
Blood cultures are the gold standard for evaluating patients with suspected bacteremia. They are an indispensable tool in evaluating diseases such as infective endocarditis, septic shock, meningitis, and pneumonia. By far, it is relatively simple to interpret the results (its either positive or negative) though whether it represents a clinically relevant entity or contamination is a bit more difficult. While their utility in terms of infections such as staphylococcal bacteremia or candidemia is inarguable, the utility of cultures in certain scenarios may not be warranted. Indeed, in some cases (17) the overall incidence of bacteremia is decreasing despite the higher numbers of ordered blood cultures.
Outpatient
The utility of blood cultures in the outpatient setting remains to be determined. For instance, in a cohort (1) of 3102 sets of blood cultures from outpatients only 2.4% (74) of the isolates were deemed to be significant. While patients with positive cultures were more likely to be admitted (RR 5.9, 95% CI 4.2 to 8.2, p-value <0.0001), the only factor associated with positive culture was age >50 (RR 1.6, 95% CI 1.3 to 2.1, p <0.01). In another prospective study (2) of febrile outpatients, 565 febrile patients were evaluated of which 210 were cultured and only 10 (4.8%) had positive blood cultures. When evaluating the frequency of positive cultures in those who were discharged from the ED, bacteremia was detected in only 0.8% vs 10.4% of those who were subsequently admitted. A retrospective study (3) evaluated the incidence of blood culture positivity in febrile patients coming in to the ED. Of 1350 ED patients, only 24 patients had true positive blood cultures (1.8%, 95% CI 1.1-2.5%), of which only 7 (0.52%) of all patients who had blood cultures had their management affected by it. Overall, blood cultures have a relatively low yield in all comers, suggesting a few things: 1) blood cultures in relative stable outpatients may not be necessary unless there is something in particular you are looking for (i.e. concern for endocarditis) and 2) in the vast majority of cases, it doesn’t change outcomes.
Inpatient and Follow Up Cultures
So outpatient blood cultures tend to be low yield. What about other bacteria or types of infections? A retrospective, multicenter study evaluated a large cohort of patients with community-onset bacteremia (4) with the goal evaluating risk factors for persistent bacteremia. A total of 1247 patients were evaluated, with bone and joint infection, vascular related infection, and IE having a higher percentage of positive follow up blood cultures:
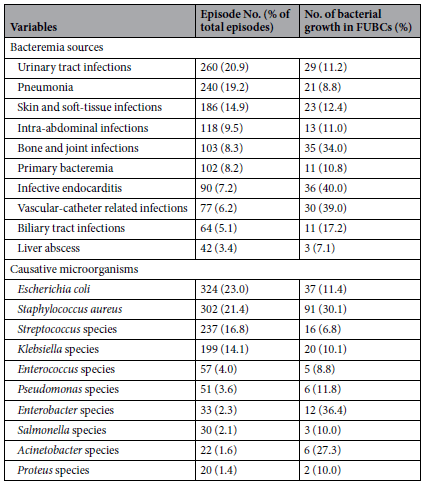
Notably, Staph aureus and Enterobacter were associated with a higher percentage of positive follow up blood culture. In multivariate analysis, follow up culture positivity at day 3-6 after antibiotic therapy was associated with increased OR for mortality (3.75, 95% CI 1.8-7.79). While this doesn’t give much of information about risk factors for follow up blood culture positivity, certain diseases jump out as warranting follow up cultures.
