
If you get nothing from this, just remember: TMP-SMX, fluroquinolones, minocycline. These tend to be good antibiotic options for this bug. Also, make sure if you isolate this from a trach or a endotracheal tube that there are signs of infection before you proceed with treatment as this can colonize plastic!
Stenotrophomonas maltophilia is a non-fermenting, aerobic gram negative rod that was formally known as Pseudomonas maltophilia and subsequently Xanthomonas (1). This is an organism that is typically seen in nosocomial infections, with its prevalence increasing over the past decades (1). It has been described as an environmental global emerging MDRO due to its multiple resistance mechanisms (2), and it has been isolated in basically anything that is wet and plastic (2). Basically, if you can think of a moist environment, it has been isolated from there (2). It has a particular ability to form biofilms, however it has relatively low virulence (2,3). As such, risk factors for this infection include immunosuppression, prolonged ICU stay, HIV infection, cystic fibrosis, mechanical ventilation and indwelling catheters (again, plastic stuff -> biofilm formation), not to mention corticosteroids and immunosuppressants (1-3).
Basics of Stenotrophomonas
S. maltophilia has an impressive resistance pattern, in part due to its intrinsic beta-lactamases, efflux pump systems, and changes in the outer membrane and target site modifications (1)
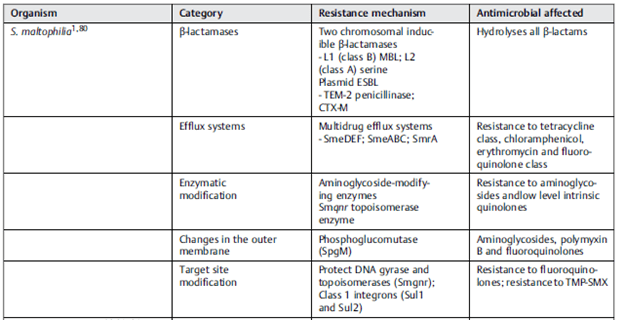
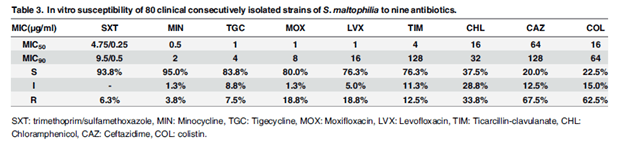
From a prior post, you can see the beta-lactamases tends to fall under the class A and class B Ambler classification. For a brief refresher, ambler class A tends to have ESBL as well as carbapenemases. Further, class B also tends to be carbapenamases. As such, most