
The cephalosporins are a class of beta-lactam antibiotics that is generally classified based on “generations.” These denote the spectrum of bacteria they target, with each successive generation having more gram negative coverage. I am convinced most people only know about ceftriaxone, the prototype third-generation cephalosporin aka an “extended-spectrum beta lactam” along with cefepime, which is the fourth-generation cephalosporin that targets pseudomonas. Most ID folks are aware of cefazolin, the first generation workhorse in MSSA infections. There is a second generation, which is not really known but has a quirk (1):
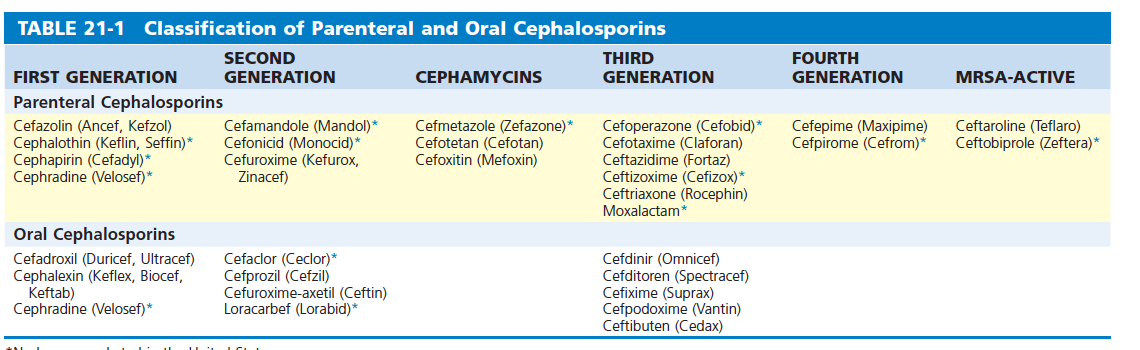
Grouped with the second generation cephalosporins are the cephamycins: cefoxitin and cefotetan. While they have lower activity against staphylococci, they actually do better against certain Enterobacter as well as Bacteroides spp. Indeed, these have been used as monotherapy in infections involving the abdomen and pelvis as well as gynecological infection.
Microbiology and In Vitro Data:
Cephamycin C was discovered as a product of Streptomyces and is closely related to the cephalosporin antibiotics produced by the filamentous fungi of the genus Cephalosporium (2). Hence, “cepha” and “myces” or “-mycin.” Both have the same core structure, however the cephamycins have a methoxyl group in place of the hydrogen group at the 7 position and are resistant to degradation by beta-lactamases:

One early in vitro study found that cephamycin C was active against salmonella and Proteus spp (3):

Another study evaluated 326 anaerobic isolates and compared the susceptibilities of different cephalosporins (4). Cefoxitin had the highest percentage of susceptible Bacteroides spp when compared to others such as cefazolin:

Cefoxitin was found to have a broad spectrum of activity to many important organisms, with the exception of E. faecalis, MRSA, and Pseudomonas (5):

A review of these agents found that cefoxitin, when compared to its parent compound cephamycin C, displayed a broader spectrum of activity (2):

Moreover, cefoxitin when compared to cephalothin (a first generation cephalosporin) had a broader spectrum of activity against most gram negatives as well as several strains of Bacteroides spp by disk-diffusion:

Of 362 cultures, cefoxitin retained activity against 76% of Bacteroides spp compared to only 19% Indeed, the cumulative percentage of susceptibility of Bacteroides spp was significantly higher for cefoxitin:

Given that cephamycins retained some activity against Bacteroides spp, one of the most important organisms in intra-abdominal infections, susceptibility to this organism is important in considering its use in said infections. An in vitro study found that cefotetan had the most activity against a selected strain of B. fragilis (6):


Despite these encouraging data, the rates of resistance seem to be going up for the cephamycins. In a multicenter study from 1990 to 1994, over 3100 isolates of Bacteroides were isolated (8). Resistance rates remained under 10% for all years for cefoxitin, however reached up to 22% for cefotetan:

Notably, however, piperacillin-tazobactam and metronidazole did not have any resistance. Similar findings were noted on the non-fragilis susceptibility trends:

961 Bacteroides spp were isolated from 1995 to 1996, with cefoxitin retaining some degree of activity for greater than 90% of isolates (9).

