
What is this? I am writing about a topic related to transplant infectious diseases? Something has to be going on! I had originally intended to write about CMV serostatus and risk of organ rejection in SOT patients, but that was a more difficult topic to tackle (just like that HTLV-1 post; yeah that one is on the shelf for now). As such, let’s talk about a simpler topic: CMV pneumonitis.
Given that anyone and everyone can be infected with CMV at any point in their lives, a few definitions are in order. CMV infection refers to the isolation of CMV virus or detection of viral products from any fluid, including plasma, serum, blood, CSF, or urine (1). The isolation of any viral product, however, does not imply pathology and in the absence of any symptoms, this would represent reactivation of latent infection. CMV syndrome, however, refers to the isolation of CMV along with fever and bone marrow suppression (defined as body temperature >38C for at least 2 days within a 3 day period in the absence of another etiology. The isolation of CMV from a body part in association with symptoms related to that body part represents a specific pathology. For the purposes of this post, CMV pneumonitis refers to the presence of signs and symptoms of pneumonia with CMV isolation from BAL, either by vial culture, immunohistochemistry analysis, or histopathological testing (1).
Why is the topic of CMV pneumonitis important? The overall mortality in the early days of transplantation was roughly 80% with it recently dropping to 30-50% with the advent of prophylaxis (2, 3). While I won’t discuss much in terms of pre-transplant risk factors, there are a few to know (2):
- Serological status of donor and recipient. It stands to reason if you have positive serology prior to transplant, your risk is higher. Interestingly, seronegative recipients who have a donor with positive serology have lower risk of CMV infection, which is the opposite in solid organ transplants
- Stem cell source: mismatched (MUD: mismatched unrelated donor) have a higher risk of disease.
- Conditioning: T-cell depletion or radiation plays a role
- Post-transplant complications, namely graft versus host disease.
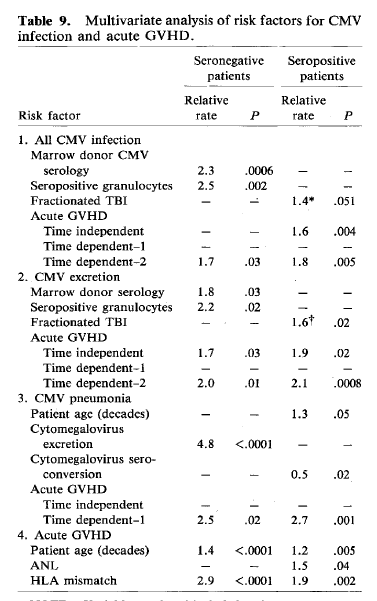
One of the older studies evaluated 545 patients, of which 16.7% had evidence of CMV pneumonia (4). Multivarite analysis found that seropositivity, older age, and acute GVHD were risk factors for CMV pneumonia. CMV excretion (aka CMV positivity off BAL without disease) was the only risk factor for those who were seronegative prior to transplantation:
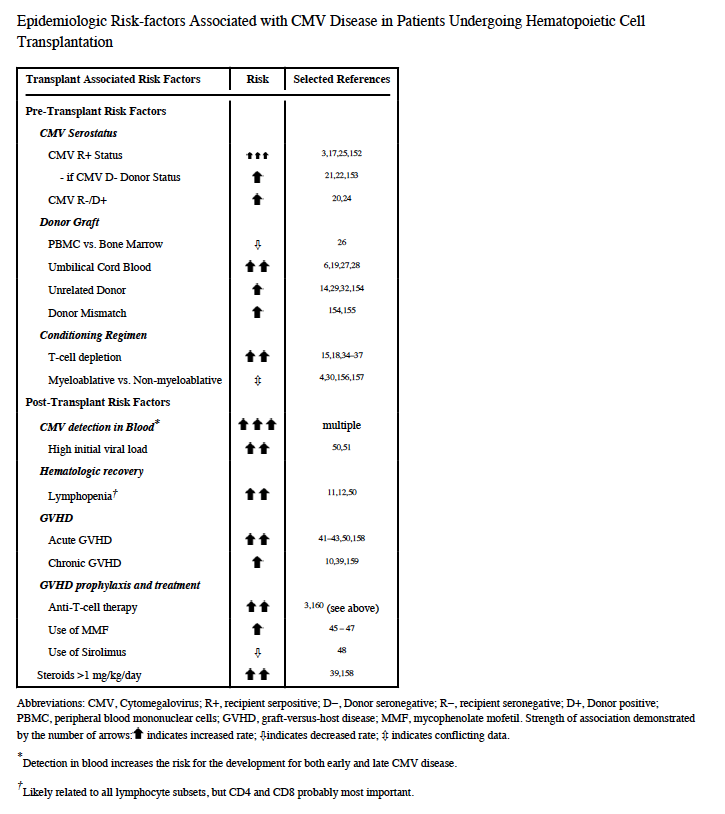
In a case-control autopsy study (5), CMV-risk factors included complete remission of hematological malignancy at diagnosis (60% vs 12%), sustained lymphopenia (55% vs 15%), and HSV co-infection (36% vs 6%). There was also a trend towards more CMV infections in those who received radiation therapy and cyclosporine, but this did not reach statistical significance. Reactivation has also been found to be correlated with risk of CMV pneumonitis. In one study, CMV reactivation after engraftment occurred more frequently in those with reduced intensity conditioning compared to myeloablative conditioning regions (53% in the reduced intensity vs 67% in the myeloablative cohort, p=0.046, 6). This held true only during the mid-recovery period with no difference in the late recovery period. One of the best tables on risk factors for CMV comes from a review by Travi and Pergam (2):
Not surprisingly, as it is with all things infectious disease, the symptoms tend to be very non-specific. One cohort (7) found that the most common symptoms were fever (94%), cough (63%), hypoxia (63%), and dyspnea (50%). On imaging, ground-glass opacities seems to be the most common radiological sign seen (66%), followed by multiple nodules in 59% and air-space consolidation in 59% (8). Overall, it seems that diffuse, ground-glass opacities were the predominant sign but these were non-specific.
