis (i.e. lots of purulence in an area = high density of bacteria). It is unclear of what the mechanism is. One review suggests several mechanisms (2):
- The amount of antibiotics that interact with an individual bacterial cell decreases with higher antibiotic dose
- Biofilms leads to decreased interaction of antibiotics with bacteria
- Expression of proteins that decreased antibiotics susceptibility
- Enzymatic degradation of antibiotic
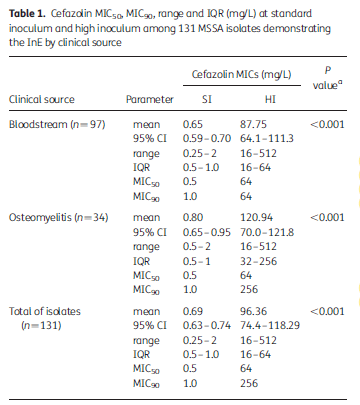
This last one has been the topic of interest. There have been 4 types of staphylococcal beta-lactamase enzymes that have been characterized based on their substrate specificity and amino acid sequence (3). Of these, 2 have been suggested to play a role in the inoculum effect, type A and type C, as they tend to hydrolyze cefazolin more effectively. Most of this data is in vitro, however. In one study from South America (3) evaluated 364 MSSA isolates from 2 prospective studies. They tested MIC to cefazolin at standard inoculum (105 cfu/mL) and high inoculum (107 cfu/ml), with inoculum effect defined as an MIC of >16 at high inoculum. Of these, 131 demonstrated high inoculum effect, with the percentage of isolates ranging from 37% to 63% that demonstrated this:
The prevalence of these strains of MSSA was evaluated in another study (4) from the US, where 308 isolates were evaluated. Here, 45 isolates displayed inoculum effect, of which 25 had type C gene and 17 had the type A gene. In another study (5), 88 MSSA strains were obtained from patients with complicated SSTI, HAP, or infective endocarditis. Type A and C strains had an increase in MIC when tested at a high inoculum:

24 strains from hemodialysis patients with bacteremia were also evaluated. Six of these strains showed the inoculum effect, resulting in at least 3 failures in those treated with cefazolin.
The data suggest that certain beta-lactamases are responsible for the inoculum effect seen with cefazolin.
Clinical Data
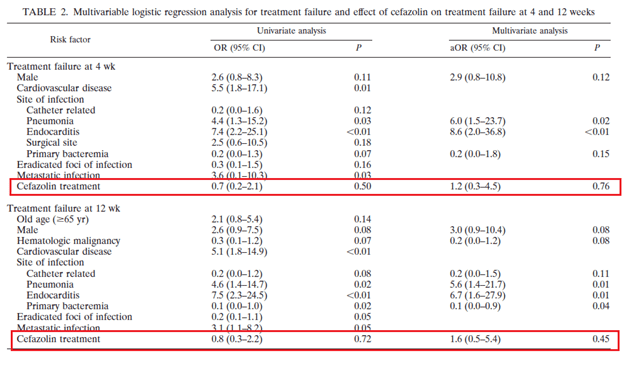
The microbiological data is compelling and would suggest the use of nafcillin or another type of anti staphylococcal penicillin for severe MSSA infections. Despite this, clinical data suggests there is no difference in terms of patient centered outcomes when comparing both types of antibiotics. While this data comes mostly from cohort studies, it is indeed compelling. A retrospective, propensity score matched study (6) evaluated 133 patients treated with either cefazolin or nafcillin. Treatment failure rates was similar in both groups, 15%, and logistic regression analysis did not find that treatment failure at 4 or 12 weeks was associated with cefazolin use:

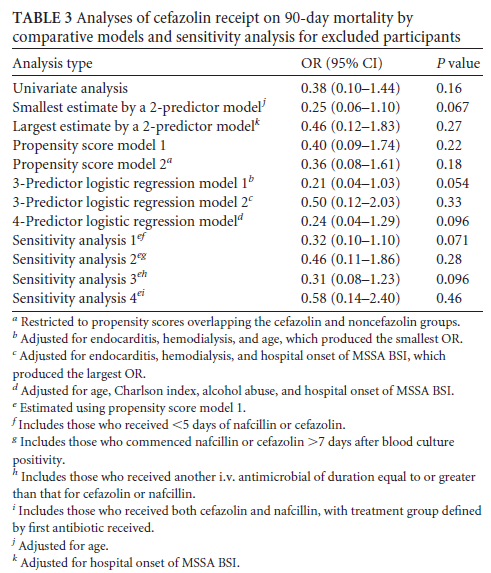
Another study (7) evaluated 90 day mortality in 100 patients treated with either nafcillin or cefazolin for MSSA bacteremia. Notably, a higher proportion of patients who got nafcillin were IVDU or had alcohol abuse, and a higher proportion of patients in the nafcillin group were admitted to the ICU. After propensity score matching, cefazolin use was not associated with a difference in 90 day mortality:
A larger retrospective VA study (8) evaluated 30 day and 90 day all cause mortality in those patients treated with either cefazolin or nafcillin/oxacillin for all MSSA infections. 3167 patients were included, of which 1163 got cefazolin and 2004 got either nafcillin/oxacillin. Notably, patients who got cefazolin were more likely to have ESRD or diabetes, though those who got nafcillin/oxacillin were more likely to have endocarditis or other hospital acquired infection. Regardless, cefazolin was associated with decreased 30 day and 90 day mortality when compared to nafcillin and both had similar recurrence rates:

Another large retrospective cohort (9) from Canada evaluated the use of cloxacillin and cefazolin in 354 patients with MSSA bacteremia. The use of cefazolin was not associated with increased 90 day mortality, though there was a trend towards reduced mortality:
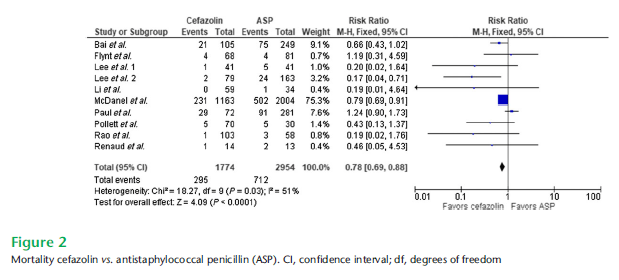
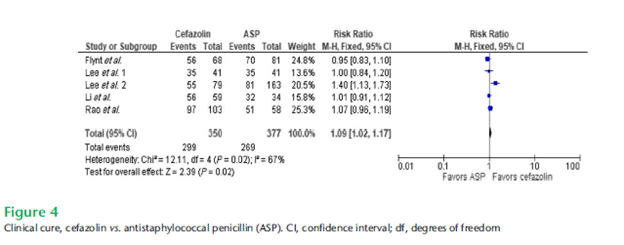
Though cefazolin use was associated with a higher rate of relapse (6% vs 2%), with all relapse cases in the cefazolin group having a deep-seated infection. A meta-analysis (10) of nafcillin vs cefazolin in MSSA bacteremia found that cefazolin was associated with improved mortality, and had similar clinical cure rates as antistaphylococcal penicillin:
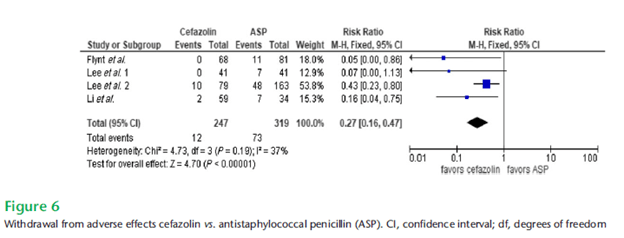
Further, anti-staphylococcal penicillins were associated with more discontinuation due to adverse events:
A prospective study (11) used propensity matching to compare 79 patients with MSSA bacteremia who got nafcillin with 79 patients who got cefazolin. Those who got cefazolin were less likely to have treatment failure and decreased mortality at 90 days which was attributed to the higher rate of discontinuation of nafcillin. Notably, in those with sepsis the mortality was not statistically different between groups (I am assuming due to shorter duration of therapy).