beta-lactams are not going to work here. Also remember that the original 3 beta-lactamase inhibitors (tazobactam, clavulonate, sulbactam) work on class A but not class B. Due to this, there is a limited number of therapeutic options available. TMP/SMX and quinolones tend to be first line therapy. An analysis of 80 clinical isolates (4) found that TMP-SMX, minocycline, and quinolones had favorable susceptibility patterns:
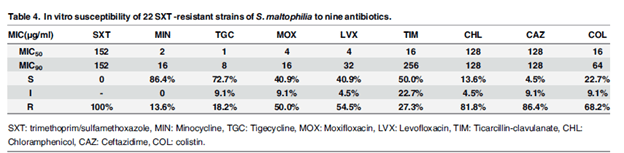
In TMP-SMX resistant specimens, minocycline was the most favorable:
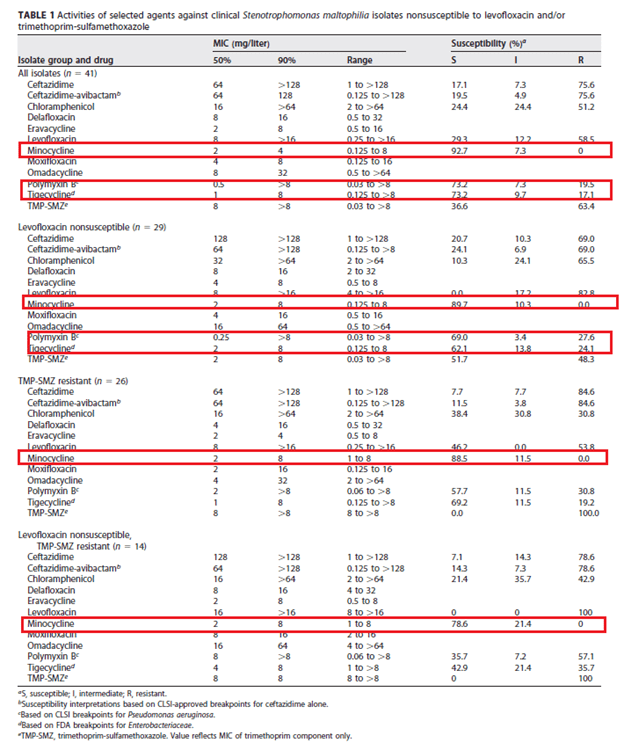
In the time-kill experiments, there was no significant synergism except for TMP-SMX and moxifloxacin, moxifloxacin + minocycline, and moxifloxacin + tigecycline. This pattern also held true in a study of 41 clinical isolates of S. maltophilia that were TMP-SMX resistant and nonsusceptible to levofloxacin (or, just resistant):
Cefiderocol, along with minocycline, were also found to be susceptible in a study of 37 isolates resistant to TMP-SMX and nonsusceptible to levofloxacin (6):
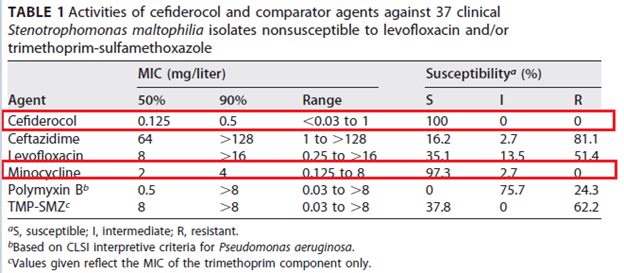
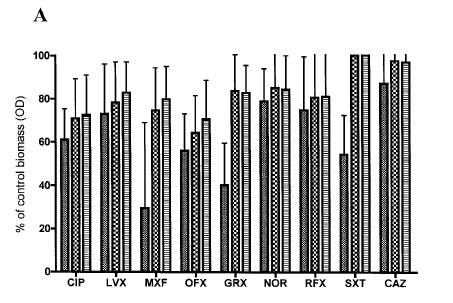
Notably, cefiderocol actually displayed synergy when compared with levofloxacin, minocycline, polymyxin B, or TMP-SMX, though the numbers were small. Avibactam was also found to inhibit the L2 beta-lactamase, restoring susceptibility when combined with aztreonam (7). Interestingly, certain antibiotics can affect the biofilm differently. For instance, one study (8) found all fluroquinolones decreased the biomass of S. melophilia biofilm at sub-inhibitory concentrations in a dose dependent manner, with rufloxicin having the most activity. Comparably, while TMP-SMX also exhibited reduction in biomass at certain concentrations, the same was not true for ceftazidime.
