
Central lines are cool, for the most part. Except for when they’re infected. The pathophysiology behind these is explained in this diagram (1):
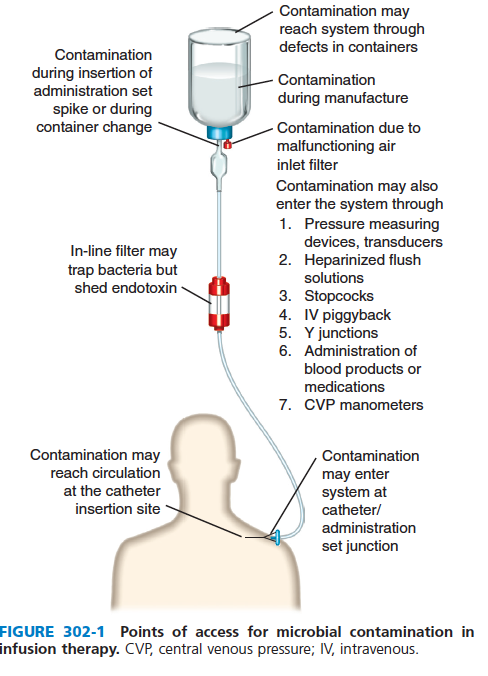
Microorganisms gain access to the extraluminal or intraluminal surface of the device. Both skin and hub may be the important entry point of organisms, with the development of biofilm contributing to their pathogenesis. There is, of course, a difference between catheter colonization and the catheter being the source of a bacteremia, but we will get into that a bit later. For now, I will focus on “relative” short term catheters i.e. not dialysis catheters and the diagnostics of line-associated infections, as well as the utility of antibiotic locks.
Diagnosis:
This is probably the trickiest subject to tackle, given the issues of colonization vs infection as well as the fact that in many patients, vascular access is a very difficult thing to obtain making folks a bit hesitant about culturing catheters and removing them. The IDSA guidelines suggest the following (2):
- For central venous catheters, the catheter tip should be cultured, rather than the subcutaneous segment. Growth of >15 CUFs from a 5-cm segment of catheter tip by roll-plate culture or >102 cuf from sonication culture reflects catheter colonization
- For suspected catheter-related bloodstream infection (CRBSI), paired blood samples, drawn from the catheter and a peripheral vein, should be cultured before initiation of antimicrobial therapy, and the bottles should be appropriately marked to reflect the site from which the samples were obtained
- A definitive diagnosis of CRSBI requires the same organism grow from at least one percutaneous blood culture and from a culture of the catheter tip OR that 2 blood samples be drawn (one peripheral, one catheter hub) that when cultured, meet CRSBI criteria for quantitative blood cultures or differential time to positivity (DTP).
- For quantitative blood cultures, a CFU obtained from the catheter hub that is at least 3-fold greater than the colony count from the peripheral vein best describes CRSBI
- For DTP, growth of microbes from the blood sample drawn from a catheter hub at least 2h before microbial growth detected from a blood sample obtained from a peripheral vein best describes a CRSBI
Ok a lot of things are going on there, but I think it’s best to look at where this data came from. While it may be reasonable to suspect that superficial erythema surrounding a catheter is suggestive of bacteremia, one prospective study of over 1000 patients with central catheters found that erythema, swelling, pain, and purulence at the insertion site had a low sensitivity at predicting blood-stream infection (3). Indeed, prevalence of inflammation was similar overall:

It seems one needs to culture the blood inside the catheter to get a diagnosis, then. One study (4) found that macroscopic debris was observed in 12 of 15 lines associated with proven bacteremia, yielding a sensitivity of 80%, however 14 out of 155 uninfected lines also had debris (specificity 91%). Moreover, while culture of the septum (i.e. the thing inside the port) had a higher sensitivity, paired cultures of the line with periphery still had higher sensitivity than culture of the tip:

Of course, this requires one to remove the catheter, which as we will see later may not be needed. So other methods have been employed for diagnosis. The most famous one being the “Maki method.” This method was evaluated in a study of 250 catheters (5). Here, the investigators evaluated a semiquantitative technique i.e. the roll-method. A colony count on agar of 15 or more colonies was associated with catheter site inflammation:

Moreover, of the 25 catheters that had >15 colonies, four catheters originated from patients with sepsis. These 25 catheters also had subsequent growth on culture medium:

Indeed, no patient who had less that 15 colonies of growth via the roll-plate method had catheter-related sepsis:

Other quantitative methods have been studied. One analysis evaluated 3 different methods (6):
- The Maki method, where the catheter tip was rolled back and forth across the surface of an agar plate, using a breakpoint of >15 cfu
- Sonication into a brain-heart broth
- Vortexing, both sonication and vortexing used a breakpoint of >100cfu/catheter segment
Overall, Maki’s method had the highest likelihood of detecting colonization when it went first by criterion A, which used the breakpoints as above:

The authors also recalculated the data using a breakpoint for sonication/vortexing of >1000cfu/catheter. For each method, the sensitivity/specificity/PPV/NPV were calculated, with all achieving fairly good sensitivity specificity across the board for both short-term and long-term catheters:

All three techniques were performed in all studied catheters, however which one came first was randomized. While useful, this still requires the removal of a line. What about culturing both the peripheral blood and the central line? Differential quantitative blood cultures (DBCs) were used in one study of ICU patients (7). Here, the cfu ratio of catheter/peripheral >1 was considered a positive DBC. 283 catheters were studied, and 19% had positive tip cultures via a quantitative method. Using a DBC threshold of 8, the sensitivity/specificity was 92.8%/98.8%.

In a cohort of 107 catheters in 64 patients, cultures drawn from a catheter that had a fourfold higher cfu than the simultaneously drawn peripheral culture had a sensitivity/specificity/PPV of 94%/100%/100% for line associated infection (8). Further, a single bacteria count >100cfu/ml from blood drawn from the catheter was highly predictive of line associated infection.
This is a better method; the idea being the inoculum of bacteria inside the catheter is much higher than that of the blood. If the source of the bacteremia is the catheter, then this is to be expected. Of course, this is still a quantitative method that may be a bit time consuming. What if we streamlined this idea? This is where the differential time to positivity (DPT) comes into play. The differential time to positivity has been defined as such: the blood culture drawn from the central venous catheter became positive at least 120 minutes earlier than a positive culture drawn simultaneously from a peripheral vein. The idea here is that if the catheter is the source of bacteremia, it should have a higher bacterial load than the peripheral blood and thus, turn positive faster. This was first evaluated in a retrospective study of 64 cases and found that the median DPT in catheter-related bacteremia was 427min compared to -15min in those where it was ruled out (9). A cut-off of 120min yielded a sensitivity and specificity of 96.4% and 100%, respectively:

This was further evaluated in a cohort of 438 patients with 817 catheters (10). 99 had suspected catheter-related infection, of which 93 were analyzed. The same microorganism was found in both peripheral/hub cultures in 28 out of 93 episodes, of which 17 were associated with bacteremic CRI. The remaining 11 patients who had bacteremia unrelated to the catheter had a median DTP of -15 minutes, meaning the peripheral blood turned positive 15min earlier than the catheter culture. Using a cut-off of +120min yielded a specificity/sensitivity of 91%/94%, and PPV/NPV of 94%/91%.

Similarly, another cohort of 191 pairs of blood cultures were analyzed and diagnosis of CR-BSI was made according to IDSA guidelines (11). When using a DTP of at least 120 minutes, the sensitivity was higher when compared to catheter tip-peripheral culture DTP:

The sensitivity was higher when catheters were left in place longer than 30 days:

A review also noted high sensitivity of DTP:

In candidemia, the optimal DTP was a bit different (12). A retrospective study of 177 simultaneous blood cultures positive for Candida spp found that those with catheter-related candidemia had significantly shorter DTP, usually a median of 8hrs:

A cutoff of >120min yielded a sensitivity/specificity of 85% and 82%. A cut-off of 120min had the highest sensitivity for C. albicans and C. tropicalis, but lowest for C. glabrata:

Indeed the optimal cutoff for C. glabrata based on ROC curve analysis was >6h.
A meta-analysis evaluated 8 methods of diagnosis, of which the highest specificity was achieved by the paired culture method, followed by line-drawn cultures via Q* (13):


Sensitivity and specificity was as follows, with the highest sensitivity being achieved by the IVD-drawn culture followed by the DPT:

What about catheters with multiple lumens? One study found that pooling blood from two to three lumes of the same catheter into a blood culture bottle yielded very similar results to individual lumen cultures (14):