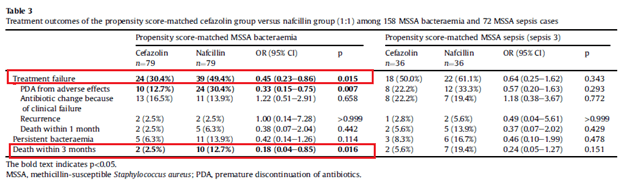
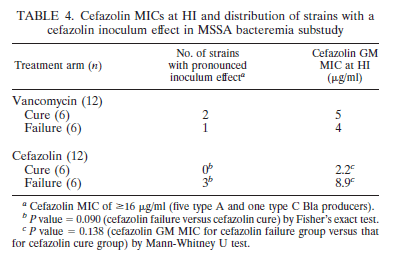
They further looked into the cefazolin inoculum effect and found that the treatment failure rate was not different overall in those with a positive inoculum effect or negative inoculum effect, but it impacted the patients who got cefazolin in both mortality and treatment failure:

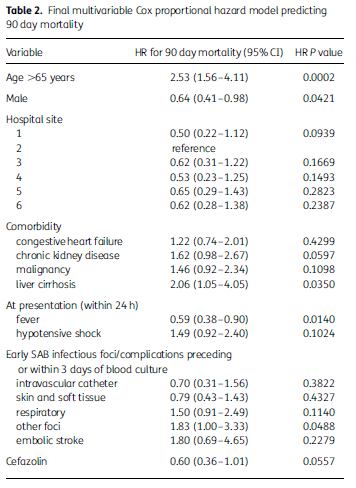
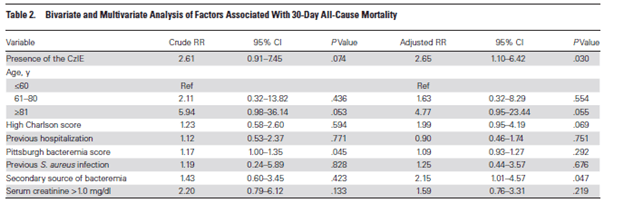
This was confirmed in another study (12) that evaluated 35 patients with negative inoculum effect and 42 with a positive inoculum effect. In the multivariate model, the presence of inoculum effect was associated with an increased 30 day mortality:
This suggests that, in the absence of the inoculum effect, cefazolin and anti-staphylococcal penicillins have similar outcomes for MSSA infections and MSSA bacteremia. This is crucial, since cefazolin has a lower incidence of adverse events, such as renal injury, thrombocytopenia, and hepatotoxicity (13). Unfortunately, there is no Bla gene sequencing that we can do for blood cultures as of now. A retrospective study (14) was able to find that resistance to clindamycin (OR 3.55, 95% CI 1.62-7.8) and erythromycin (OR 5, 85% CI 2.5-9.99) was associated with cefazolin inoculum effect positivity, with high specificities (92.9% for clindamycin and 90.9% for erythromycin) and negative predictive values (82.3% and 84.6%, respectively).
TL;DR
- The inoculum effect refers to the decreased efficacy of cefazolin at high inoculum (typically 107 cfu/mL in the micro lab).