Risk Factors for Mortality
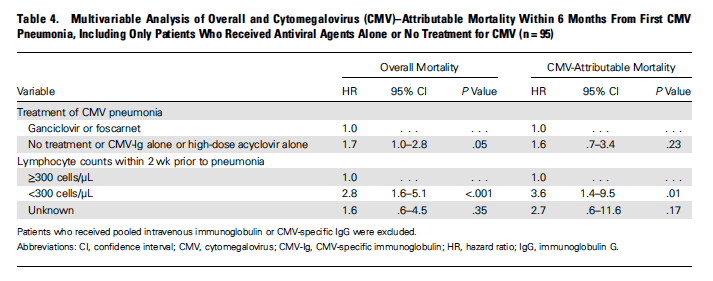
This tends to be somewhat simple, as people who are sick are more likely to die. For instance, a multivariate analysis from a retrospective study (3) found that female sex (HR 1.3, 95% CI 1.1-1.7), grade 3-4 GVHD (HR 1.4, 95% CI 1.1-1.7), lymphopenia within 2 weeks prior to pneumonia (HR 1.8, 95% CI 1.3-2.5), and mechanical ventilation (HR 3.1, 95% CI 2.4-3.9) were all associated with increased mortality. Therapy with ganciclovir, compared to no therapy, was associated with decreased overall mortality in univariate analysis (HR 1.9, 95% CI 1.2-3.2).
Similarly, a study of patients with lymphoma (9) found that an APACHE II score >16 (HR 15.5, 95% CI 1.5-163.7), admission to the ICU (univariate HR 9.21, 95% CI 1.88-45), and antiviral toxicity (HR 14.03, 95% CI 1.2-169.1) were also associated with higher mortality. Notably, combination therapy with IVIG or CMV Ig with ganciclovir was associated with improved outcomes (HR for mortality 0.19, 95% CI 0.03-0.95). Those with hematological malignancies and bone marrow transplantation seem to have higher risk for mortality when compared to those who received solid organ transplantation (7).
Diagnosis
This topic is kind of a crapshoot. In general, the isolation of CMV in conjunction with signs and symptoms of pneumonia suggest the diagnosis (2). Detection of CMV, however, can be a bit difficult. Secretion of CMV from lungs of seropositive patients is common and does not necessarily represent CMV pneumonia. This was confirmed in a retrospective study of 123 patients with allogeneic HSCT (10). In this cohort, CMV pneumonia was diagnosed only in 2 patients (1.6%), though CMV DNA was detected in 56 out of 144 BAL specimens (38.9%), with 49 patients having pneumonia due to another organism. Notably, 41 episodes of CMV BAL detection occurred in conjunction with CMV viremia. When looking at the etiology of pneumonia in the cohort in relatinoshi[p to the level of CMV DNA load, there was no statistical difference here:
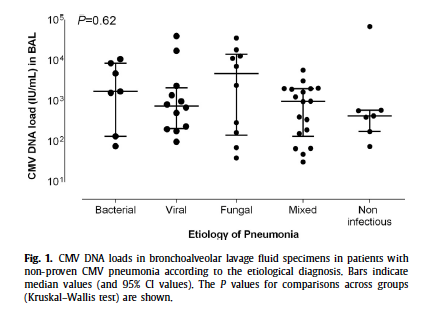
The median CMV DNA load in BAL specimens in those who did not have CMV pneumonia was 1210 IU/mL, which is a bit less than the 2 who were diagnosed with CMV pneumonia, 1453 and 12988 IU/mL. There was no statistical difference in terms of the level of CMV DNA off BAL in those who survived and those who died, though multivariate analysis found that a load >500 IU/mL was associated with increased mortality (HR 2.21, 95% CI 1.13-4.32).
