
Over the past couple of weeks, vitamin D supplementation has been looked at as a potential therapy for COVID-19. Basic science data suggests that vitamin D has an immunomodulatory effects, such as upregulation of oxidative burst in activated macrophages in tuberculosis, or modulation of cytokine profiles that limits excessive production of pro-inflammatory cytokines in viral infections (1). Further, it may stimulate the expression of antimicrobial peptides such as the defensin retrocyclin-2. Due to this, there has been a push towards supplementing vitamin D to both treat and protect against viral respiratory infections.
Low vitamin D levels seem to be associated with higher incidence of respiratory tract infections. In a cross-sectional study (2), patients with serum 25 (OH) D levels <10 were found to have a higher incidence of URTI:

The effect of vitamin D seemed to decrease once controlling for other factors, but nevertheless was present in a multivariate model:

In other words, patients were 36% more likely to have a upper respiratory tract infection when their serum 25 (OH)D was <10 ng/mL. Not surprisingly, winter and fall seasons were found to have a correlation with increased upper respiratory tract infections. An interesting correlation, but didn’t necessarily imply causation.
This would suggest that supplementation would lead to decreased incidence of URTI. In a RCT comparing vitamin D3 supplementation (3), patients with frequent URTI were randomized to 12 months of vitamin D3 (4000IU/day) or placebo oil. Primary outcome was a composite of an infectious score based on a daily patient-reported questionnaire. 140 patients were randomized (70 to each group), and some of these had some sort of immunological disorder:

Overall, the vitamin D group had a statistically significant drop in their overall infection score. Notably, this did not actually have any clinically relevant information:
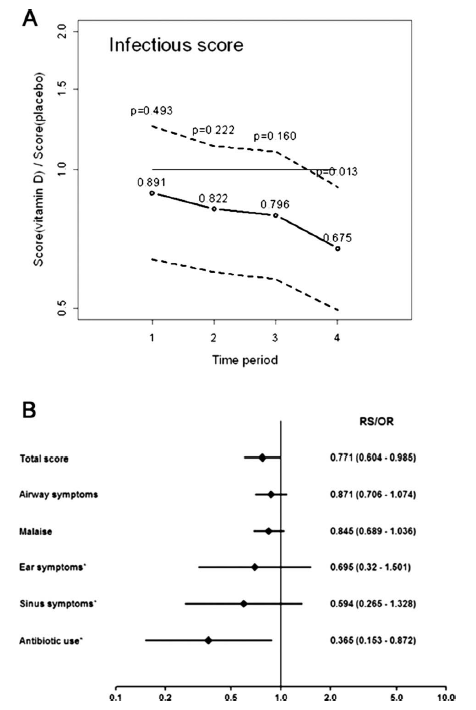
This seems to have been driven primarily by antibiotic use, though there was a trend towards the vitamin D group having less airway symptoms when compared to the placebo:

Notably, those who had vitamin D supplementation had lower incidence of positive bacterial cultures:

While not clinically significant, vitamin D supplementation in this population lead to lower antibiotic use and lower bacterial culture positivity. In a post-hoc analysis (4) evaluating the same data set, an RTI was more thoroughly defined as >/=2 points per day for at least 5 days, allowing this outcome to be dichotomized. Those in the vitamin D group had a significant lower fraction of one or more RTI (42% vs 63%, RR 0.64, 95% CI 0.43-0.94) as well as lower total number of RTIs, 62 in the vitamin D group vs 120 in the placebo group (p-value 0.05).

Two other RCTs evaluated vitamin D supplementation on children/adolescents and elderly adults. In a Vietnamese RCT in adolescent and children aged 3-7 (4), 1300 patients were randomized to receive either placebo or 14,000 IU/week of vitamin D weekly for 8 months. Primary outcome was RT-PCR positivity for influenza while secondary outcomes included RT-PCR positivity for other non-influenza infections. The vitamin D group had a 24% less chance of having any non-influenza viral infection when compared to the placebo group (HR 0.76 95% CI 0.61-0.94). There was no statistical difference between the vitamin D group and the placebo group for influenza, though:


Notably, the overall vitamin D levels upfront were not very different. In fact, only a small percentage had a vitamin D level <25:

While compelling, the positive result was a secondary outcome, which at best is hypothesis generating. Nevertheless, the results are intriguing.
Another RCT evaluating monthly vitamin D supplementation in older adults (5), aged 50-84 years old, involved 100,000 IU of vitamin D monthly following a 200,000 IU loading dose at the start vs placebo. This was part of the larger ViDA trial, of which the primary outcome was cardiovascular disease. Secondary outcomes were acute respiratory infections, specifically time to first reported ARI (a combination of URI and LRI events). 5110 patients were randomized and 5056 were analyzed. Overall, there was no difference in time to ARI in either group (74.7% in vitamin D group vs 73.7% in placebo group, aHR 1.01 95% CI 0.94-1.07):

There was a significant association in those whose vitamin D levels were <25 and risk of ARI, with an aHR of 1.21 in this group (95% CI 1.03-1.42). The authors speculate as to why the results were not significant and thing that more frequent dosing may mimic a more physiologic response that would confer health benefits. Another RCT from New Zealand (6) randomized 322 patients to either placebo or monthly vitamin D supplementation (200,000 IU load then 200,000 IU on month 1, then 100,000 IU monthly for 18 months total) with primary endpoint being number of URTI episodes. Overall, there was no difference in the number of URTI episodes between group (593 total in vitamin D vs 611 in placebo group), nor was there a difference in the median number of URTIs per person, or duration of symptoms:

They did not find any difference between URTI episodes when stratifying by vitamin D levels, however only 13 patients had levels <20ng/ml throughout the study. In a sub study (7) of a larger parent study on vitamin D and calcium supplementation and polyp prevention evaluated daily vitamin D on incidence of URI. 399 patients were randomized to receive 1000 IU/day of vitamin D and/or calcium carbonate (1200mg elemental calcium/day) and 360 received placebo. Patients were asked to fill out a questionnaire at the beginning and in the last 6 remaining months, they filled a “Colds and Flu” substudy health diaries. There were no differences between treatment groups in episodes of URTI (RR 0.93, 95% CI 0.79-1.09), cold (RR 0.93, 95% CI 0.78-1.10), or flu-like illness (RR 0.95, 95% CI 0.62-1.46). Further, there were no differences seen in those who had low mean levels of vitamin D at enrollment:

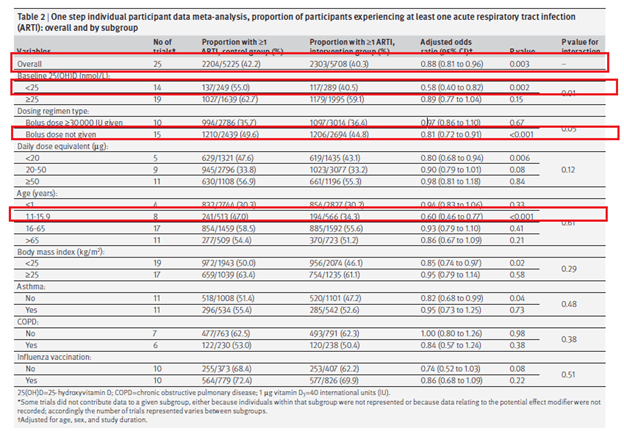
Finally, the largest meta-analysis in the subject (8) evaluated 25 RCTs of vitamin D supplementation on the incidence of acute respiratory tract infection (incorporating both URTI and LRTI). They also performed subgroup analysis based on vitamin D level, vitamin D dosing, dose size, and age, among other variables. Over 11,000 patients were included in the analysis, and overall, vitamin D was associated with a 12% reduction in acute RTI (aOR 0.88, 95% CI 0.81 to 0.96, p-value 0.003), which seems to have been driven mostly by pediatric studies as well a subgroup of patients with vitamin D <25nmol/L:
Looking at the Forrest plot (their two step analysis) showed an aOR of 0.80 (95% CI 0.69 to 0.93):
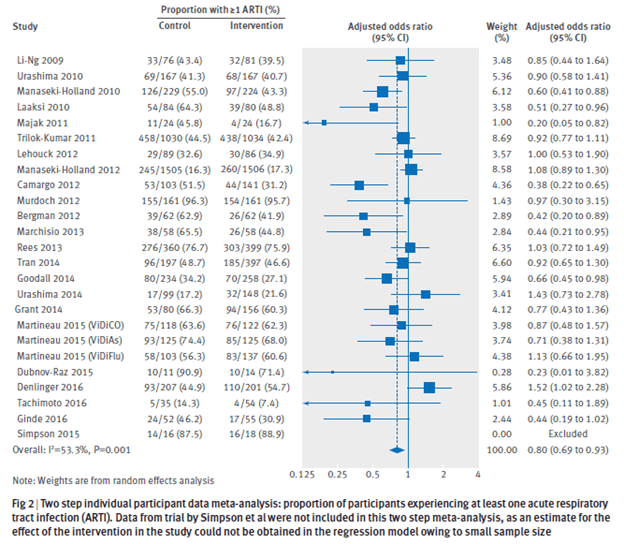
However all but one of the studies (Bergman 2012) that had any statistical difference were pediatric studies. Furthermore, seems that the benefit is seen mostly in studies using daily or weekly dosing vs bolus dosing (monthly):
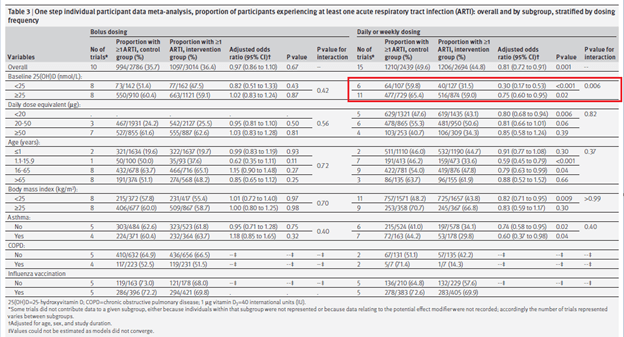
And this benefit applied mostly to URTI and did not have an impact on LRTI (both secondary outcomes) or antibiotic use:

Overall, the evidence on the use of vitamin D is not very concrete. On the one hand, there is some noise suggesting that those with low vitamin D levels at baseline as well children would benefit from vitamin D supplementation to prevent frequent episodes of URI. This also applies to those who are immunosuppressed. Indeed, vitamin D deficiency may predispose people to more URI episodes than expected. There seems to be no benefit of supplementation to those who are vitamin D replete, however. In light of this, it is reasonable to supplement those at risk patients and those who are vitamin D deficient, but vitamin D in and of itself is not a silver bullet for upper and lower respiratory tract infection treatment. Data suggests that either daily or weekly supplementation may be better than monthly supplementation.
References:
- Yamshchikov, Alexandra & Desai, Nirali & Blumberg, Henry & Ziegler, Thomas & Tangpricha, Vin. (2009). Vitamin D for Treatment and Prevention of Infectious Diseases: A Systematic Review of Randomized Controlled Trials. Endocrine practice : official journal of the American College of Endocrinology and the American Association of Clinical Endocrinologists. 15. 438-49. 10.4158/EP09101.ORR.
- Ginde, Adit A et al. “Association between serum 25-hydroxyvitamin D level and upper respiratory tract infection in the Third National Health and Nutrition Examination Survey.” Archives of internal medicine vol. 169,4 (2009): 384-90. doi:10.1001/archinternmed.2008.560
- Bergman P, Norlin AC, Hansen S, et al. Vitamin D3 supplementation in patients with frequent respiratory tract infections: a randomised and double-blind intervention study. BMJ Open. 2012;2(6):e001663. Published 2012 Dec 13. doi:10.1136/bmjopen-2012-001663
- Loeb M, Dang AD, Thiem VD, et al. Effect of Vitamin D supplementation to reduce respiratory infections in children and adolescents in Vietnam: A randomized controlled trial. Influenza Other Respir Viruses. 2019;13(2):176-183. doi:10.1111/irv.12615
- Camargo CA, Sluyter J, Stewart AW, et al. Effect of Monthly High-Dose Vitamin D Supplementation on Acute Respiratory Infections in Older Adults: A Randomized Controlled Trial. Clin Infect Dis. 2020;71(2):311-317. doi:10.1093/cid/ciz801
- Murdoch DR, Slow S, Chambers ST, et al. Effect of vitamin D3 supplementation on upper respiratory tract infections in healthy adults: the VIDARIS randomized controlled trial. JAMA. 2012;308(13):1333-1339. doi:10.1001/jama.2012.12505
- Rees JR, Hendricks K, Barry EL, et al. Vitamin D3 supplementation and upper respiratory tract infections in a randomized, controlled trial. Clin Infect Dis. 2013;57(10):1384-1392. doi:10.1093/cid/cit549
- Martineau AR, Jolliffe DA, Hooper RL, et al. Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. BMJ. 2017;356:i6583. Published 2017 Feb 15. doi:10.1136/bmj.i6583