Clinical data – pulmonary infections
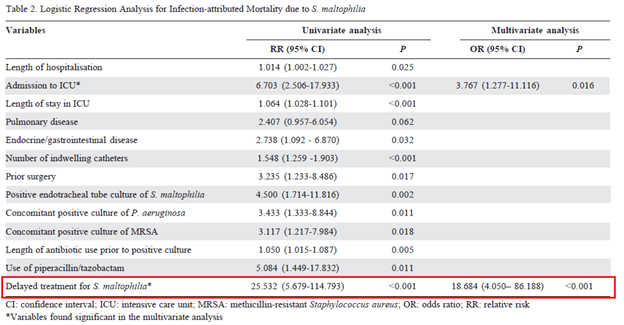
One of the most common manifestations of Stenotrophomnas infections are pulmonary infections. Differentiating between colonization and infection tends to be difficult, especially in the ICU setting. For instance, a retrospective study (9) of 143 patients found the difference between infected and colonized patients was a higher APACHE score. A cohort study of 89 patients with positive respiratory tract for S. maltophilia did not find that targeted therapy (p-value 0.485) was associated with worse outcomes (10). Indeed, it shouldn’t be surprising that those who were likely to die were more likely to be on mechanical ventilation, have higher APACHE II scores or have lower serum albumin. This study, however, excluded patients with radiographic evidence of pneumonia. These data contrast a retrospective study of 150 cases (11), in which a logistic regression analysis found that delay in S. maltophilia treatment was significantly associated with infection-attributed mortality due to S. maltophilia:
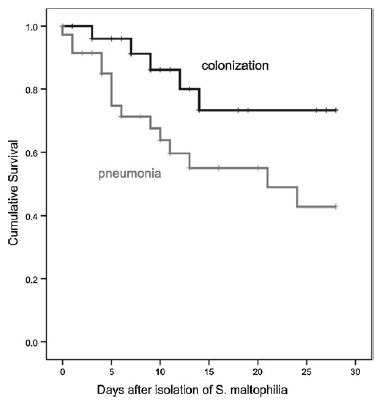
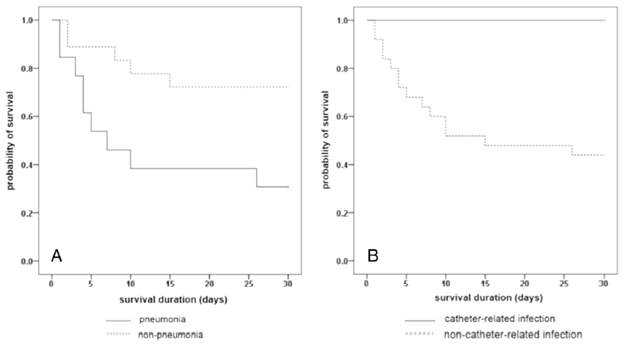
Not surprisingly, pneumonia with S. maltophilia is associated with worse outcomes. A retrospective cohort of 64 ICU patients (12) found higher mortality in patients who were diagnosed with S. maltophilia pneumonia compared with colonization at 30 days:
Indeed, isolation of S. maltophilia in the absence of new clinical symptoms or infiltrates should not prompt initiation of targeted therapy.
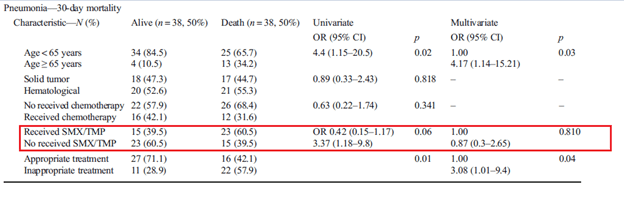
Having said that, the utility of early empiric therapy tends to be questionable in certain studies. In a retrospective cohort study of 76 patients (13) with confirmed pneumonia, receipt of TMP-SMX was associated with improvement in mortality in univariate analysis. Multivariate analysis found that inappropriate treatment was associated with higher 30 day mortality:
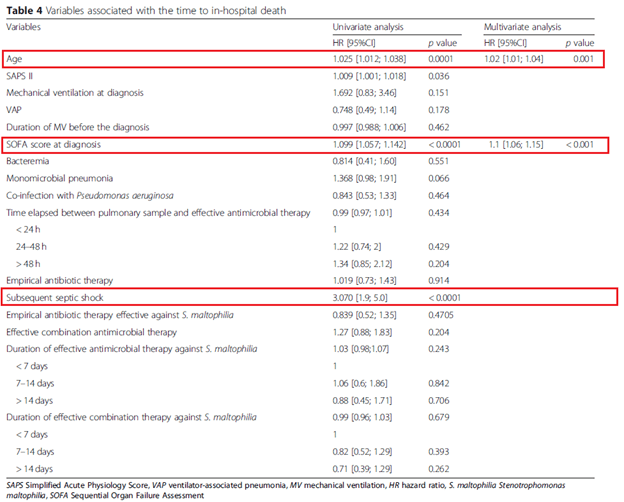
Two other retrospective studies suggest no difference between treatment and no treatment. For instance, a retrospective study (14) of 40 patients found the only thing associated with mortality was low albumin content (p-value 0.024) and hypotension (p-value 0.027) in univariate analysis. In multivariate analysis, these same factors were associated with mortality. Therapy for S.maltophilia was not associated with improved mortality. In the ICU setting, 282 patients were retrospectively analyzed (15). Univariate and multivariate analysis did not find that targeted therapy was associated with improved outcomes:
It is difficult to make sense of this. For one, it could be that S. maltophilia is actually a marker of underlying illness severity. Indeed, many of these patients averaged a length of hospital stay ranging from 17 days to up to 30 and even beyond, suggesting that infection is overall a marker of subsequent “badness.” It could also be argued that many times, therapy is delayed, however this does not seem to be the case.