BAL with viral culture, or histopathological evaluation is the standard for diagnosis. Faster methods, such as shell vial culture or DFA are also employed:
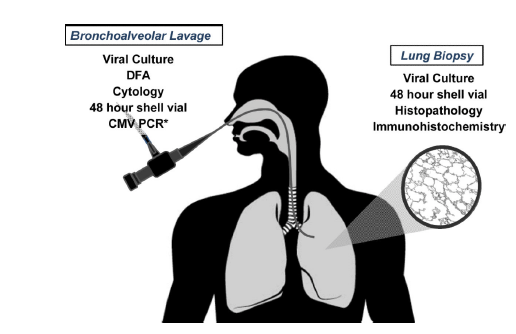
Given the invasive nature of things such as biopsy, as well as how long cytology and culture can take, PCR has been evaluated as another method of diagnosis. While definitions for proven CMV pneumonitis employ immunohistochemical staining on biopsy specimens (see below), this has not stopped people from attempting to use PCR as an alternative:

One thing to note from these studies is the fact that, while patients who do not have CMV pneumonitis can shed CMV from their lungs, their viral loads tend to be lower than those who do have illness. A retrospective study of 25 lung transplant patients found that those who were symptomatic had higher BAL and plasma CMV viral loads compared to those who were asymptomatic (11):

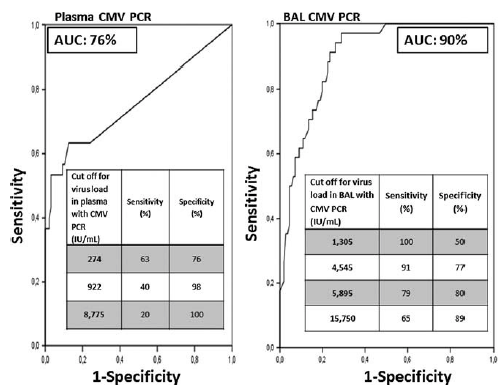
Similarly, in another study (12) that evaluated the correlation of CMV PCR with histopathology or immunohistochemistry, those who had CMV Pneumonia had higher viral loads compared to those without the diagnosis (32,940 IU/mL vs 1260 IU/mL, p <0.001). Further, plasma viral load was also higher in the pneumonia cohort (44,100 IU/mL vs 2340 IU/mL). Interestingly, when looking at those with proven vs probable pneumonia, those with proven pneumonia had higher BAL viral loads (90,000 vs 19,800) and plasma viral loads (67,000 vs 44,000). At a cutoff of 4545 IU/mL, BAL CMV PCR yielded a sensitivity and specificity of 91% and 77%, respectively:
A cohort of 132 HCT patients with CMV pneumonia were compared with 139 controls (100 with non-CMV pneumonia, 18 with idiopathic pulmonary syndrome, and 21 asymptomatic patients) to evaluate the threshold value for BAL CMV DNA-specific PCR for diagnosis (13). Samples also were compared to shell-vial culture and conventional culture. More patients with CMV pneumonia had PCR detection off BAL (99%) compared to the asymptomatic group with IPS (28%), asymptomatic group (57%) and the non-CMV pneumonia (32%). Further, PCR levels were significantly higher in the CMV pneumonia group:
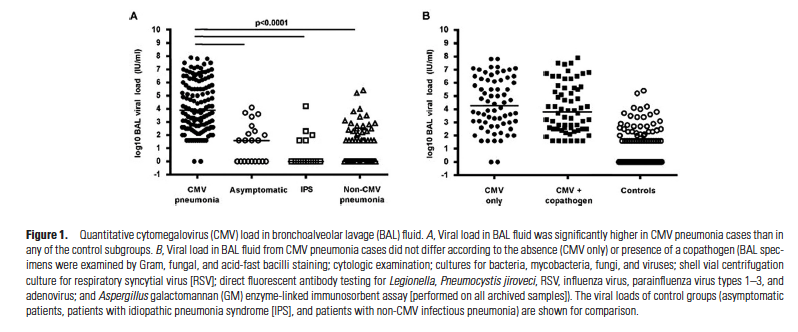
The presence of co-pathogens or blood did not affect the viral load. Using ROC curves and predictive models identified a cutoff of 500 IU/mL to differentiate between CMV pneumonia and pulmonary shedding. This model, however, assumed a prevalence of 10%, allowing the PPV to be 45% but the NPV to be >95% making it a good test to rule out CMV pneumonia. Here, 26% of those patients who have CMV pneumonia would be categorized as being pulmonary shedders.
