
Retrospective study from South Korea evaluating the predictive value of BD glucan in the age of mold active triazole prophylaxis. They recruited patients that underwent induction chemotherapy, SCT, or GVHD treatment that had BD glucans throughout their stay while on posa or micafungin prophylaxis. They defined a positive BD glucan as 2 or more BDG results >80pg/mL. IFI were diagnosed per MSG criteria and they only counted proven or probable as positive IFIs. Clinicians were free to use BDG as they saw fit, diagnostic or for surveillance based on the situation.
In all 203 episodes from 155 patients were identified. The most common malignancy was AML (56.7%), followed by MM/amyloid (14.8%) and lymphoma (12.8%). Posaconazole was used 49.8% of the time, while micafungin was used for 50.2% of the time, with median time of PPx ~20 days. Most common indication for prophylaxis was induction chemo (43.8%), followed by auto SCT (26.1%) and allo SCT (23.6%).
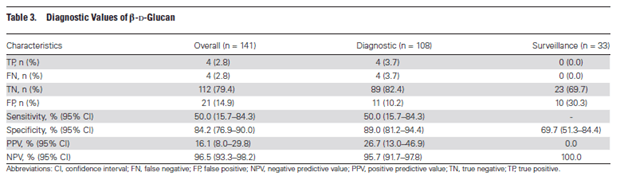
From the 141 episodes, they had 8 positive IFIs (5 aspergillus, 2 candida, 1 trichosporosis). 4 of these had positive BD glucan. They noted no crypto or Mucor in this study group. They calculated the NPV, PPV, sensitivity and specificity as such:
- Because it gives new readers context. What are you about? Why should they
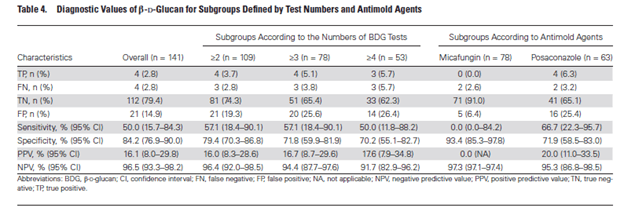
The post can be short or long, a personal intro to your life or a bloggy mission Breaking it down further by the number of BDG test and the type of agent used:
- Notably, there were a lot of false positives, 21 to be exact. They attributed this to either pip-tazo, meropenem, IVIG, or albumin but seems that albumin was the more likely to cause it.
Y

eSo BDG is not very good for surveillance is what I am getting here. IT is a reasonable diagnostic tool to throw in someone who has neutropenic fever that is not resolving with antibiotic therapy, however given the not great sensitivity, I do not think that any of us would even consider stopping antifungals even with a negative BD glucan. Certainly, it helps if you are looking for something and if its positive. The role of surveillance, however, its unclear. They defined “surveillance” as getting BD glucan in the absence of clinical evidence. SO they got it, just because? As far as the subgroup according to agent, think this is a statistical fluke, more than anything inherit to any agent specifically. Either way, I feel more confused with regards to BDG and its clinical utility.
