
I am probably not the only one who doubts the utility of the physical exam in the diagnosis of disease. Indeed, when looking at the imaging modalities that we have at hand, including CT, MRI, PET, Echo, ultrasound, and how quickly we can get any of these studies now, the physical exam seems to be more of a rite of passage than anything useful. At its core, the physical exam is a tool to “look into the body” to diagnose disease and its creation dates to an era before we had such fancy tools. For a more in-depth discussion on the history of the physical exam, I recommend looking at the podcast “Bedside Rounds” by Adam Rodman. What does the data say about the utility of exam findings for pneumonia?
In a study from 1997 published in JAMA (1) the precision of signs and symptoms for the diagnosis of community-acquired pneumonia in the outpatient setting was reviewed. Overall, they found that no single symptom by itself was able to rule out or rule in pneumonia without the aid of a CXR (based on likelihood ratios):
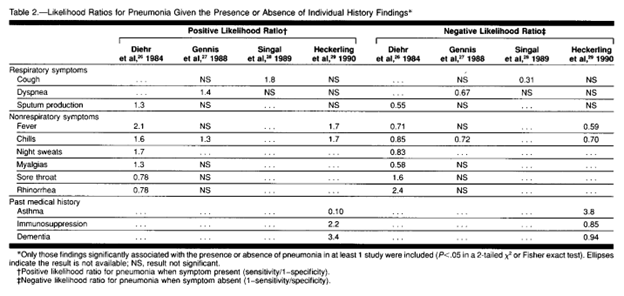
Physical exam findings that were highly associated were egophony and fever. The absence of fever, RR <30, and HR <100, had a negative likelihood ratio of 0.18 (95% CI 0.07-0.46). Crackles, by themselves, would not be enough to rule in our out disease:
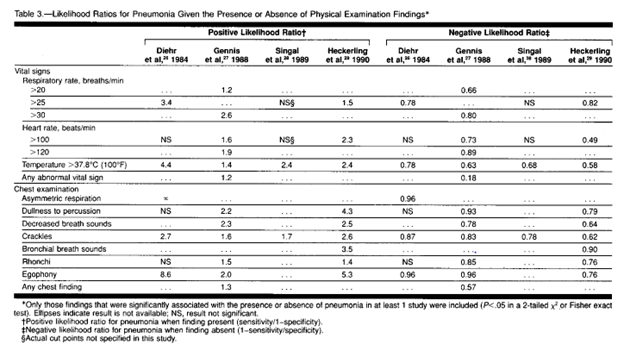
Looking at the negative likelihood ratios is also helpful. For instance, the absence of crackles has a negative likelihood ratio ranging from 0.62 to 0.87, suggesting that its absence may not be enough to rule out disease. Similarly, lack of cough only has a negative likelihood ratio of 0.31 at best, while lack of sputum production has a negative LR of 0.51, suggesting their absence does not rule out pneumonia.