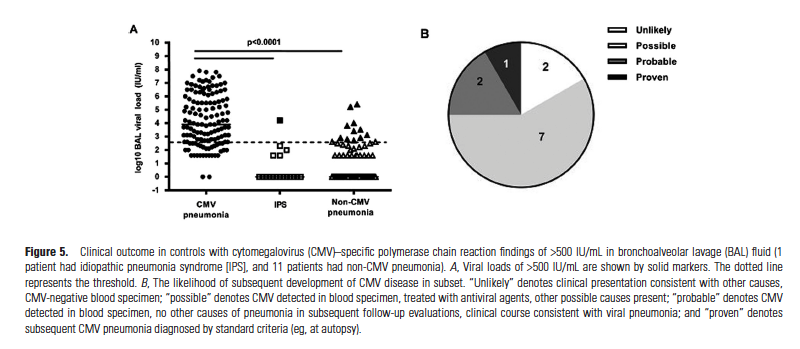
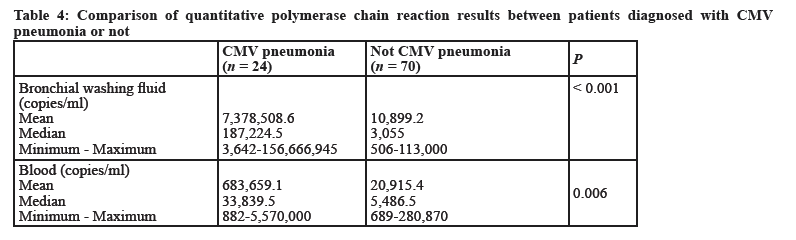
Note that, even those who had another etiology secreted CMV at a certain level, with some values being around those who were ultimately diagnosed. As noted above, this suggests that PCR can be used for ruling out CMV. Another cohort (14) found that 101 patients had a CMV PCR off their BAL >380 copies/mL, though only 24 of these were previously diagnosed with CMV pneumonia. Those who were ultimately diagnosed with CMV pneumonitis had higher mean values compared to those who were not diagnosed with pneumonitis:
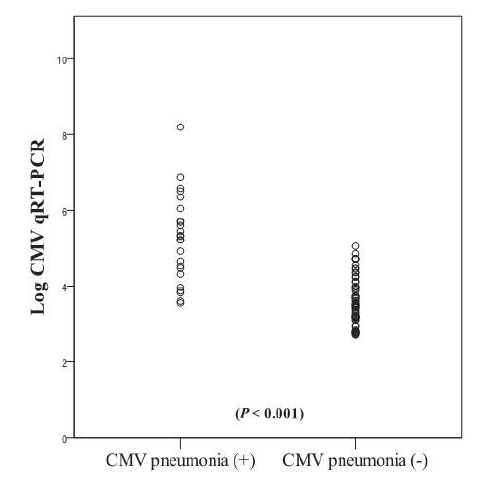
The relationship also held true when evaluating the bronchial washing fluid between the two cohorts, as well as peripheral blood:
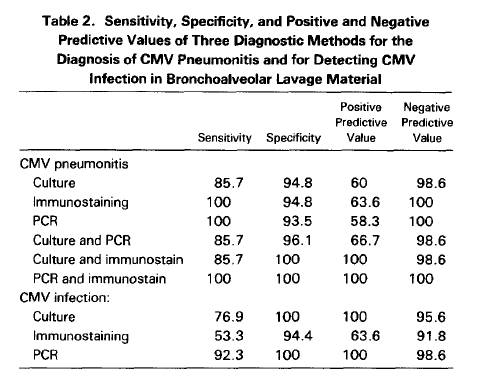
Using these values, the investigators used a ROC curve and found that the optimal point was 189,000 copies/mL (137,970 IU/mL; sensitivity 81.3% and specificity 81.4%) for post-BMT patients. Comparatively, those who had not undergone BMT had a higher inflection point, with a cutoff of 316,415 copies/mL (2,309,825 IU/mL) yielding a sensitivity of 100% but specificity of 63%. This last fact shouldn’t be surprising, as all people who have been infected with CMV in the past can have some degree of reactivation in severe illness. The combination of immunostaining/viral culture with PCR has been compared in another retrospective cohort study (15). Here, PCR by itself had a high sensitivity but low PPV when compared to other methods, however the combination of CPR and immunostain provided the greatest diagnostic utility:
There seems to be little diagnostic utility at this time when it comes to PCR, however the power of the test comes as a rule-out test, given its high negative predictive value. As seen above, those who have CMV pneumonitis have higher baseline copies off their BAL when compared to those who do not. In other words, if your pre-test probability of CMV pneumonitis is low, a PCR can be a good test to rule out CMV pneumonitis.