Antibiotic Lock
The idea behind this is to salvage a colonized/infected catheter. By instilling a high concentration of antibiotic/disinfectant, one may be able to avoid the removal of catheters. Most of this data comes from observational and cohort data, however some randomized trials have been performed recently. One small observational study of 14 oncology patients with tunneled lines evaluated the usefulness of lock therapy in uncomplicated bacteremia (15). Here, only 2 catheters were removed, one due to relapse of methicillin-resistant CoNS bacteremia resistant to the antibiotic lock used, and another one due to polymicrobial bacteremia. A similar study evaluated 48 episodes of bacteremia occurring in the context of central venous catheters, excluding dialysis catheters (16). 19 episodes were treated with antibiotic-lock therapy + systemic antibiotics, while the rest were treated only with systemic antibiotics. Successful treatment was achieved in 84% of the lock therapy group compared to 65% of the standard of care group (p=0.27), though this did not reach statistical significance. When looking specifically at CoNS, 93% of the ALT group were cured compared to 79% of the standard of care group, again not reaching statistical significance (p= 0.36).
One randomized trial evaluated the use of antibiotic lock therapy, with the primary endpoint being failure to cure a central line related BSI (17). Only 46 patients were recruited, with failure to cure being higher in the placebo arm when compared to the antibiotic lock arm, though this did not reach statistical significance:

A retrospective study (18) evaluated the use of antibiotic lock therapy (third gen cephalosporin-beta-lactamase inhibitor, aminoglycoside or carbapenem for gram negative isolates, or vancomycin/teicoplanin for gram positive organisms). Dwell time was for 24hrs with lock being kept for 14 days. 224 patients undergoing HSCT were evaluated, with 91% of patients who were colonized clearing following the use of ALT. Amongst those who had catheter-related bacteremia, salvage with ALT was possible in 86.6% in those where it was used (13 out of 15 patients).
A minocycline-EDTA-Ethanol lock was used in a cohort of 30 oncology patients, which were compared to 60 patients whose lines were removed (19). Dwell time was 2hrs for a total of 7 doses. Most of the organisms were gram positives (Staph aureus 17%, CoNS 18%, Streptococcus 13%), followed by E.coli (~21%). While there was no difference in time to fever resolution, those who received the antibiotic lock were able to retain their catheters for a lot longer without any adverse events:

Moreover, mortality was not statistically different between groups:

Finally, a meta-analysis of 13 studies compared the use of prophylactic antibiotic locks containing either vancomycin or ethanol in adult and pediatric cancer patients (20). When looking at the adult population, the use of either type of prophylactic lock was associated with a reduced incidence of catheter-associated bacteremia, though the authors note there was a high degree of heterogeneity due to the different definitions used:

LINE REMOVAL:
When it comes to removal of a line, the guidelines state the following (2):
- Antibiotic lock therapy should be used for catheter salvage; however if antibiotic lock therapy cannot be used in this situation, systemic antibiotics should be administered through the colonized catheter.
- Long-term catheters (>30 days) should be removed with any of the following conditions: severe sepsis, suppurative thrombophlebitis, endocarditis, BSI that continues despite >72hrs of antibiotic therapy, or any of the following: S. aureus, P. aeruginosa, fungi, or mycobacteria.
- Short-term catheters should be removed from patients with CRSBI due to gram negative bacilli, S. aureus, enterococci, fungi, and mycobacteria.
- For catheters (both long and short term) with CRSBI due to less virulent organisms that are difficult to eradicate (Bacillus spp, MIcrococcus spp, Propionibacteria), catheters should generally be removed after blood culture contamination is ruled out.
- In uncomplicated CRSBI due to pathogens other than any of the above (including Micrococcus and P. acnes) in patients who require long-term access for survival (read: dialysis) treatment should be attempted without catheter removal with the use of systemic antibiotics and antibiotic lock therapy.
- If a patient has a single peripheral blood culture with CoNS, then get additional cultures one from the hub and another one from the periphery before removing line or starting antibiotics.
Indeed, failure to remove lines has been associated with worse outcomes, which was demonstrated in 2 cohort studies. A cohort of 300 patients with central catheters and gram negative bacteremia, multivariate analysis demonstrated that catheter removal within 2 days of bacteremia was associated with higher rates of microbiological resolution of infection as well as lower mortality at 3 months (21):

Another study of 124 patients (22) found that delayed catheter removal in gram negative bacteremia was associated with higher rate of persistent bacteremia (51% vs 18%, p= 0.01) and increased 30-day mortality (40% vs 12%, p =0.01). Delayed catheter removal was also found to be a risk factor for mortality in multivariate analysis:

Similarly, for enterococcus, a retrospective study (23) of 111 patients found that catheter retention was associated with higher in-hospital mortality (OR 3.19, 95% CI 1.21-9.26), along with VRE colonization (3.19, 95% CI 1.12-10.01). In another retrospective study of 430 patients with MDRO CLASBIs, 30-day mortality was higher in the cohort that did not have their catheter removed (24):

Furthermore, adjusted HR showed that not removing a line was associated with a 13 time higher risk of 30 day mortality:

And it should be no surprise when it comes to staph aureus. A small study of 55 patients (25) with catheter-related SAB found that mortality was higher amongst those who did not get their catheter removed within 48 hours (20% vs 5%), although this did not reach statistical significance, likely due to the small number of enrolled patients (p=0.18). Similarly, a single-center retrospective study (26) found that failure to remove intravascular device in SAB was associated with higher odds of relapse or death from reinfection (OR 6.5, 95% CI 2.1-20.2). In one study of nearly 400 patients with catheter-related SAB (27), time to removal of catheter (OR 1.13, 95% CI 1.06-1.21 per day), the presence of a permanent intravascular device (RR 2.85, 95% CI 1.49-5.48) were associated with higher instances of hematogenous complications.
This suggests that, if possible, lines should be removed. One randomized study evaluated a watchful waiting approach in a select number of patients in the ICU with central lines (28). Exclusion criteria included bacteremia with S. epidermidis, S, aureus, or candidemia and hemodynamically unstable patients. Removal of the venous catheter was done if there was worsening hemodynamics, bacteremia with the above organisms, or ongoing sepsis after 5 days. 64 patients were included, with all 38 lines in the standard of care group being removed compared to only 16 of 42 in the watchful waiting group. There was no difference in SOFA scores, duration of ICU stay, or mortality at the end of the study period:

This suggest that, at least in the ICU population, lines can be kept depending on the clinical stability and the type of organism.
TL;DR
- Diagnostics depend on both peripheral and line cultures, with a DTP of >120min suggesting a CLABSI.
- If you remove the line, the tip should be sent for culture, ideally by the Roll method
- For the most part, removal of the line should be attempted. If not feasible, antibiotic lock therapy can be done
References:
- [edited by] John E. Bennett, Raphael Dolin, Martin J. Blaser. (2015). Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. Philadelphia, PA :Elsevier/Saunders,
- Mermel LA, Allon M, Bouza E, Craven DE, Flynn P, O’Grady NP, Raad II, Rijnders BJ, Sherertz RJ, Warren DK. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2009 Jul 1;49(1):1-45. doi: 10.1086/599376. Erratum in: Clin Infect Dis. 2010 Apr 1;50(7):1079. Dosage error in article text. Erratum in: Clin Infect Dis. 2010 Feb 1;50(3):457. PMID: 19489710; PMCID: PMC4039170.
- Safdar N, Maki DG. Inflammation at the insertion site is not predictive of catheter-related bloodstream infection with short-term, noncuffed central venous catheters. Crit Care Med. 2002 Dec;30(12):2632-5. doi: 10.1097/00003246-200212000-00003. PMID: 12483050.
- Douard MC, Arlet G, Longuet P, Troje C, Rouveau M, Ponscarme D, Eurin B. Diagnosis of venous access port-related infections. Clin Infect Dis. 1999 Nov;29(5):1197-202. doi: 10.1086/313444. PMID: 10524963.
- Maki DG, Weise CE, Sarafin HW. A semiquantitative culture method for identifying intravenous-catheter-related infection. N Engl J Med. 1977 Jun 9;296(23):1305-9. doi: 10.1056/NEJM197706092962301. PMID: 323710.
- Bouza E, Alvarado N, Alcalá L, Sánchez-Conde M, Pérez MJ, Muñoz P, Martín-Rabadán P, Rodríguez-Créixems M. A prospective, randomized, and comparative study of 3 different methods for the diagnosis of intravascular catheter colonization. Clin Infect Dis. 2005 Apr 15;40(8):1096-100. doi: 10.1086/428576. Epub 2005 Mar 17. PMID: 15791507.
- Quilici N, Audibert G, Conroy MC, Bollaert PE, Guillemin F, Welfringer P, Garric J, Weber M, Laxenaire MC. Differential quantitative blood cultures in the diagnosis of catheter-related sepsis in intensive care units. Clin Infect Dis. 1997 Nov;25(5):1066-70. doi: 10.1086/516090. PMID: 9402359.
- Capdevila JA, Planes AM, Palomar M, Gasser I, Almirante B, Pahissa A, Crespo E, Martínez-Vázquez JM. Value of differential quantitative blood cultures in the diagnosis of catheter-related sepsis. Eur J Clin Microbiol Infect Dis. 1992 May;11(5):403-7. doi: 10.1007/BF01961854. PMID: 1425710.
- Blot F, Schmidt E, Nitenberg G, Tancrède C, Leclercq B, Laplanche A, Andremont A. Earlier positivity of central-venous- versus peripheral-blood cultures is highly predictive of catheter-related sepsis. J Clin Microbiol. 1998 Jan;36(1):105-9. doi: 10.1128/JCM.36.1.105-109.1998. PMID: 9431930; PMCID: PMC124817.
- Blot F, Nitenberg G, Chachaty E, Raynard B, Germann N, Antoun S, Laplanche A, Brun-Buisson C, Tancrède C. Diagnosis of catheter-related bacteraemia: a prospective comparison of the time to positivity of hub-blood versus peripheral-blood cultures. Lancet. 1999 Sep 25;354(9184):1071-7. doi: 10.1016/s0140-6736(98)11134-0. PMID: 10509498.
- Raad I, Hanna HA, Alakech B, Chatzinikolaou I, Johnson MM, Tarrand J. Differential time to positivity: a useful method for diagnosing catheter-related bloodstream infections. Ann Intern Med. 2004 Jan 6;140(1):18-25. doi: 10.7326/0003-4819-140-1-200401060-00007. PMID: 14706968.
- Park KH, Lee MS, Lee SO, Choi SH, Sung H, Kim MN, Kim YS, Woo JH, Kim SH. Diagnostic usefulness of differential time to positivity for catheter-related candidemia. J Clin Microbiol. 2014 Jul;52(7):2566-72. doi: 10.1128/JCM.00605-14. Epub 2014 May 14. PMID: 24829236; PMCID: PMC4097682.
- Safdar N, Fine JP, Maki DG. Meta-analysis: methods for diagnosing intravascular device-related bloodstream infection. Ann Intern Med. 2005 Mar 15;142(6):451-66. doi: 10.7326/0003-4819-142-6-200503150-00011. Erratum in: Ann Intern Med. 2005 May 3;142(9):803. PMID: 15767623.
- Herrera-Guerra AS, Garza-González E, Martínez-Resendez MF, Llaca-Díaz JM, Camacho-Ortiz A. Individual versus pooled multiple-lumen blood cultures for the diagnosis of intravascular catheter-related infections. Am J Infect Control. 2015 Jul 1;43(7):715-8. doi: 10.1016/j.ajic.2015.02.028. Epub 2015 Apr 11. PMID: 25868651.