Notably, B. fragilis had the lowest rates of resistance next to B. vulgatus:

Cefotetan, however, had resistance rates nearly 40% for B. fragilis with significantly higher for other strains of Bacteroides spp.
Clinical Data:
You know me, I am more of a clinical guy so as long as there is some clinical data there may be some utility. Unfortunately, most of the data on cefoxitin tends to be fairly old and mostly focused on obstetrical and gynecological infections.
A retrospective study of 36 patients evaluated cefoxitin as monotherapy, with anaerobic bacteria isolated in 57% of infections (10). These typically ranged from skin and soft tissue infections to bacteremias. Cure was achieved in 71% of cases. Another retrospective study evaluated cefotetan in gynecological infections (11). 118 patients were evaluated, with cure being achieved in 99% of patients. Notably, however, N. gonorrhae was the most commonly isolated organism (39 isolates), followed by Streptococcus spp (34 isolates ), E. coli (24 isolates), S. agalactiae (23 isolates), and S. epidermidis (17 isolates).
A pair of multicenter studies published in the same paper evaluated either cefotetan with moxalactam in a 2:1 ratio or cefotetan and cefoxitin, also in a 2:1 ratio (12). There was no statistical difference in terms of clinical or bacteriological response amongst all agents:

While E. coli and streptococcus spp made up the majority of isolates, a not insignificant number of anaerobic organisms were isolated:

A similarly designed study (13) also found similar rates of clinical success (96% success for those treated with cefotetan, 97% for those treated with moxalactam for study I; 94% success for cefotetan and 91% for cefoxitin in study II). Only a total of 5 isolates amongst 335 subjects were isolated, however.
A multicenter trial compared cefotetan with cefoxitin in a randomized fashion in gynecological infections (14). 287 patients were enrolled, 189 assigned to cefotetan and 98 to cefoxitin. A large proportion of anaerobic organisms were isolated prior to therapy, including 30 spp of B. fragilis, 70 spp of B. bivius, and 117 spp of Peptostreptococcus. Overall, clinical response was similar between groups:

Unfortunately, there is not a lot of data when it comes to surgical patients. One of the only trials I was able to find was a randomized trial of patients with intra-abdominal infections (15). Cefotetan and cefoxitin were compared in a cohort of 188 patients, with with no statistical difference in outcomes between groups:

Rest of the data comes from their use in surgical prophylaxis to avoid surgical site infections. A retrospective analysis of 4331 patients who underwent colectomy used multivariate analysis and found that ciprofloxacin/metronidazole, cefazolin/metronidazole, and ertapenem when used as prophylaxis were associated with lower rates of surgical site infections (16):

A VA study involving 5750 colorectal surgeries (17) found that 53% of all written IV antibiotics were for cefoxitin (n = 3051). Multivariate backward stepwise generalized estimation equation analyses found that the use of cefoxitin and cefotetan was associated with higher risk of SSI:

The largest randomized trial of preoperative antibiotics compared a dose of ertapenem with a dose of cefotetan (18). In the mITT analysis, failure rate was higher in the cefotetan group (50.9% vs 40.2%, absolute difference -10.7%, 95% CI -17.1 to -4.2). This also held in the per protocol analysis (absolute difference -14.8%, 95% CI -21.9 to -7.5).
This is not a lot to go off on. The 2010 IDSA guidelines do list cefoxitin as a recommended single-agent therapy for mild to moderate intra-abdominal abscess (19):