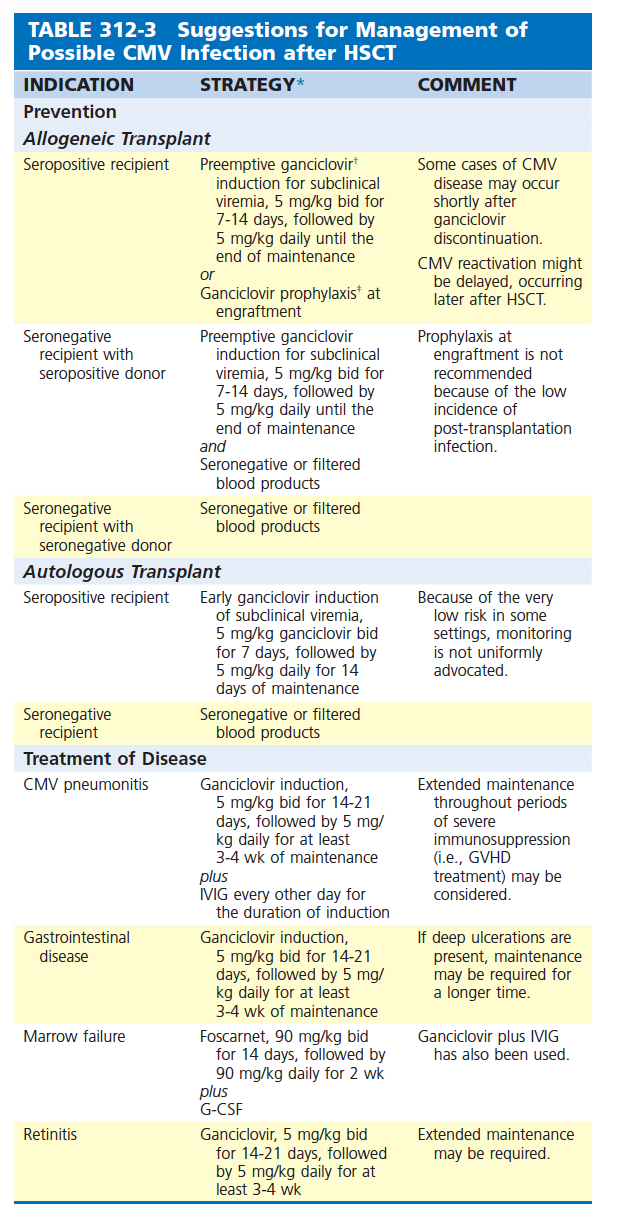
Therapy
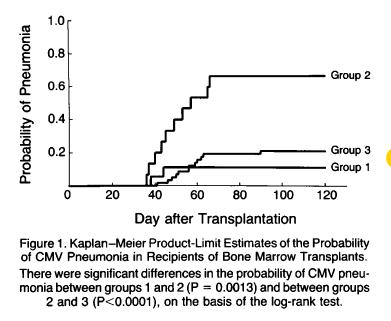
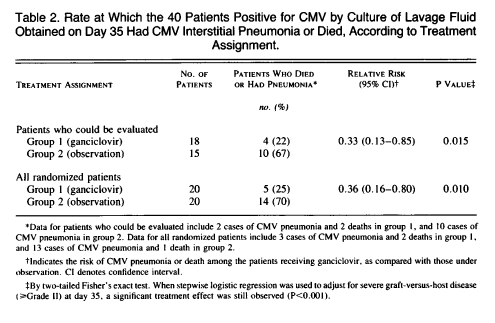
Therapy is generally done in two phases: a 2 week period of induction, usually with IV ganciclovir with intravenous immunoglobulin, followed by a 3-4 week period of maintenance, where valganciclovir is typically used. Early data on ganciclovir for its use on CMV pneumonitis suggested faster clearance of viremia (16) however a larger trial on its use for prophylaxis in HSCT patients with positive CMV serology supported its use in clinical scenarios (17). Patients who were positive for CMV via shell-vial cell culture or cytology on BAL were randomized to either prophylaxis or observation. 40 patients were included in randomization, with an additional 64 patients who were CMV negative off BAL. The risk of CMV pneumonia was significantly smaller in those who received prophylaxis compared to those who did not (group 1 vs group 2, respectively):
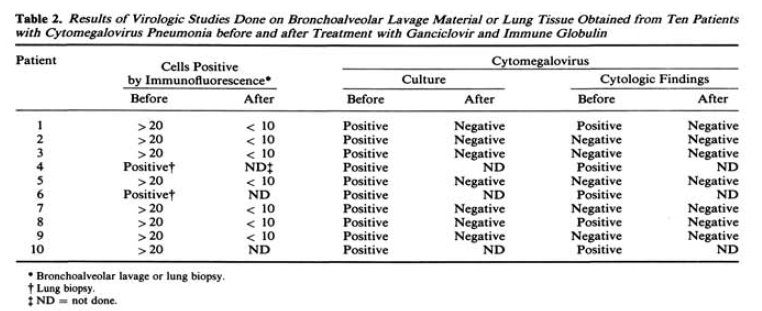
This question was explored in a multicenter, non-randomized study of 20 patients (18) where ganciclovir was given to these patients for 2 weeks. Here, only 8 patients survived to 90 days with an additional 2 surviving to 60 and 79 days. Notably, 3 of the 8 surviving patients had received CMV immunoglobulin, suggesting a possible effect of dual therapy. Since then, various non-controlled trials with either IVIG or other types of immune globulin have been undertaken. The combination of ganciclovir and high-dose IVIG was studied in 10 patients, where they were given 2.5 mg/kg ganciclovir TID for 20 days plus 500mg/kg IVIG every other day for 10 doses (19). These patients were compared to those who got ganciclovir alone, CMV hyperimmune globulin or IVIG alone. All 10 patients in the experimental group demonstrated improvement, with 8 being discharged within a month of starting therapy. When compared to the historical control group, all in the latter died from 2 to 42 days after starting therapy. BAL studies found that culture turned negative in 7/10 patients after therapy, did their cytological findings:
Another cohort of 25 BMT patients (20) with proven CMV pneumonitis evaluated IV ganciclovir and IV CMV immunoglobulin and found that 13/25 patients had survived the initial episode of pneumonia. Of these, 8 had improvement in oxygen saturation and 4 had recurrence based on pulmonary infiltrates and symptoms. Compared with other cohorts, survival was significantly better than the 15% previously reported. In an uncontrolled cohort of 13 patients (21), the combination of IVIG and ganciclovir given over 21 days resulted in clinical improvement in eleven patients with 9 surviving at the end of the study period.
