This is a cross-sectional and longitudinal assessment of BD glucan levels in 146 patients living with HIV. Within this cohort, 53 had been diagnosed within 6 months, 22 had chronic HIV but no ART, and 71 had chronic HIV and were on ART. These were then compared to 42 uninfected controls. The study design is as follows:
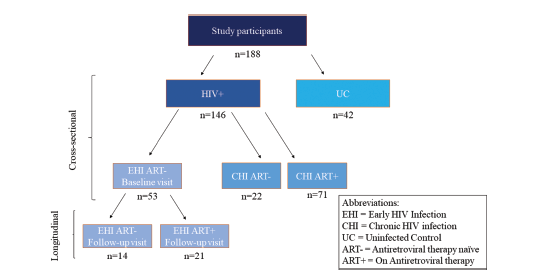
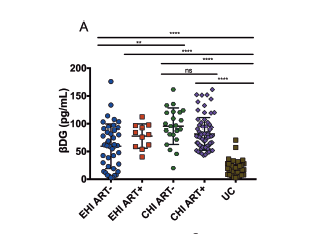
The cross-sectional assessment involved the chronic HIV with and without ART and the early onset HIV without ART. Those patients with newly diagnosed (within 6mo) were followed longitudinally to assess how ART affected BD glucan levels. In general, BD glucan levels were higher in early onset infection (67.9 +/- 40.7 pg/mL) and chronic infection (88.5 +/- 30.9 pg/mL) compared to uninfected controls (20.4 +/- 13.3 pg/mL, p-value <0.001). The values were independent of age, sex, CD4 and CD8 T cell counts. This was also independent of any STI. Notably, those with chronic HIV had higher levels than early HIV regardless of ART use:
Further, it seems that all ART did in the longitudinal group was to keep the BD glucan levels stable. This is compared to the group that did not start ART, whose lvel wen up from 47.8 +/- 33.8 pg/mL up to 55.8 +/- 41.9 pg/mL over a 24 month period (P- value 0.01). Further analysis show that the duration of infection PRIOR to starting ART was correlated ith BD glucan (r = 0.254 p -value 0.04).

Further, they also show weak correlation between beta-D glucan levels and gut mucosal damange, bacterial translocation, systemic immune translocation and other things you can take a look at. The interesting thing is the correlation between BD glucan and HIV progression:
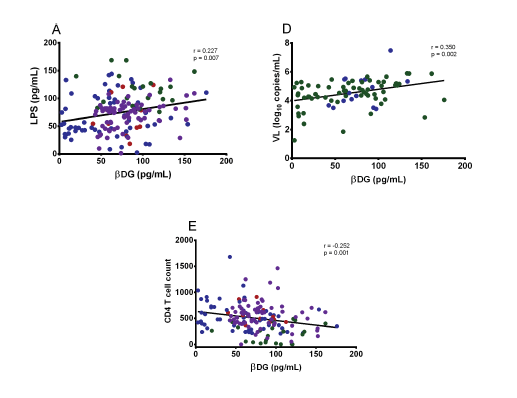
While the correlation is weak, it does exist and it may play a role in interpreting weak BD glucan levels in these patients i.e. BD glucan of like 90 when they have advanced AIDS and the ICU team gets all the test under the sun. I would feel relatively safe ignoring it, in context. It does beg the question of the same result in the neutropenic population, where we assume neutropenic fevers may occur in the context of “gut translocation.” Would they also have low levels of BD glucan hanging around?
Having said that, there are a few basic science papers suggesting that BD glucan may be opsonized by the complement pathway. How this plays a role in clinical medicine is unknown. Perhaps leukemoid reactions will lead to a false negative BD glucan by eating it all away??
Overview of (1→3)-β-D-glucan immunobiology. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2365860/
Front Immunol. 2013; 4: 230. Published online 2013 Aug 12. doi: 10.3389/fimmu.2013.00230 Binding of Soluble Yeast β-Glucan to Human Neutrophils and Monocytes is Complement-Dependent. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3740326/ Either way, these basic science papers hurt my brain