Their rationale boils down to one sentence: “single agents approved for use include ticarcillin-clavulanate, cefoxitin, moxifloxacin, ertapenem, and tigecycline.” Not much to go off on. The surgical infection society revised guidelines (20) actually recommend against the use of cefoxitin as the only agent in these types of infections:
“ 4.4a. We suggest that cefoxitin and cefotetan not be used for the empiric treatment of adults and children with IAI (Grade 2-B).
Overall, given the lack of contemporary data and the potential for decreased efficacy of cephamycin antibiotic agents, as reflected in the indirect evidence from studies of colorectal surgical procedure prophylaxis, the task force suggests use of regimens other than cephamycins for empiric treatment of patients with IAI. It is recognized that this conflicts with a recent guideline on surgical prophylaxis, which recommends cephamycins for appendectomy and colorectal procedures [238]. Nevertheless, because there are alternative regimens for lower-risk patients with CA-IAI, the task force believes that these should be used preferentially to cephamycins.”
Which, given the above, seems reasonable. Bacteroides spp (at least some of them) are inhibited by cephamycins, but considering there is an alternative that has no resistance (read: metronidazole) using them as monotherapy when there is no robust data for surgical patients (which tend to be older and have more co-morbidities than many of the ob/gyn patients in the above studies) seems a bit odd.
References:
- [edited by] John E. Bennett, Raphael Dolin, Martin J. Blaser. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Philadelphia, PA :Elsevier/Saunders, 2015.
- Stapley EO, Birnbaum J, Miller AK, Wallick H, Hendlin D, Woodruff HB. Cefoxitin and cephamycins: microbiological studies. Rev Infect Dis. 1979 Jan-Feb;1(1):73-89. doi: 10.1093/clinids/1.1.73. PMID: 400941.
- Miller AK, Celozzi E, Pelak BA, Stapley EO, Hendlin D. Cephamycins, a new family of beta-lactam antibiotics. 3. In vitro studies. Antimicrob Agents Chemother. 1972 Oct;2(4):281-6. doi: 10.1128/AAC.2.4.281. PMID: 4670501; PMCID: PMC444307.
- Bach VT, Roy I, Thadepalli H. Susceptibility of anaerobic bacteria to cofoxitin and related compounds. Antimicrob Agents Chemother. 1977 May;11(5):912-3. doi: 10.1128/AAC.11.5.912. PMID: 879743; PMCID: PMC352096.
- Uri JV, Actor P, Guarini JR, Phillips L, Pitkin D, Demarinis RM, Weisbach JA. Biological and chemotherapeutic studies on three semisynthetic cephamycins. J Antibiot (Tokyo). 1978 Jan;31(1):82-91. doi: 10.7164/antibiotics.31.82. PMID: 627526.
- White RL, Kays MB, Friedrich LV, Del Bene VE. Impact of different statistical methodologies on the evaluation of the in-vitro MICs for Bacteroides fragilis of selected cephalosporins and cephamycins. J Antimicrob Chemother. 1993 Jan;31(1):57-64. doi: 10.1093/jac/31.1.57. PMID: 8444675.
- Aldridge KE, Weeks LS, Stratton CW, Sanders CV. Differences in the in vitro inhibitory and bactericidal activity of ceftizoxime, cefoxitin, cefotetan, and penicillin G against Bacteroides fragilis group isolates. Comparison of time-kill kinetic studies with MIC values. Diagn Microbiol Infect Dis. 1990 Jul-Aug;13(4):311-6. doi: 10.1016/0732-8893(90)90023-o. PMID: 2076592
- Snydman DR, McDermott L, Cuchural GJ Jr, Hecht DW, Iannini PB, Harrell LJ, Jenkins SG, O’Keefe JP, Pierson CL, Rihs JD, Yu VL, Finegold SM, Gorbach SL. Analysis of trends in antimicrobial resistance patterns among clinical isolates of Bacteroides fragilis group species from 1990 to 1994. Clin Infect Dis. 1996 Dec;23 Suppl 1:S54-65. doi: 10.1093/clinids/23.supplement_1.s54. PMID: 8953108.