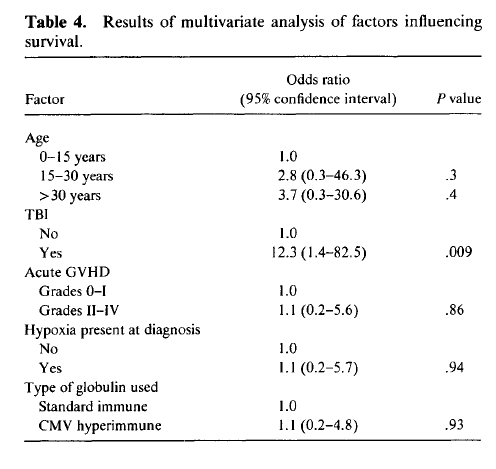
Despite the encouraging data on IVIG, not all data seems to suggest equal efficacy. In a cohort of 49 patients (22), several doses of ganciclovir were used (2.5mg/kg TID, 5mg/kg BID or daily), with half receiving standard IVIG and the other half receiving CMV-hyper immune IVIG. Survival was poor overall (35%). Multivariate analysis did not find any effect for CMV-specific immunoglobulin, with only the use of total body irradiation being associated with worse outcomes:
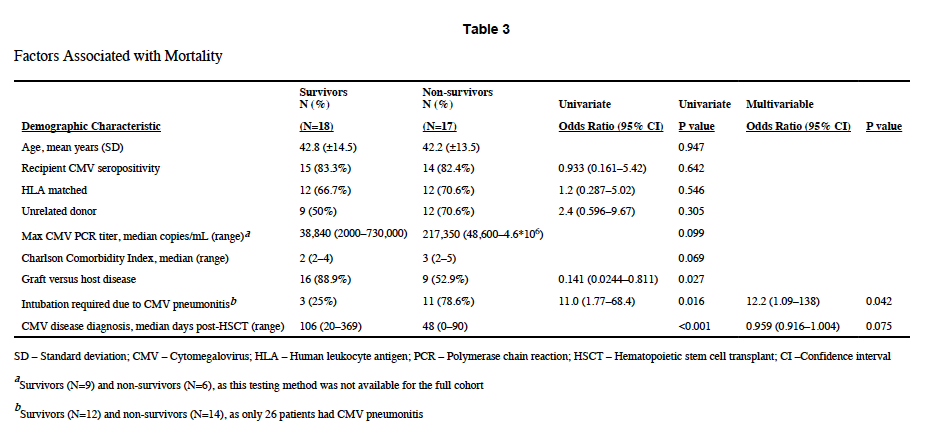
A single-center retrospective study (23) of 35 patients evaluated the combination of antivirals (ganciclovir 5mg/kg q12h or foascarnet 60mg/kg q8h) plus CMV-IVIG 150mg/kg every other day or twice weekly. All cause mortality was 49%, with it being 54% for those with pneumonitis. Multivariate analysis found that only intubation was associated with increased mortality for CMV pneumonitis, while CMV-IVIG was well tolerated in the cohort:
Despite the lack of randomized data, most texts continue to endorse therapy with ganciclovir or foscarnet with immunoglobulin or CMV-Ig (24, 25, 26) for at least 2 weeks followed by maintenance therapy. This is true in Mendell as well as the Taiwanese guidelines, however there is no robust data backing this up. Regardless, given the overall track record, combination therapy seems to be reasonable with both IVIG and Cytogam being equal all things considered (with IVIG being much cheaper than cytogam; I was unable to find any advantages of Cytogam over standard IVIG).
References:
- Ljungman P, Griffiths P, Paya C. Definitions of cytomegalovirus infection and disease in transplant recipients. Clin Infect Dis. 2002 Apr 15;34(8):1094-7. doi: 10.1086/339329. Epub 2002 Mar 11. PMID: 11914998.
- Travi G, Pergam SA. Cytomegalovirus pneumonia in hematopoietic stem cell recipients. J Intensive Care Med. 2014 Jul-Aug;29(4):200-12. doi: 10.1177/0885066613476454. Epub 2013 Feb 6. PMID: 23753231; PMCID: PMC3775875.