- This is likely due to staphylococcal beta-lactamases, usually type A and type C. This is seen in the microbiological lab by a rise of MIC to >16 at high inoculum
- Clinically, the data does not suggest that cefazolin is inferior to nafcillin in the vast majority of cases, however the inoculum effect is associated with higher rates of relapse
- Resistance to clindamycin and erythromycin may be used as a surrogate for the inoculum effect
References:
- EAGLE H, MUSSELMAN AD. The rate of bactericidal action of penicillin in vitro as a function of its concentration, and its paradoxically reduced activity at high concentrations against certain organisms. J Exp Med. 1948;88(1):99-131. doi:10.1084/jem.88.1.99
- Lenhard JR, Bulman ZP. Inoculum effect of β-lactam antibiotics. J Antimicrob Chemother. 2019;74(10):2825-2843. doi:10.1093/jac/dkz226
- Rincón S, Reyes J, Carvajal LP, et al. Cefazolin high-inoculum effect in methicillin-susceptible Staphylococcus aureus from South American hospitals. J Antimicrob Chemother. 2013;68(12):2773-2778. doi:10.1093/jac/dkt254
- Wang SK, Gilchrist A, Loukitcheva A, et al. Prevalence of a Cefazolin Inoculum Effect Associated with blaZ Gene Types among Methicillin-Susceptible Staphylococcus aureus Isolates from Four Major Medical Centers in Chicago. Antimicrob Agents Chemother. 2018;62(8):e00382-18. Published 2018 Jul 27. doi:10.1128/AAC.00382-18
- Nannini EC, Stryjewski ME, Singh KV, et al. Inoculum effect with cefazolin among clinical isolates of methicillin-susceptible Staphylococcus aureus: frequency and possible cause of cefazolin treatment failure. Antimicrob Agents Chemother. 2009;53(8):3437-3441. doi:10.1128/AAC.00317-09
- Lee S, Choe PG, Song KH, et al. Is cefazolin inferior to nafcillin for treatment of methicillin-susceptible Staphylococcus aureus bacteremia?. Antimicrob Agents Chemother. 2011;55(11):5122-5126. doi:10.1128/AAC.00485-11
- Pollett S, Baxi SM, Rutherford GW, Doernberg SB, Bacchetti P, Chambers HF. Cefazolin versus Nafcillin for Methicillin-Sensitive Staphylococcus aureus Bloodstream Infection in a California Tertiary Medical Center. Antimicrob Agents Chemother. 2016;60(8):4684-4689. Published 2016 Jul 22. doi:10.1128/AAC.00243-16
- McDanel JS, Roghmann MC, Perencevich EN, et al. Comparative Effectiveness of Cefazolin Versus Nafcillin or Oxacillin for Treatment of Methicillin-Susceptible Staphylococcus aureus Infections Complicated by Bacteremia: A Nationwide Cohort Study. Clin Infect Dis. 2017;65(1):100-106. doi:10.1093/cid/cix287
- Bai AD, Showler A, Burry L, et al. Comparative effectiveness of cefazolin versus cloxacillin as definitive antibiotic therapy for MSSA bacteraemia: results from a large multicentre cohort study. J Antimicrob Chemother. 2015;70(5):1539-1546. doi:10.1093/jac/dku560
- Rindone JP, Mellen CK. Meta-analysis of trials comparing cefazolin to antistaphylococcal penicillins in the treatment of methicillin-sensitive Staphylococcus aureus bacteraemia. Br J Clin Pharmacol. 2018;84(6):1258-1266. doi:10.1111/bcp.13554
- Lee S, Song KH, Jung SI, et al. Comparative outcomes of cefazolin versus nafcillin for methicillin-susceptible Staphylococcus aureus bacteraemia: a prospective multicentre cohort study in Korea. Clin Microbiol Infect. 2018;24(2):152-158. doi:10.1016/j.cmi.2017.07.001
- Miller WR, Seas C, Carvajal LP, et al. The Cefazolin Inoculum Effect Is Associated With Increased Mortality in Methicillin-Susceptible Staphylococcus aureus Bacteremia. Open Forum Infect Dis. 2018;5(6):ofy123. Published 2018 May 23. doi:10.1093/ofid/ofy123
- Eljaaly K, Alshehri S, Erstad BL. Systematic Review and Meta-analysis of the Safety of Antistaphylococcal Penicillins Compared to Cefazolin. Antimicrob Agents Chemother. 2018;62(4):e01816-17. Published 2018 Mar 27. doi:10.1128/AAC.01816-17
- Song KH, Jung SI, Lee S, et al. Characteristics of cefazolin inoculum effect-positive methicillin-susceptible staphylococcus aureus infection in a multicentre bacteraemia cohort. Eur J Clin Microbiol Infect Dis. 2017;36(2):285-294. doi:10.1007/s10096-016-2799-

1 comments on “Staphylococcus Aureus, the Inoculum Effect, Cefazolin, and Nafcillin: The Odyssey”