- Snydman DR, Jacobus NV, McDermott LA, Supran S, Cuchural GJ Jr, Finegold S, Harrell L, Hecht DW, Iannini P, Jenkins S, Pierson C, Rihs J, Gorbach SL. Multicenter study of in vitro susceptibility of the Bacteroides fragilis group, 1995 to 1996, with comparison of resistance trends from 1990 to 1996. Antimicrob Agents Chemother. 1999 Oct;43(10):2417-22. doi: 10.1128/AAC.43.10.2417. PMID: 10508018; PMCID: PMC89494.
- Tally FP, Miao PV, O’Keefe JP, Gorbach SL. Cefoxitin therapy of anaerobic and aerobic infections. J Antimicrob Chemother. 1979 Jan;5(1):101-8. doi: 10.1093/jac/5.1.101. PMID: 761998.
- Poindexter AN 3rd, Sweet R, Ritter M. Cefotetan in the treatment of obstetric and gynecologic infections. Am J Obstet Gynecol. 1986 Apr;154(4):946-50. doi: 10.1016/0002-9378(86)90495-3. PMID: 3515949.
- Wilson SE, Boswick JA Jr, Duma RJ, Echols RM, Jemsek JG, Lerner R, Lewis RT, Najem AZ, Press RA, Rittenbury MS, et al. Cephalosporin therapy in intraabdominal infections. A multicenter randomized, comparative study of cefotetan, moxalactam, and cefoxitin. Am J Surg. 1988 May 31;155(5A):61-6. doi: 10.1016/s0002-9610(88)80215-0. PMID: 3287971.
- Sweet RL, Gall SA, Gibbs RS, Hemsell DL, Knuppel RA, Lane TW, Miller RD, Newton ER, Poindexter AN, Reguero W, et al. Multicenter clinical trials comparing cefotetan with moxalactam or cefoxitin as therapy for obstetric and gynecologic infections. Am J Surg. 1988 May 31;155(5A):56-60. doi: 10.1016/s0002-9610(88)80214-9. PMID: 3287970.
- Hemsell DL, Wendel GD, Gall SA, Newton ER, Gibbs RS, Knuppel RA, Lane TW, Sweet RL. Multicenter comparison of cefotetan and cefoxitin in the treatment of acute obstetric and gynecologic infections. Am J Obstet Gynecol. 1988 Mar;158(3 Pt 2):722-7. doi: 10.1016/s0002-9378(16)44535-7. PMID: 3281462.
- Lewis RT, Duma RJ, Echols RM, Jemsek JG, Najem AZ, Press RA, Stone HH, Ton GT, Wilson SE. Comparative study of cefotetan and cefoxitin in the treatment of intra-abdominal infections. Am J Obstet Gynecol. 1988 Mar;158(3 Pt 2):728-35. doi: 10.1016/s0002-9378(16)44536-9. Erratum in: Am J Obstet Gynecol 1989 Apr;160(4):1025. PMID: 3281463.
- Hendren S, Fritze D, Banerjee M, Kubus J, Cleary RK, Englesbe MJ, Campbell DA Jr. Antibiotic choice is independently associated with risk of surgical site infection after colectomy: a population-based cohort study. Ann Surg. 2013 Mar;257(3):469-75. doi: 10.1097/SLA.0b013e31826c4009. PMID: 23059498.
- Deierhoi RJ, Dawes LG, Vick C, Itani KM, Hawn MT. Choice of intravenous antibiotic prophylaxis for colorectal surgery does matter. J Am Coll Surg. 2013 Nov;217(5):763-9. doi: 10.1016/j.jamcollsurg.2013.07.003. Epub 2013 Sep 14. PMID: 24045142.
- Itani KM, Wilson SE, Awad SS, Jensen EH, Finn TS, Abramson MA. Ertapenem versus cefotetan prophylaxis in elective colorectal surgery. N Engl J Med. 2006 Dec 21;355(25):2640-51. doi: 10.1056/NEJMoa054408. PMID: 17182989.
- Solomkin JS, Mazuski JE, Bradley JS, Rodvold KA, Goldstein EJ, Baron EJ, O’Neill PJ, Chow AW, Dellinger EP, Eachempati SR, Gorbach S, Hilfiker M, May AK, Nathens AB, Sawyer RG, Bartlett JG. Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis. 2010 Jan 15;50(2):133-64. doi: 10.1086/649554. Erratum in: Clin Infect Dis. 2010 Jun 15;50(12):1695. Dosage error in article text. PMID: 20034345.
- Mazuski JE, Tessier JM, May AK, Sawyer RG, Nadler EP, Rosengart MR, Chang PK, O’Neill PJ, Mollen KP, Huston JM, Diaz JJ Jr, Prince JM. The Surgical Infection Society Revised Guidelines on the Management of Intra-Abdominal Infection. Surg Infect (Larchmt). 2017 Jan;18(1):1-76. doi: 10.1089/sur.2016.261. PMID: 28085573.