Clinical data – bloodstream infections
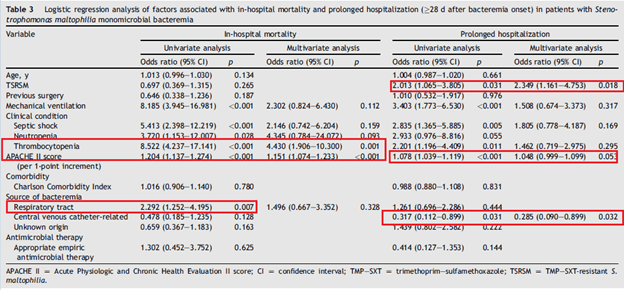
The other common disease associated with S. maltophilia is bacteremia. How to interpret a blood culture positive to Stenotrophomonas is not a mystery. A 10 year retrospective cohort study (16) compared outcomes in TMP-SMX resistant and sensitive monomicrobial bacteremia. 14 day mortality was comparable in both groups (24.2% vs 23.2%) as was in-hospital mortality (50% in the sensitive group vs 41.1% in the resistant group, p-value 0.264). Multivariate analysis did not find appropriate empiric antimicrobial therapy to be associated with in-hospital mortality or prolonged hospitalization:
In a previously cited retrospective study of oncology patients (13), the only factor associated in univariate and multivariate analysis found that CVC removal was the only factor associated with improved mortality:

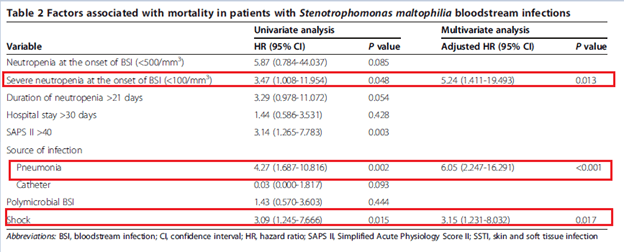
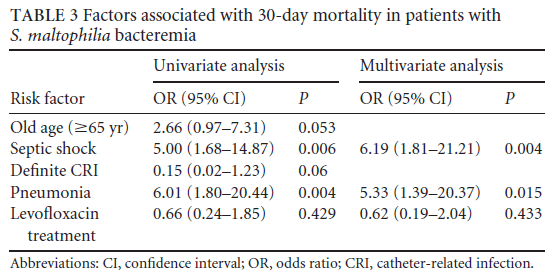
In hematological patients, 31 retrospective cases of S. maltophilia bacteremia were evaluated (17). In this cohort, univariate and multivariate analysis found that severe neutropenia, pneumonia as source of infection, and shock were independently associated with worse 30d mortality:
Fluroquinolones vs TMP-SMX
Several studies have compared the two front-line therapies. For instance, a cohort study compared 53 patients treated with TMP-SMX and 35 patients treated with levofloxacin and compared 30 day mortality (18). There was no difference in terms of 30 day mortality, length of hospital stay, or recurrent bacteremia, though patients in the TMP-SMX group were more likely to have adverse events:

Multivariate analysis did not find levofloxacin to be associated with worse 30 day mortality, though pneumonia as a source of bacteremia was significantly associated with worse mortality:
This was also confirmed in another cohort study. 98 patients were evaluated, of which 35 got TMP-SMX and 63 got a FQ (19). Microbiological cure was achieved in 62% of FQ patients and 65% of TMP-SMX patients (p-value 0.832). 30 day mortality was 31% in the FQ group vs 22% in the TMP-SMX (p-value 0.42). This pattern held true regardless of the presumed source of bacteremia.