- Sánchez-Muñoz A, Aguado JM, López-Martín A, López-Medrano F, Lumbreras C, Rodríguez FJ, Colomer R, Cortés-Funes H. Usefulness of antibiotic-lock technique in management of oncology patients with uncomplicated bacteremia related to tunneled catheters. Eur J Clin Microbiol Infect Dis. 2005 Apr;24(4):291-3. doi: 10.1007/s10096-005-1291-0. PMID: 15902539.
- Fortún J, Grill F, Martín-Dávila P, Blázquez J, Tato M, Sánchez-Corral J, García-San Miguel L, Moreno S. Treatment of long-term intravascular catheter-related bacteraemia with antibiotic-lock therapy. J Antimicrob Chemother. 2006 Oct;58(4):816-21. doi: 10.1093/jac/dkl318. Epub 2006 Aug 8. PMID: 16899468.
- Rijnders BJ, Van Wijngaerden E, Vandecasteele SJ, Stas M, Peetermans WE. Treatment of long-term intravascular catheter-related bacteraemia with antibiotic lock: randomized, placebo-controlled trial. J Antimicrob Chemother. 2005 Jan;55(1):90-4. doi: 10.1093/jac/dkh488. Epub 2004 Dec 1. PMID: 15574481
- Zanwar S, Jain P, Gokarn A, Devadas SK, Punatar S, Khurana S, Bonda A, Pruthy R, Bhat V, Qureshi S, Khattry N. Antibiotic lock therapy for salvage of tunneled central venous catheters with catheter colonization and catheter-related bloodstream infection. Transpl Infect Dis. 2019 Feb;21(1):e13017. doi: 10.1111/tid.13017. Epub 2018 Nov 19. PMID: 30369006.
- Raad I, Chaftari AM, Zakhour R, Jordan M, Al Hamal Z, Jiang Y, Yousif A, Garoge K, Mulanovich V, Viola GM, Kanj S, Pravinkumar E, Rosenblatt J, Hachem R. Successful Salvage of Central Venous Catheters in Patients with Catheter-Related or Central Line-Associated Bloodstream Infections by Using a Catheter Lock Solution Consisting of Minocycline, EDTA, and 25% Ethanol. Antimicrob Agents Chemother. 2016 May 23;60(6):3426-32. doi: 10.1128/AAC.02565-15. PMID: 27001822; PMCID: PMC4879419.
- Norris LB, Kablaoui F, Brilhart MK, Bookstaver PB. Systematic review of antimicrobial lock therapy for prevention of central-line-associated bloodstream infections in adult and pediatric cancer patients. Int J Antimicrob Agents. 2017 Sep;50(3):308-317. doi: 10.1016/j.ijantimicag.2017.06.013. Epub 2017 Jul 6. PMID: 28689878.
- Fares J, Khalil M, Chaftari AM, Hachem R, Jiang Y, Kantarjian HM, Raad II. Impact of Catheter Management on Clinical Outcome in Adult Cancer Patients With Gram-Negative Bacteremia. Open Forum Infect Dis. 2019 Sep 28;6(10):ofz357. doi: 10.1093/ofid/ofz357. PMID: 31660336; PMCID: PMC6765346.
- Lee YM, Moon C, Kim YJ, Lee HJ, Lee MS, Park KH. Clinical impact of delayed catheter removal for patients with central-venous-catheter-related Gram-negative bacteraemia. J Hosp Infect. 2018 May;99(1):106-113. doi: 10.1016/j.jhin.2018.01.004. Epub 2018 Jan 10. PMID: 29330016.
- Marschall J, Piccirillo ML, Fraser VJ, Doherty JA, Warren DK. Catheter removal versus retention in the management of catheter-associated enterococcal bloodstream infections. Can J Infect Dis Med Microbiol. 2013 Fall;24(3):e83-7. doi: 10.1155/2013/678503. PMID: 24421837; PMCID: PMC3852445.
- Burnham JP, Rojek RP, Kollef MH. Catheter removal and outcomes of multidrug-resistant central-line-associated bloodstream infection. Medicine (Baltimore). 2018 Oct;97(42):e12782. doi: 10.1097/MD.0000000000012782. PMID: 30334966; PMCID: PMC6211864.
- Malanoski GJ, Samore MH, Pefanis A, Karchmer AW. Staphylococcus aureus catheter-associated bacteremia. Minimal effective therapy and unusual infectious complications associated with arterial sheath catheters. Arch Intern Med. 1995 Jun 12;155(11):1161-6. doi: 10.1001/archinte.155.11.1161. PMID: 7763121.
- Fowler VG Jr, Sanders LL, Sexton DJ, Kong L, Marr KA, Gopal AK, Gottlieb G, McClelland RS, Corey GR. Outcome of Staphylococcus aureus bacteremia according to compliance with recommendations of infectious diseases specialists: experience with 244 patients. Clin Infect Dis. 1998 Sep;27(3):478-86. doi: 10.1086/514686. PMID: 9770144.
- Fowler VG Jr, Justice A, Moore C, Benjamin DK Jr, Woods CW, Campbell S, Reller LB, Corey GR, Day NP, Peacock SJ. Risk factors for hematogenous complications of intravascular catheter-associated Staphylococcus aureus bacteremia. Clin Infect Dis. 2005 Mar 1;40(5):695-703. doi: 10.1086/427806. Epub 2005 Feb 4. PMID: 15714415.
- Rijnders BJ, Peetermans WE, Verwaest C, Wilmer A, Van Wijngaerden E. Watchful waiting versus immediate catheter removal in ICU patients with suspected catheter-related infection: a randomized trial. Intensive Care Med. 2004 Jun;30(6):1073-80. doi: 10.1007/s00134-004-2212-x. Epub 2004 Mar 4. PMID: 14999442.