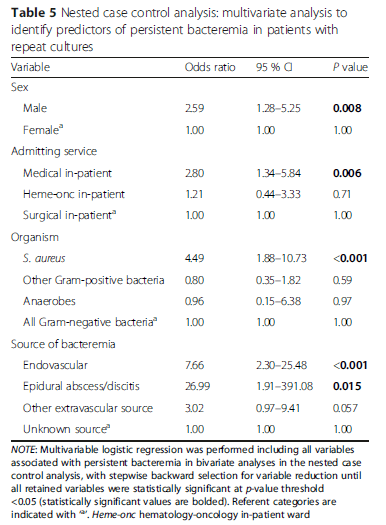
A better designed retrospective cohort study (5) evaluated the variables associated with persistent bacteremia. 1080 index bacteremias were evaluated, of which 118 had persistent bacteremia and were matched with 118 of the cleared bacteremias. The most common cause of persistent bacteremia was Staph aureus (44.9%) followed by Enterococcus (16.9%). Multivariate analysis associated with persistent bacteremia included male sex, Staph aureus, endovascular or epidural abscess as source:
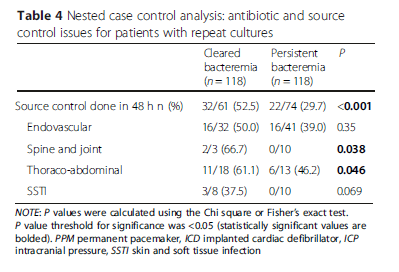
Further, when source control was done within 48hrs in thoraco-abdominal infections, or spine/joint infections, persistent bacteremia was not an issue (This did not apply to endovascular infections):
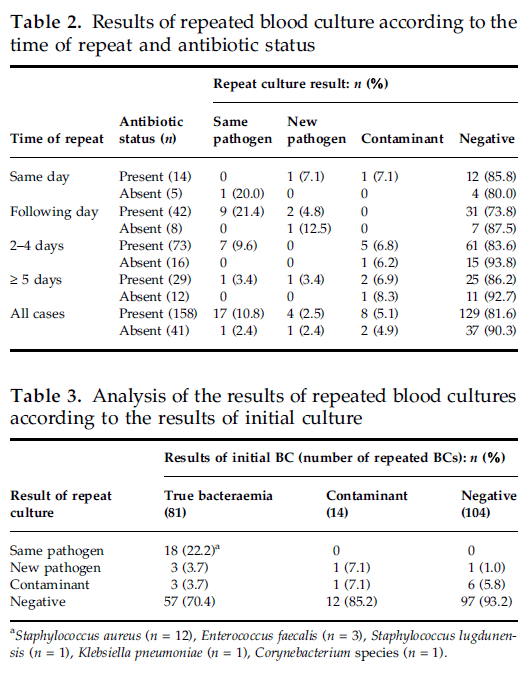
So repeat blood cultures may not be needed if you have a clear source and if that source is not a bone/joint or endovascular infection, or if the bacteria is staph aureus in most cases. Indeed, even in the inpatient setting outside of these scenario, repeat blood cultures are of low yield. For instance, in a retrospective (10) cohort 96 patients with repeat blood cultures were evaluated. Most of these (90.1%) had antibiotic prior to the repeat cultures, however the yield overall was low with 9.1% growing the same pathogen, 2.5% growing a new one, and 5% being contaminated:
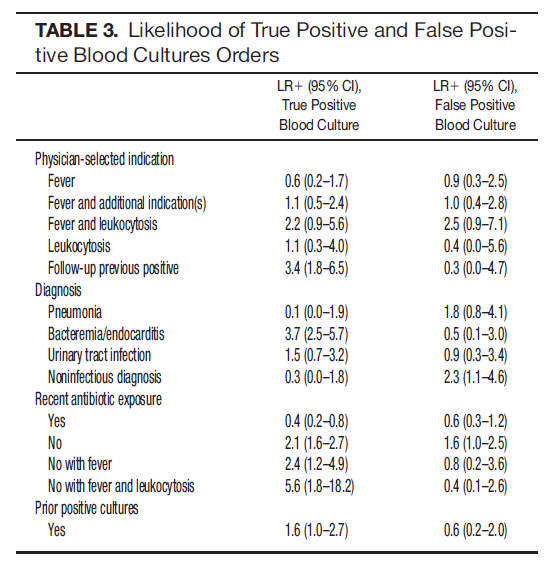
Are there any predictors for blood culture positivity in general? A prospective study evaluated the incidence of positive blood cultures in a VA system over a 7 month period (11) as well as predictive characteristics of patients for blood culture positivity. 576 blood cultures were ordered in 363 admitted patients, yielding a true positive rate of 3.6% (21/576) and false positive rate of 2.3% (13/576). Notably, fever by itself, fever with leukocytosis, and leukocytosis were not predictive of a positive blood culture. Infective endocarditis and fever, leukocytosis without prior antibiotic exposure were associated with blood culture positivity:
Suspected Bacteremia
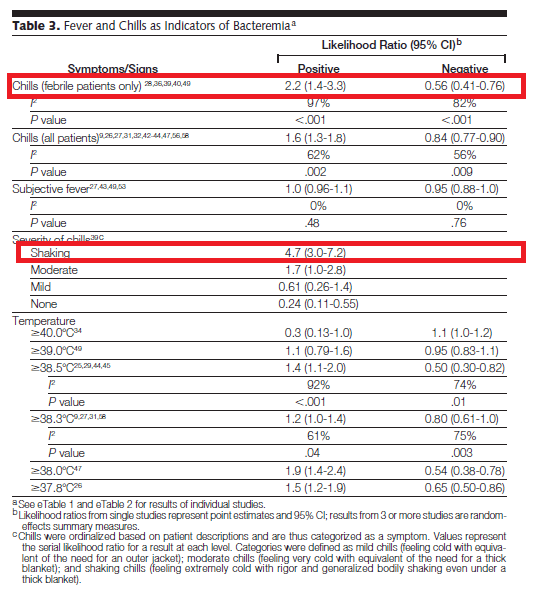
This tends to be a bit difficult, but in general it boils down to if a patient with fevers and possible sepsis require blood cultures to look for bacteremia. A review (6) evaluated clinical and laboratory findings and its correlation to suspected bacteremia. They included 4566 episodes of bacteremia and 25,946 control episodes. They found that shaking chills, irrespective of the presence of fevers, had the highest likelihood ratio when compared to fever at different cutoffs:
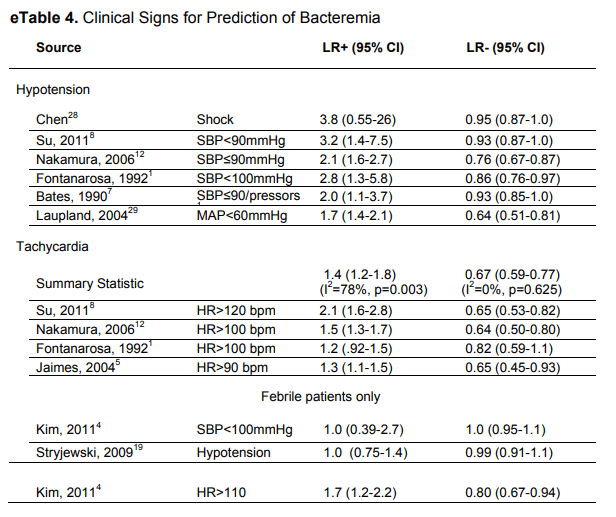
Tachycardia by itself was not terribly useful, but hypotension, especially in the context of shock, had a PLR of 3.8 but was not helpful if it was absent to rule out bacteremia:
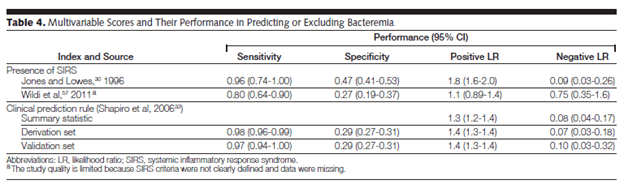
Similarly, the presence or absence of TCP and lymphocyte-neutrophil ratio had high positive likelihood ratio (1.6-2.1, and 2.1-2.6, respectively) but also high negative likelihood ratio (0.68 to 0.91, 0.36 to 0.76 respectively). Notably, the use of SIRS or a clinical predictor tool (including major criteria such as indwelling catheter, elevated temp >39.4, suspected endocarditis and minor criteria, such as chills, SBP <90, WBC >18k, Cr >2, thrombocytopenia, etc) had high sensitivity but poor specificity for bacteremia:
So not terribly helpful. If you have someone with several characteristics (i.e. they have SIRS), then blood cultures will be obtained typically. The one sign that is significantly associated with bacteremia is chills, specifically shaking chills or rigors. In a retrospective study evaluating 396 febrile patients coming in to the ED (7) found that age <65yo (OR 2.81, 95% CI 1.25-6.33), rigors (OR 13.7, 95% CI 4.47-42.0), chills (6.04, 95% CI 1.10-32.9), fever >39.9C (OR 2.68, 95% CI 1.03-6.94) were associated bacteremia. Another prospective study (8) evaluated the risk ratios for different degrees for chills in febrile patients. Shaking chills was found to have an aRR of 12.112:

Further, shaking chills had the highest specificity for bacteremia, but this was not terribly sensitive:

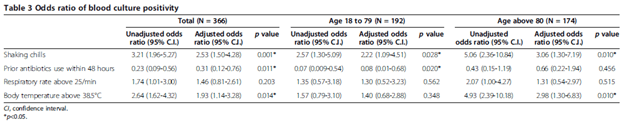
A retrospective study (9) found a more modest OR for elderly patients with shaking chills. 363 patients were evaluated, and shaking chills was found to have an aOR of 2.22 (95%CI 1.09-4.51) in those aged 18 to 79, which was higher in patients aged >80:
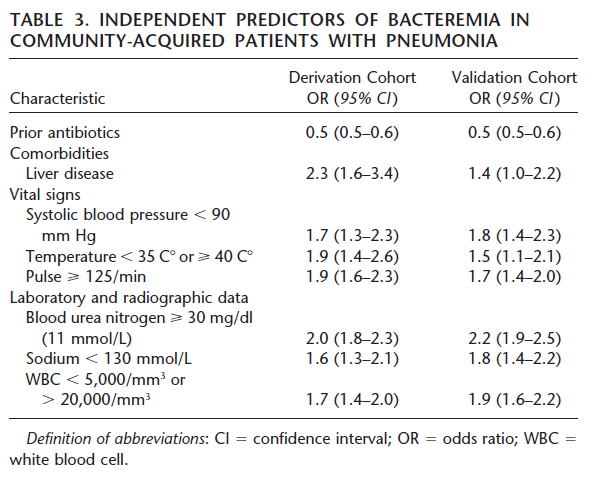
For pneumonia, a retrospective study (12) evaluated a prediction tool using a derivation cohort and a validation cohort. Liver disease, low blood pressure, fevers or hypothermia, tachycardia, hyponatremia and leukocytosis/leukopenia were associated with blood culture positivity in pneumonia:
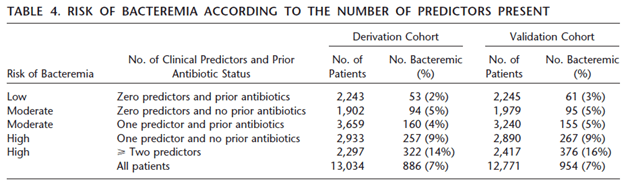
The rate of bacteremia in patients with CAP increased with at least one predictor and no prior antibiotics:
Despite these findings, however, afebrile patients can be bacteremic if they have CAP. In one retrospective study, the clinical characteristics of patients admitted with CAP (13). Bacteremia was identified in 190 of 2116 febrile patients (8.9%) while it was identified in 101 of 2149 afebrile patients (4.7%) and in in 1/23 hypothermic patients. Notably, patients with bacteremia were significantly older, and had higher CURB-65 score, with rates of bacteremia rising with higher CURB-65 score (from 3.5% with 0 points to 17.1% with 4 points).
All that to say, fevers and leukocytosis by themselves may not predict blood culture positivity, but shaking chills and multiple predictors for sickness (i.e. hypotension/shock, high CURB-65 in pneumonia patients, lack of prior antibiotics, elevated BUN, thrombocytopenia, and neutrophil:lymphocyte ratio >10) may increase the rate of positivity. In other words, if someone is sick, then they’re sick and they warrant blood cultures. Genius, I know.