A meta-analysis of 14 studies (20) found that FQ use was associated with survival benefit over TMP-SMX (I2 = 18%). When evaluating specific agents, such as ciprofloxacin or levofloxacin, there was no significant difference in comparison with TMP-SMX.

Overall, seems that both FQ and TMP-SMX tend to be good options for therapy, as far as clinical data is concerned. While in-vitro data also suggest minocycline is a reasonable option, data tends to be restricted to case series. Further, ceftazidime, while being susceptible in some cases, does not seem to be a good choice, as the resistance patterns do not favor its use not to mention the lack of biofilm activity. Tigecycline and polymyxin B are also susceptible but given its toxicity profile, I would not pursue these. Avibactam, in combination with ceftazidime-avibactam is also a reasonable option if resistance to TMP-SMX is a concern.
Combination therapy?
The idea behind combination therapy was proposed in the early 2000s for VAP, given the concern for Pseudomonas. For instance, an RCT evaluated 740 ventilated patients with suspected VAP who were colonized with pseudomonas or MRSA (21). Patients were allocated meropenem + ciprofloxacin or meropenem alone and found no difference in 28 day mortality between groups (RR 1.05, 95% CI 0.78-1.42). What is the rationale here? A review notes the rationale behind this is one of the following 3 reasons (22):
- Broaden empiric therapy (i.e. 2 antibiotics may lead to 100% coverage)
- Synergy
- Prevent resistance from developing (similar to TB therapy or ART in HIV)
Indeed, this same review found increased mortality in patients who were given inappropriate empiric therapy for Pseudomonas (22) in several studies. While this review goes over beta-lactam based combination therapies, as I mentioned above, this may not necessarily apply for Stenotrophomonas given its intrinsic resistance to most beta-lactams. The point here is it may not necessarily help.
For Stenotrophomonas, I mentioned previously that in vitro data for combination with cefidericol tends to favor the combination therapy (6). An interesting study evaluated in vitro data for TMP-SMX combination therapy as well as evaluating clinical data within the same study (23). In the in vitro portion of the study, 89 strains were evaluated, which found that most of the combination therapies were showed either no interaction or some synergy with only the TMP-SMX and levofloxacin combination showing a degree of antagonism:
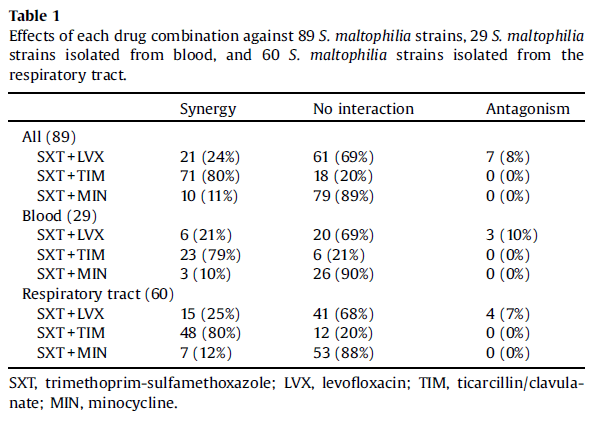
In the clinical data, there was no beneficial benefits in the 30 day mortality rate for the combination therapy compared to the monotherapy (p-value 0.64). This similar pattern was seen in a previously cited study in terms of in vitro data (18), with TMP-SMX finding at least no antagonism when compared with either ticarcillin-clavulonic acid, or levofloxacin or moxifloxacin:

A retrospective study (24) evaluated the same question in pneumonia patients. There was no difference in mortality between the monotherapy and combination therapy in mortality (22% vs 29%, p-value 0.547), clinical response (56% vs 66%, p-value 0.404) or microbiologic eradication (63% vs 72%, p-value 0.455). At the end of the day, combination therapy would depend on an institution’s antibiogram if there is significant resistance. In other words, if any given drug has low susceptibility (i.e lower than 70% for each), then it may be reasonable to proceed with dual therapy until susceptibilities return for the purpose of covering Stenotrophomonas. There is no benefit to this in terms of clinical data.