- Erard V, Guthrie KA, Seo S, Smith J, Huang M, Chien J, Flowers ME, Corey L, Boeckh M. Reduced Mortality of Cytomegalovirus Pneumonia After Hematopoietic Cell Transplantation Due to Antiviral Therapy and Changes in Transplantation Practices. Clin Infect Dis. 2015 Jul 1;61(1):31-9. doi: 10.1093/cid/civ215. Epub 2015 Mar 16. PMID: 25778751; PMCID: PMC4542910.
- Meyers JD, Flournoy N, Thomas ED. Risk factors for cytomegalovirus infection after human marrow transplantation. J Infect Dis. 1986 Mar;153(3):478-88. doi: 10.1093/infdis/153.3.478. PMID: 3005424.
- Torres HA, Aguilera E, Safdar A, Rohatgi N, Raad II, Sepulveda C, Luna M, Kontoyiannis DP, Chemaly RF. Fatal cytomegalovirus pneumonia in patients with haematological malignancies: an autopsy-based case-control study. Clin Microbiol Infect. 2008 Dec;14(12):1160-6. doi: 10.1111/j.1469-0691.2008.02106.x. Epub 2008 Nov 25. PMID: 19046167.
- Kim SH, Kee SY, Lee DG, Choi SM, Park SH, Kwon JC, Eom KS, Kim YJ, Kim HJ, Lee S, Min CK, Kim DW, Choi JH, Yoo JH, Lee JW, Min WS. Infectious complications following allogeneic stem cell transplantation: reduced-intensity vs. myeloablative conditioning regimens. Transpl Infect Dis. 2013 Feb;15(1):49-59. doi: 10.1111/tid.12003. Epub 2012 Sep 24. PMID: 22998745.
- Konoplev S, Champlin RE, Giralt S, Ueno NT, Khouri I, Raad I, Rolston K, Jacobson K, Tarrand J, Luna M, Nguyen Q, Whimbey E. Cytomegalovirus pneumonia in adult autologous blood and marrow transplant recipients. Bone Marrow Transplant. 2001 Apr;27(8):877-81. doi: 10.1038/sj.bmt.1702877. PMID: 11477447.
- Franquet T, Lee KS, Müller NL. Thin-section CT findings in 32 immunocompromised patients with cytomegalovirus pneumonia who do not have AIDS. AJR Am J Roentgenol. 2003 Oct;181(4):1059-63. doi: 10.2214/ajr.181.4.1811059. PMID: 14500230.
- Chemaly RF, Torres HA, Hachem RY, Nogueras GM, Aguilera EA, Younes A, Luna MA, Rodriguez G, Tarrand JJ, Raad II. Cytomegalovirus pneumonia in patients with lymphoma. Cancer. 2005 Sep 15;104(6):1213-20. doi: 10.1002/cncr.21294. PMID: 16078263.
- Piñana JL, Giménez E, Gómez MD, Pérez A, González EM, Vinuesa V, Hernández-Boluda JC, Montoro J, Salavert M, Tormo M, Amat P, Moles P, Carretero C, Balaguer-Roselló A, Sanz J, Sanz G, Solano C, Navarro D. Pulmonary cytomegalovirus (CMV) DNA shedding in allogeneic hematopoietic stem cell transplant recipients: Implications for the diagnosis of CMV pneumonia. J Infect. 2019 May;78(5):393-401. doi: 10.1016/j.jinf.2019.02.009. Epub 2019 Feb 21. PMID: 30797790; PMCID: PMC7126576.
- Bauer CC, Jaksch P, Aberle SW, Haber H, Lang G, Klepetko W, Hofmann H, Puchhammer-Stöckl E. Relationship between cytomegalovirus DNA load in epithelial lining fluid and plasma of lung transplant recipients and analysis of coinfection with Epstein-Barr virus and human herpesvirus 6 in the lung compartment. J Clin Microbiol. 2007 Feb;45(2):324-8. doi: 10.1128/JCM.01173-06. Epub 2006 Dec 6. PMID: 17151208; PMCID: PMC1829057.
- Lodding IP, Schultz HH, Jensen JU, Kirkby N, Perch M, Andersen C, Lundgren JD, Iversen M. Cytomegalovirus Viral Load in Bronchoalveolar Lavage to Diagnose Lung Transplant Associated CMV Pneumonia. Transplantation. 2018 Feb;102(2):326-332. doi: 10.1097/TP.0000000000001927. PMID: 28846557.
- Boeckh M, Stevens-Ayers T, Travi G, Huang ML, Cheng GS, Xie H, Leisenring W, Erard V, Seo S, Kimball L, Corey L, Pergam SA, Jerome KR. Cytomegalovirus (CMV) DNA Quantitation in Bronchoalveolar Lavage Fluid From Hematopoietic Stem Cell Transplant Recipients With CMV Pneumonia. J Infect Dis. 2017 May 15;215(10):1514-1522. doi: 10.1093/infdis/jix048. PMID: 28181657; PMCID: PMC5461426.