Gram Negative Bacteremia
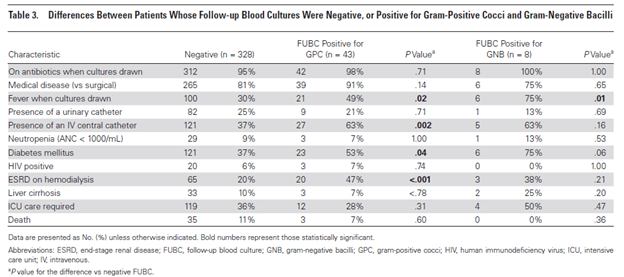
What about repeat blood cultures in gram negative bacteremia? This is still a contentious issue. For instance, a study (14) evaluated 500 episodes of bacteremia of which 383 had follow up blood cultures with 55 (14%) having positive results. Of these, only 8 (15%) were positive for gram negative rods. Overall, risk factors for repeat positive blood cultures were fevers when blood cultures were drawn, presence of a central line, or ESRD on iHD. For gram negative bacteremia, the only significant risk factor found was the presence of fever when the blood cultures were drawn:
Another retrospective study (15) evaluated 463 patients with gram negative bacteremia. 306 of these had follow up blood cultures and only 28 (9.2%) of the entire cohort had repeat positive blood cultures. Factors associated with positive follow up cultures included the presence of an intravascular device, ESRD on iHD, or an ESBL or carbapenemase producing organism:
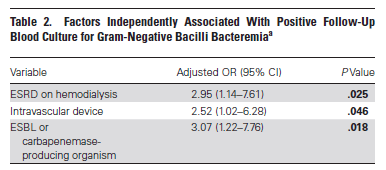
The presence of at least one risk factor increased the yield of a follow up blood culture from 3.3% to 14.8%.
For more specific organisms, a multi-center retrospective study (16) evaluated risk factors for persistent Klebsiella pneumonia bacteremia. Patients were matched in a 1:3 fashion for persistent and non-persistent bacteremia and risk factors were determined. Independent risk factors for persistent bacteremia included intra-abdominal infection, higher Charleston’s co-morbiditiy score, history of SOT, and unfavorable response to treatment on second day after initial blood culture (defined as positivity of at least 2 parameters, including fever, leukocytosis, or no decrease in CRP).
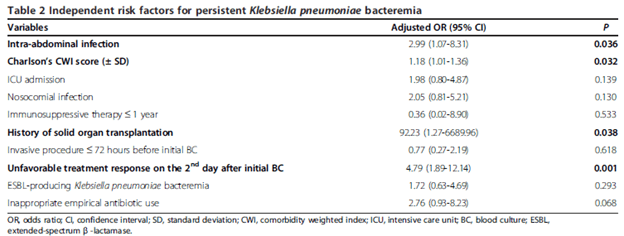
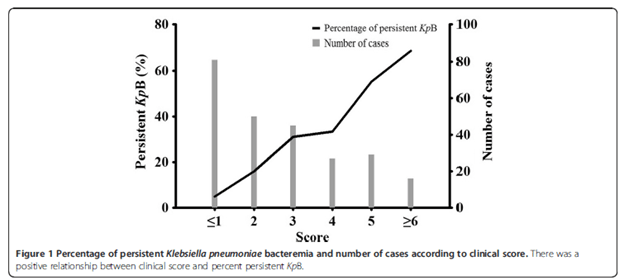
Notably, one could use these parameters (namely, intra-abdominal infection, nosocomial acquisition, fever, and lack of CRP decrease) with weighted scores of 1, 2, 3, and 2 to establish a score at which the risk of persistant bacteremia is present (using a cut off of >2, the sensitivity was 0.81 and specificity was 0.64):

So it may seem that as long as there are no risk factors for persistant bacteremia (MDRO, central catheters), there is no need for follow up blood cultures. Having said that, follow up cultures for gram negative bacteremia may have important prognostic consideration. For instance (18), follow up blood culture acquisition was associated with lower all cause in-hospital mortality (HR 0.629, 95% CI 0.511-0.722, p-value <0.0001) and attributable in-hospital mortality (HR 0.628, 95% CI 0.48-0.82, p-value 0.0007). Positive cultures were associated with an increased all-cause mortality (HR 2.099, 95% CI 1.567-2.811 p-value <0.0001) and attributable mortality (HR1.800, 95% CI 1.245-2.603, p-value 0.002).
References:
- Laupland KB, Church DL, Gregson DB. Blood cultures in ambulatory outpatients. BMC Infect Dis. 2005;5:35. Published 2005 May 17. doi:10.1186/1471-2334-5-35
- Eisenberg JM, Rose JD, Weinstein AJ. Routine blood cultures from febrile outpatients. Use in detecting bacteremia. JAMA. 1976;236(25):2863-2865.