Approach to Stenotrophomonas
I mentioned before that isolating this from blood is not a mystery; this should be treated. In terms of pulmonary infection, there should be an infiltrate plus radiographic evidence as this can be isolated from plastics such as CVC and endotracheal tubes. If this is isolated, TMP-SMX at 15mg/kg divided into 3-4 doses is a reasonable approach. Levofloxacin 750mg daily is also reasonable. If these are resistant, minocycline 200mg followed by 100mg q12h is reasonable as well. While I advocate for minocycline given its better profile, I do not go against TMP-SMX per UpToDate (though to be fair, I worked with the main author of the UpToDate article on Stenotrophomonas, so I may be biased. Given that, I recommend reading that if you have access. I trust the author more than myself). Duration of therapy is up in the air, but 7 days for pneumonia and 2 weeks for bacteremia is reasonable, though this is based on hospitalized patients. I suspect that shorter therapy is reasonable, but given I think this organism is more of a marker of “badness” and prolonged hospitalization is a risk factor, 7 and 14 days as therapy is a reasonable therapeutic goal unless there is more clinical data to suggest otherwise.
TL;DR:
- Stenotrophomonas is an GNR that is of low virulence, tends to make biofilms, and infects those who are immunosuppressed
- Most common presentations are pneumonia and bacteremias
- Colonization with stenotrophomonas does not portend worse outcomes
- TMP-SMX and FQs are first line therapies followed by ceftazidime or ceftazidime-avibactam, tigecycline, polymyxin B
- Dual therapy depends on institutional antibiogram; if susceptibility is roughly 70% for any given antibiotic, it may be reasonable to use dual therapy until susceptibilities come back. After that, de-escalating to one drug is reasonable
- 7 days for pneumonia and 14 days for bacteremia is reasonable.
References:
- Abbott IJ, Peleg AY. Stenotrophomonas, Achromobacter, and nonmelioid Burkholderia species: antimicrobial resistance and therapeutic strategies. Semin Respir Crit Care Med. 2015 Feb;36(1):99-110. doi: 10.1055/s-0034-1396929. Epub 2015 Feb 2. PMID: 25643274.
- Brooke JS. Stenotrophomonas maltophilia: an emerging global opportunistic pathogen. Clin Microbiol Rev. 2012 Jan;25(1):2-41. doi: 10.1128/CMR.00019-11. PMID: 22232370; PMCID: PMC3255966.
- Chang, Y. T., Lin, C. Y., Chen, Y. H., & Hsueh, P. R. (2015). Update on infections caused by Stenotrophomonas maltophilia with particular attention to resistance mechanisms and therapeutic options. Frontiers in microbiology, 6, 893. https://doi.org/10.3389/fmicb.2015.00893
- Wei C, Ni W, Cai X, Zhao J, Cui J. Evaluation of Trimethoprim/Sulfamethoxazole (SXT), Minocycline, Tigecycline, Moxifloxacin, and Ceftazidime Alone and in Combinations for SXT-Susceptible and SXT-Resistant Stenotrophomonas maltophilia by In Vitro Time-Kill Experiments. PLoS One. 2016 Mar 21;11(3):e0152132. doi: 10.1371/journal.pone.0152132. PMID: 26999818; PMCID: PMC4801212.
- Biagi M, Tan X, Wu T, Jurkovic M, Vialichka A, Meyer K, Mendes RE, Wenzler E. Activity of Potential Alternative Treatment Agents for Stenotrophomonas maltophilia Isolates Nonsusceptible to Levofloxacin and/or Trimethoprim-Sulfamethoxazole. J Clin Microbiol. 2020 Jan 28;58(2):e01603-19. doi: 10.1128/JCM.01603-19. PMID: 31748318; PMCID: PMC6989059.
- Biagi M, Vialichka A, Jurkovic M, Wu T, Shajee A, Lee M, Patel S, Mendes RE, Wenzler E. Activity of Cefiderocol Alone and in Combination with Levofloxacin, Minocycline, Polymyxin B, or Trimethoprim-Sulfamethoxazole against Multidrug-Resistant Stenotrophomonas maltophilia. Antimicrob Agents Chemother. 2020 Aug 20;64(9):e00559-20. doi: 10.1128/AAC.00559-20. PMID: 32571820; PMCID: PMC7449157.