- Lee HY, Rhee CK, Choi JY, Lee HY, Lee JW, Lee DG. Diagnosis of cytomegalovirus pneumonia by quantitative polymerase chain reaction using bronchial washing fluid from patients with hematologic malignancies. Oncotarget. 2017 Jun 13;8(24):39736-39745. doi: 10.18632/oncotarget.14504. PMID: 28061469; PMCID: PMC5503648.
- Cathomas G, Morris P, Pekle K, Cunningham I, Emanuel D. Rapid diagnosis of cytomegalovirus pneumonia in marrow transplant recipients by bronchoalveolar lavage using the polymerase chain reaction, virus culture, and the direct immunostaining of alveolar cells. Blood. 1993 Apr 1;81(7):1909-14. PMID: 7681706.
- Shepp DH, Dandliker PS, de Miranda P, Burnette TC, Cederberg DM, Kirk LE, Meyers JD. Activity of 9-[2-hydroxy-1-(hydroxymethyl)ethoxymethyl]guanine in the treatment of cytomegalovirus pneumonia. Ann Intern Med. 1985 Sep;103(3):368-73. doi: 10.7326/0003-4819-103-3-368. PMID: 2992333.
- Schmidt GM, Horak DA, Niland JC, Duncan SR, Forman SJ, Zaia JA. A randomized, controlled trial of prophylactic ganciclovir for cytomegalovirus pulmonary infection in recipients of allogeneic bone marrow transplants; The City of Hope-Stanford-Syntex CMV Study Group. N Engl J Med. 1991 Apr 11;324(15):1005-11. doi: 10.1056/NEJM199104113241501. PMID: 1848679.
- Clyde Crumpacker, Steven Marlowe, Jai Lin Zhang, Steve Abrams, Paul Watkins, Treatment of Cytomegalovirus Pneumonia, Reviews of Infectious Diseases, Volume 10, Issue Supplement_3, July-August 1988, Pages S538–S546, https://doi.org/10.1093/clinids/10.Supplement_3.S538
- Emanuel D, Cunningham I, Jules-Elysee K, Brochstein JA, Kernan NA, Laver J, Stover D, White DA, Fels A, Polsky B, et al. Cytomegalovirus pneumonia after bone marrow transplantation successfully treated with the combination of ganciclovir and high-dose intravenous immune globulin. Ann Intern Med. 1988 Nov 15;109(10):777-82. doi: 10.7326/0003-4819-109-10-777. PMID: 2847609.
- Reed EC, Bowden RA, Dandliker PS, Lilleby KE, Meyers JD. Treatment of cytomegalovirus pneumonia with ganciclovir and intravenous cytomegalovirus immunoglobulin in patients with bone marrow transplants. Ann Intern Med. 1988 Nov 15;109(10):783-8. doi: 10.7326/0003-4819-109-10-783. PMID: 2847610.
- Schmidt GM, Kovacs A, Zaia JA, Horak DA, Blume KG, Nademanee AP, O’Donnell MR, Snyder DS, Forman SJ. Ganciclovir/immunoglobulin combination therapy for the treatment of human cytomegalovirus-associated interstitial pneumonia in bone marrow allograft recipients. Transplantation. 1988 Dec;46(6):905-7. PMID: 2849818.
- Ljungman P, Engelhard D, Link H, Biron P, Brandt L, Brunet S, Cordonnier C, Debusscher L, de Laurenzi A, Kolb HJ, et al. Treatment of interstitial pneumonitis due to cytomegalovirus with ganciclovir and intravenous immune globulin: experience of European Bone Marrow Transplant Group. Clin Infect Dis. 1992 Apr;14(4):831-5. doi: 10.1093/clinids/14.4.831. PMID: 1315585.
- Alexander BT, Hladnik LM, Augustin KM, Casabar E, McKinnon PS, Reichley RM, Ritchie DJ, Westervelt P, Dubberke ER. Use of cytomegalovirus intravenous immune globulin for the adjunctive treatment of cytomegalovirus in hematopoietic stem cell transplant recipients. Pharmacotherapy. 2010 Jun;30(6):554-61. doi: 10.1592/phco.30.6.554. PMID: 20500045; PMCID: PMC3668347.
- Jerry Teng CL, Wang PN, Chen YC, Ko BS. Cytomegalovirus management after allogeneic hematopoietic stem cell transplantation: A mini-review. J Microbiol Immunol Infect. 2021 Jun;54(3):341-348. doi: 10.1016/j.jmii.2021.01.001. Epub 2021 Jan 13. PMID: 33514495.
- Schulz U, Solidoro P, Müller V, Szabo A, Gottlieb J, Wilkens H, Enseleit F. CMV Immunoglobulins for the Treatment of CMV Infections in Thoracic Transplant Recipients. Transplantation. 2016 Mar;100 Suppl 3(Suppl 3):S5-10. doi: 10.1097/TP.0000000000001097. PMID: 26900992; PMCID: PMC4764017.
- [edited by] John E. Bennett, Raphael Dolin, Martin J. Blaser. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Philadelphia, PA :Elsevier/Saunders, 2015.