- Sturmann KM, Bopp J, Molinari D, Akhtar S, Murphy J. Blood cultures in adult patients released from an urban emergency department: a 15-month experience. Acad Emerg Med. 1996;3(8):768-775. doi:10.1111/j.1553-2712.1996.tb03513.x
- Lee CC, Yang CY, Hsieh CC, et al. Timing of follow-up blood cultures for community-onset bacteremia. Sci Rep. 2019;9(1):14500. Published 2019 Oct 10. doi:10.1038/s41598-019-51032-z
- Wiggers JB, Xiong W, Daneman N. Sending repeat cultures: is there a role in the management of bacteremic episodes? (SCRIBE study). BMC Infect Dis. 2016;16:286. Published 2016 Jun 13. doi:10.1186/s12879-016-1622-z
- Coburn B, Morris AM, Tomlinson G, Detsky AS. Does this adult patient with suspected bacteremia require blood cultures? [published correction appears in JAMA. 2013 Jan 23;309(4):343]. JAMA. 2012;308(5):502-511. doi:10.1001/jama.2012.8262
- Lee CC, Wu CJ, Chi CH, et al. Prediction of community-onset bacteremia among febrile adults visiting an emergency department: rigor matters. Diagn Microbiol Infect Dis. 2012;73(2):168-173. doi:10.1016/j.diagmicrobio.2012.02.009
- Tokuda Y, Miyasato H, Stein GH, Kishaba T. The degree of chills for risk of bacteremia in acute febrile illness. Am J Med. 2005;118(12):1417. doi:10.1016/j.amjmed.2005.06.043
- Taniguchi T, Tsuha S, Takayama Y, Shiiki S. Shaking chills and high body temperature predict bacteremia especially among elderly patients. Springerplus. 2013;2:624. Published 2013 Nov 21. doi:10.1186/2193-1801-2-624
- Tabriz MS, Riederer K, Baran J Jr, Khatib R. Repeating blood cultures during hospital stay: practice pattern at a teaching hospital and a proposal for guidelines. Clin Microbiol Infect. 2004;10(7):624-627. doi:10.1111/j.1469-0691.2004.00893.x
- Linsenmeyer K, Gupta K, Strymish JM, Dhanani M, Brecher SM, Breu AC. Culture if spikes? Indications and yield of blood cultures in hospitalized medical patients. J Hosp Med. 2016;11(5):336-340. doi:10.1002/jhm.2541
- Metersky ML, Ma A, Bratzler DW, Houck PM. Predicting bacteremia in patients with community-acquired pneumonia. Am J Respir Crit Care Med. 2004;169(3):342-347. doi:10.1164/rccm.200309-1248OC
- Forstner C, Patchev V, Rohde G, et al. Rate and Predictors of Bacteremia in Afebrile Community-Acquired Pneumonia. Chest. 2020;157(3):529-539. doi:10.1016/j.chest.2019.10.006
- Canzoneri CN, Akhavan BJ, Tosur Z, Andrade PEA, Aisenberg GM. Follow-up Blood Cultures in Gram-Negative Bacteremia: Are They Needed?. Clin Infect Dis. 2017;65(11):1776-1779. doi:10.1093/cid/cix648
- Mitaka H, Gomez T, Lee YI, Perlman DC. Risk Factors for Positive Follow-Up Blood Cultures in Gram-Negative Bacilli Bacteremia: Implications for Selecting Who Needs Follow-Up Blood Cultures. Open Forum Infect Dis. 2020;7(4):ofaa110. Published 2020 Mar 28. doi:10.1093/ofid/ofaa110
- Kang CK, Kim ES, Song KH, et al. Can a routine follow-up blood culture be justified in Klebsiella pneumoniae bacteremia? A retrospective case-control study. BMC Infect Dis. 2013;13:365. Published 2013 Aug 2. doi:10.1186/1471-2334-13-365
- Nielsen SL. The incidence and prognosis of patients with bacteremia. Dan Med J. 2015;62(7):B5128.
- Maskarinec SA, Park LP, Ruffin F, et al. Positive follow-up blood cultures identify high mortality risk among patients with Gram-negative bacteraemia. Clin Microbiol Infect. 2020;26(7):904-910. doi:10.1016/j.cmi.2020.01.025