- Mojica MF, Papp-Wallace KM, Taracila MA, Barnes MD, Rutter JD, Jacobs MR, LiPuma JJ, Walsh TJ, Vila AJ, Bonomo RA. Avibactam Restores the Susceptibility of Clinical Isolates of Stenotrophomonas maltophilia to Aztreonam. Antimicrob Agents Chemother. 2017 Sep 22;61(10):e00777-17. doi: 10.1128/AAC.00777-17. PMID: 28784669; PMCID: PMC5610502.
- Di Bonaventura G, Spedicato I, D’Antonio D, Robuffo I, Piccolomini R. Biofilm formation by Stenotrophomonas maltophilia: modulation by quinolones, trimethoprim-sulfamethoxazole, and ceftazidime. Antimicrob Agents Chemother. 2004 Jan;48(1):151-60. doi: 10.1128/aac.48.1.151-160.2004. PMID: 14693533; PMCID: PMC310151.
- Gopalakrishnan R, Hawley HB, Czachor JS, Markert RJ, Bernstein JM. Stenotrophomonas maltophilia infection and colonization in the intensive care units of two community hospitals: A study of 143 patients. Heart Lung. 1999 Mar-Apr;28(2):134-41. doi: 10.1053/hl.1999.v28.a96418. PMID: 10076113.
- Pathmanathan A, Waterer GW. Significance of positive Stenotrophomonas maltophilia culture in acute respiratory tract infection. Eur Respir J. 2005 May;25(5):911-4. doi: 10.1183/09031936.05.00096704. PMID: 15863651.
- Kwa AL, Low JG, Lim TP, Leow PC, Kurup A, Tam VH. Independent predictors for mortality in patients with positive Stenotrophomonas maltophilia cultures. Ann Acad Med Singap. 2008 Oct;37(10):826-30. PMID: 19037515.
- Saugel B, Eschermann K, Hoffmann R, Hapfelmeier A, Schultheiss C, Phillip V, Eyer F, Laugwitz KL, Schmid RM, Huber W. Stenotrophomonas maltophilia in the respiratory tract of medical intensive care unit patients. Eur J Clin Microbiol Infect Dis. 2012 Jul;31(7):1419-28. doi: 10.1007/s10096-011-1459-8. Epub 2011 Nov 7. PMID: 22057419.
- Velázquez-Acosta C, Zarco-Márquez S, Jiménez-Andrade MC, Volkow-Fernández P, Cornejo-Juárez P. Stenotrophomonas maltophilia bacteremia and pneumonia at a tertiary-care oncology center: a review of 16 years. Support Care Cancer. 2018 Jun;26(6):1953-1960. doi: 10.1007/s00520-017-4032-x. Epub 2018 Jan 7. PMID: 29307014.
- Xun M, Zhang Y, Li BL, Wu M, Zong Y, Yin YM. Clinical characteristics and risk factors of infections caused by Stenotrophomonas maltophilia in a hospital in northwest China. J Infect Dev Ctries. 2014 Aug 13;8(8):1000-5. doi: 10.3855/jidc.4236. PMID: 25116665.
- Guerci P, Bellut H, Mokhtari M, Gaudefroy J, Mongardon N, Charpentier C, Louis G, Tashk P, Dubost C, Ledochowski S, Kimmoun A, Godet T, Pottecher J, Lalot JM, Novy E, Hajage D, Bouglé A; AZUREA research network. Outcomes of Stenotrophomonas maltophilia hospital-acquired pneumonia in intensive care unit: a nationwide retrospective study. Crit Care. 2019 Nov 21;23(1):371. doi: 10.1186/s13054-019-2649-5. PMID: 31752976; PMCID: PMC6873544.
