Morgan DJ, Zhan M, Goto M, Franciscus C, Alexander B, Vaughan-Sarrazin M, Roghmann MC, Pineles L. The Effectiveness of Contact Precautions on Methicillin-Resistant Staphylococcus aureus in Long-term Care Across the United States. Clin Infect Dis. 2020 Oct 23;71(7):1676-1683. doi: 10.1093/cid/ciz1045. PMID: 31637429.
This was a cohort study of long-term VA facilities (aka the CLC) evaluating the efficacy of MRSA contact precautions compared to standard precautions (in other words, gowns/gloves vs standard hand hygiene). The authors evaluated a time period of 2011-2015, which included 2 years following implementation of a 2013 VA guidance that mandated the use of contact precautions in patients who were colonized with MRSA. Primary outcome was any positive culture or PCR test for MRSA in those who were previously negative for MRSA (patients who were positive for MRSA on admission to long-term facilities were excluded). During this period of time, the rate of acquisition of MRSA was 2.55/1000 patient days in the contact precaution vs 2.54/1000 in standard precautions. Notably, the presence of contact or standard precautions was not associated with increase incidence of MRSA colonization:
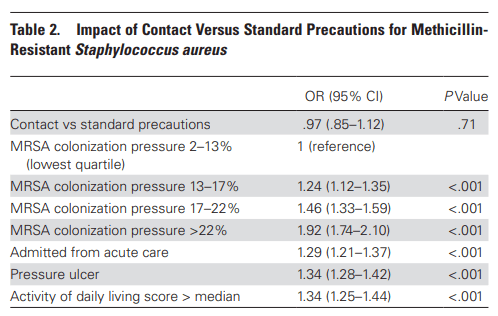
The authors posit this may be due to the fact that it may be difficult to adhere to contact precautions in long-term facilities, as patients tend to go outside of the rooms and interact with other patients in the common areas (if you have been to a CLC or any long-care facility, you know this is the case). This suggests that contact precautions may not be necessary in long-term facilities, though this study does not ask about acute care facilities (i.e. in-patient or ICU settings). As seen above, it seems that when around a fourth of the patients are already colonized, contact precautions may not be warranted.
Beydoun N, Tandon S, Krengel S, Johnson E, Palacio Bedoya F, Moore M, Refai D, Rouphael N. A Retrospective Chart Review on the Role of Suppressive Therapy in the Management of Spinal Infections Involving Hardware. Open Forum Infect Dis. 2020 Jun 25;7(7):ofaa253. doi: 10.1093/ofid/ofaa253. PMID: 32715019; PMCID: PMC7372706.
This study evaluated the association between the use of suppressive antibiotics and treatment success in complicated spinal infections that involved hardware, as well as evaluating patients who were more likely to be prescribed suppression antibiotics. In this retrospective chart review, patients wo had >4 weeks of antibiotics and had either infection in previously included hardware (group 1) or active infection leading to hardware replacement (group 2) were included. Primary outcome was treatment success (composite of survival, absence of additional surgery, no relapse). 124 patients met inclusion criteria, with 50 patients in group 1 and 74 in group 2. Logistic regression analysis found, surprisingly, that streptococcus, enterococcus, GNR, or polymicrobial infection was associated with less treatment success. Furthermore, longer initial antibiotic therapy was also inversely associated with treatment success.

Not surprisingly, however, those patients who had any type of Staph were more likely to have suppressive antibiotics (OR 2.11, 95% CI 1-4.46). One interesting finding was the fact that Strep and enterococcus accounted for a fourth of the early infections:

Moreover, early infection was inversely associated with hardware removal (OR 0.24, 95% CI 0.06-0.91) and infection with any staph species was associated with hardware removal, though this was not statistically significant. Notably here, the use of suppressive antibiotics was not associated with worse outcomes, and neither was hardware removal. While suppressive antibiotics were used across all groups, those who had an infection followed by hardware placement were more likely to receive >12mo of suppressive antibiotics. One of the surprising bits here was the relative high incidence of strep and enterococcus in early infection, though both MSSA and MRSA total are still the most prevalent infections early on. While there is no significant difference in the use of suppressive antibiotics and treatment success, foregoing this practice for either MSSA or MRSA is still a bit concerning, given its virulence, despite that around half of patients had either MSSA or MRSA. Probably not enough to not get me to give suppressive antibiotics when hardware is still present, especially in the spine.
van Wyk J, Ajana F, Bisshop F, De Wit S, Osiyemi O, Portilla Sogorb J, Routy JP, Wyen C, Ait-Khaled M, Nascimento MC, Pappa KA, Wang R, Wright J, Tenorio AR, Wynne B, Aboud M, Gartland MJ, Smith KY. Efficacy and Safety of Switching to Dolutegravir/Lamivudine Fixed-Dose 2-Drug Regimen vs Continuing a Tenofovir Alafenamide-Based 3- or 4-Drug Regimen for Maintenance of Virologic Suppression in Adults Living With Human Immunodeficiency Virus Type 1: Phase 3, Randomized, Noninferiority TANGO Study. Clin Infect Dis. 2020 Nov 5;71(8):1920-1929. doi: 10.1093/cid/ciz1243. PMID: 31905383; PMCID: PMC7643745.
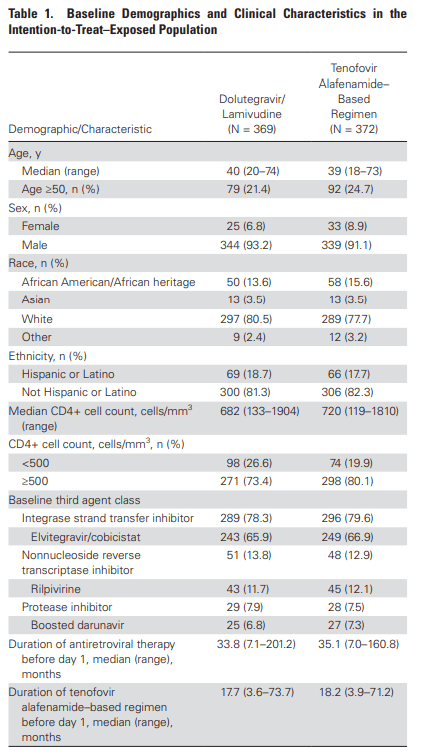
The past few years have seen the adoption of two-drug regimens for well controlled HIV infection. For instance, several studies such as the SWORD 1 and 2 and GEMINI 1 and 2 have shown that 2 drug regimens are non-inferior to 3 drug regimens. These, however, were switches from TDF-based regimens. The TANGO study (wee) was a phase 3, randomized, open label, noninferiority study evaluating DTG/3TC with a 3 or 4 drug TAF-based regimen in patients who were already suppressed. Patients who were suppressed for over 6 months or had a TDF to TAF switch within 3 months were enrolled. Patients were randomized in a 1:1 fashion, with primary outcome being the proportion of patients who had >50 copies/mL at week 48 in an ITT analysis. 371 patients were randomized to FTC/3TC while 371 were on the TAF-based regimen. Both groups were well balanced:
Based on a 4% non-inferiority margin, FTC/3TC was non-inferior toa TAF-based regimen:

In the per-protocol population, FTC/3TC had a similar proportion of patients to that of a TAF based regimen for HIV patients with VL <50 copies/mL.

Moreover, patients with an M184V/I mutation in both groups (4 in the study group, 3 in the TAF based group) all were virally suppressed through week 48. There were no significant changes in renal function (at least when using cystatin D as a surrogate rather than creatinine) between groups, though the study group did have a greater number of drug-related AE (12.2% vs 1.3%) though none of them lead to withdrawal (they mention one, which was by homicide, so not really related). These are encouraging results, though I am curious as to the long-term results for those with M184V/I mutations in dual-therapy regimens, as this regimen essentially leaves you with a one-drug regimen. At the end of the day, while it would be nice to have less drugs for well controlled patients to take, most of these combinations are a one pill-a-day combinations anyways. Maybe a ploy to get different combinations out there? Though this does challenge the notion that 3 drugs are the only way to go.
Reichler MR, Khan A, Yuan Y, Chen B, McAuley J, Mangura B, Sterling TR; Tuberculosis Epidemiologic Studies Consortium Task Order 2 Team. Duration of Exposure Among Close Contacts of Patients With Infectious Tuberculosis and Risk of Latent Tuberculosis Infection. Clin Infect Dis. 2020 Oct 23;71(7):1627-1634. doi: 10.1093/cid/ciz1044. PMID: 32044987.
This was an interesting one. This was a prospective study that included index TB patients and their contacts, who were interviewed to collect epidemiological information. This was a multicenter study with 9 health departments involved. Close contacts were defined as follows:
- People in household, social, workplace, or school settings
- Shared indoor space with someone with pulmonary TB for >15 hours per week for 1 or more weeks
- Total of >180hrs total
3040 close contacts had TST results available, of which 1390 (48%) were TST positive. The number of hours exposed was correlated with LTBI diagnoses in contacts, with a prevalence of 8.2% per 250 hours exposed:

Notably, there was no correlation for those who were exposed for less than 250 hours (OR 1.024, 95% CI 0.930-1.13), though there was a trend here. Multivariate analysis demonstrated that age >5, male sex, nonwhites, foreign origin, severe disease (positive smear or bilateral disease), household contacts and share bedroom with the index case were associated with LTBI in contacts:
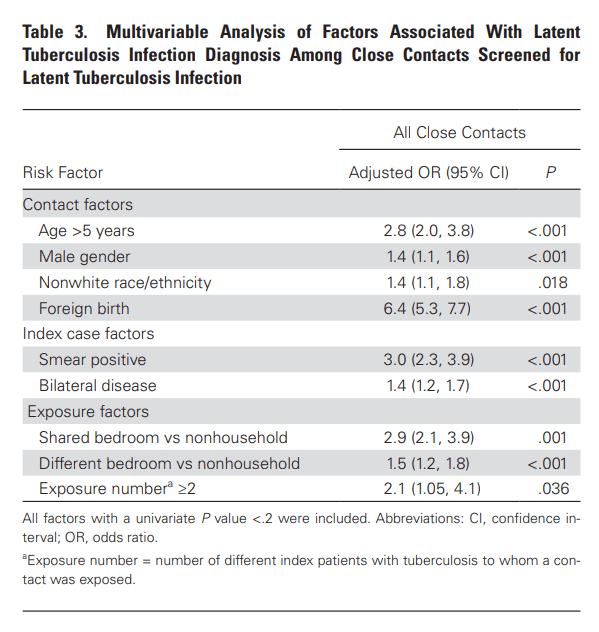
The authors note that non-US/Canadian birth was associated with increased likelihood of LTBI may have been in part due to BCG vaccine, though they do not think this is the only reason. So if you’re spending a lot of time with someone who is coughing up TB and has bad lungs on CT you’re likely going to seroconvert. Given physicians spend <5min with TB patients anyways, I do not think they’re at risk for seroconverting, unless they’re doing a bronch.