- Wang CH, Lin JC, Lin HA, Chang FY, Wang NC, Chiu SK, Lin TY, Yang YS, Kan LP, Yang CH, Chan MC, Yeh KM. Comparisons between patients with trimethoprim-sulfamethoxazole-susceptible and trimethoprim-sulfamethoxazole-resistant Stenotrophomonas maltophilia monomicrobial bacteremia: A 10-year retrospective study. J Microbiol Immunol Infect. 2016 Jun;49(3):378-86. doi: 10.1016/j.jmii.2014.06.005. Epub 2014 Jul 28. PMID: 25081988.
- Wang CH, Lin JC, Lin HA, Chang FY, Wang NC, Chiu SK, Lin TY, Yang YS, Kan LP, Yang CH, Chan MC, Yeh KM. Comparisons between patients with trimethoprim-sulfamethoxazole-susceptible and trimethoprim-sulfamethoxazole-resistant Stenotrophomonas maltophilia monomicrobial bacteremia: A 10-year retrospective study. J Microbiol Immunol Infect. 2016 Jun;49(3):378-86. doi: 10.1016/j.jmii.2014.06.005. Epub 2014 Jul 28. PMID: 25081988.
- Cho SY, Kang CI, Kim J, Ha YE, Chung DR, Lee NY, Peck KR, Song JH. Can levofloxacin be a useful alternative to trimethoprim-sulfamethoxazole for treating Stenotrophomonas maltophilia bacteremia? Antimicrob Agents Chemother. 2014;58(1):581-3. doi: 10.1128/AAC.01682-13. Epub 2013 Oct 14. PMID: 24126583; PMCID: PMC3910801.
- Wang YL, Scipione MR, Dubrovskaya Y, Papadopoulos J. Monotherapy with fluoroquinolone or trimethoprim-sulfamethoxazole for treatment of Stenotrophomonas maltophilia infections. Antimicrob Agents Chemother. 2014;58(1):176-82. doi: 10.1128/AAC.01324-13. Epub 2013 Oct 21. PMID: 24145530; PMCID: PMC3910778.
- Ko JH, Kang CI, Cornejo-Juárez P, Yeh KM, Wang CH, Cho SY, Gözel MG, Kim SH, Hsueh PR, Sekiya N, Matsumura Y, Lee DG, Cho SY, Shiratori S, Kim YJ, Chung DR, Peck KR. Fluoroquinolones versus trimethoprim-sulfamethoxazole for the treatment of Stenotrophomonas maltophilia infections: a systematic review and meta-analysis. Clin Microbiol Infect. 2019 May;25(5):546-554. doi: 10.1016/j.cmi.2018.11.008. Epub 2018 Nov 16. PMID: 30448331.
- Heyland DK, Dodek P, Muscedere J, Day A, Cook D; Canadian Critical Care Trials Group. Randomized trial of combination versus monotherapy for the empiric treatment of suspected ventilator-associated pneumonia. Crit Care Med. 2008 Mar;36(3):737-44. doi: 10.1097/01.CCM.0B013E31816203D6. PMID: 18091545.
- Tamma PD, Cosgrove SE, Maragakis LL. Combination therapy for treatment of infections with gram-negative bacteria. Clin Microbiol Rev. 2012 Jul;25(3):450-70. doi: 10.1128/CMR.05041-11. PMID: 22763634; PMCID: PMC3416487.
- Araoka H, Baba M, Okada C, Abe M, Kimura M, Yoneyama A. Evaluation of trimethoprim-sulfamethoxazole based combination therapy against Stenotrophomonas maltophilia: in vitro effects and clinical efficacy in cancer patients. Int J Infect Dis. 2017 May;58:18-21. doi: 10.1016/j.ijid.2017.02.020. Epub 2017 Feb 28. PMID: 28257816.
- Patrick Lake, PharmD, E. Yoko Furuya, MD, MS, Christine J. Kubin, PharmD BCPS (AQ-ID), Comparison of Monotherapy Versus Combination Therapy for Stenotrophomonas maltophilia Pneumonia Including Trimethoprim-Sulfamethoxazole-Containing and -Sparing Regimens, Open Forum Infectious Diseases, Volume 3, Issue suppl_1, December 2016, 2029, https://doi.org/10.1093/ofid/ofw172.1577