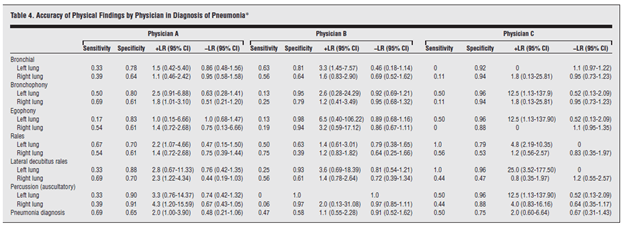
A later VA study of 52 patients with suspected pneumonia evaluated the sensitivity and specificity of the pulmonary exam. In this study, 28 of these patients had radiographically confirmed pneumonia and 3 physicians were tasked with performing the pulmonary exam (which took about 10 minutes…yeah, no one is taking this long to round on a patient nowadays.) Of course, with 3 different physicians, there is going to be a significant degree of interobserver variability. . In general, rales were the finding that had the highest degree of agreement between examiners, while bronchophony, egophony, and bronchial breath sounds had the lowest degree of agreement:

As noted, sensitivity and specificity between examiners differ depending on the physical exam finding, though the highest sensitivity was found to be listening to rales in the upright position, while percussion, egophony, and rales in the dependent position were found to have the highest specificity:
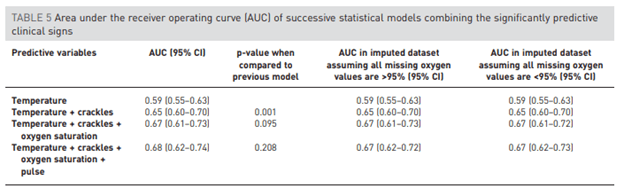
In another prospective study from 2017 (3), 720 patients with acute lower respiratory tract symptoms who presented to the primary care setting with a CXR performed within 7 days were evaluated. Specifically, they evaluated the risk factors associated with CXR findings of pneumonia. Signs such as fever, crackles, pulse >100 and low O2 saturation all had significant independent predictive value:
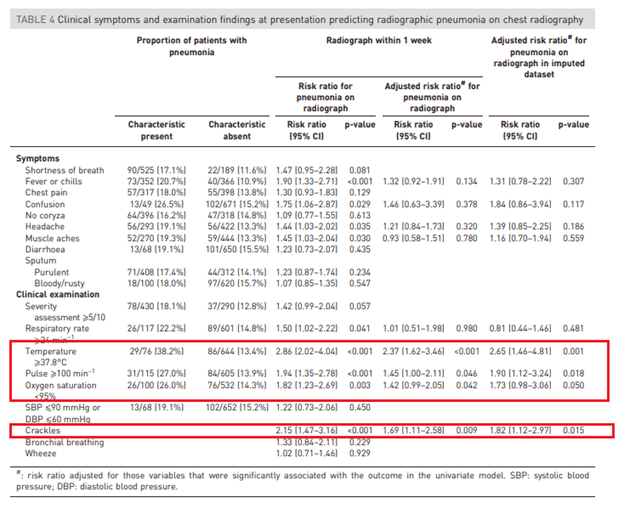
AUC of each predictive values are highlighted below, however they only reach an AUC of 0.68 when pooling temperature, crackles, O2 sat and elevated pulse:
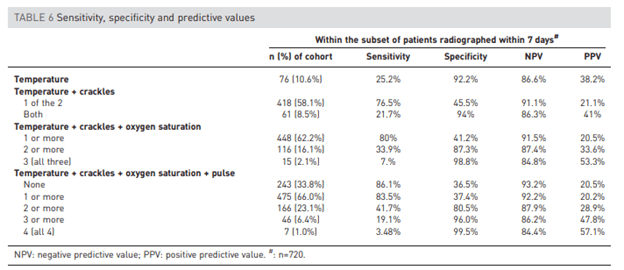
The overall sensitivity decreases with additional signs (For instance, presence of fever, unilateral crackles, oxygen saturation, and pulse has a sensitivity of ~3.5%). However, the absence of any of those symptoms has a high negative predictive value, despite all 4 symptoms put together having a PPV of only 57.1% (in other words, you cannot rule in pneumonia despite having all 4 signs at hand by themselves).
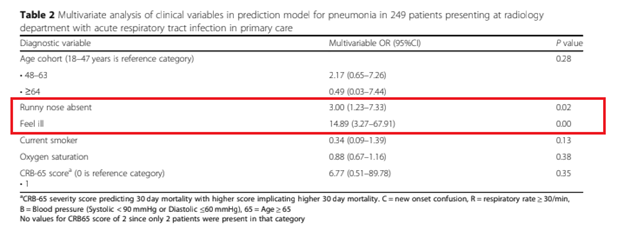
A prospective observational study (4) evaluated the role of signs and symptoms in the diagnosis of a consolidative pneumonia in the outpatient setting, based on CXR. 249 patients were included, and 12% of these were found to have a consolidation on imaging. Risk factors for consolidation included lack of runny nose (so not URI) and “feeling ill” whatever that means:
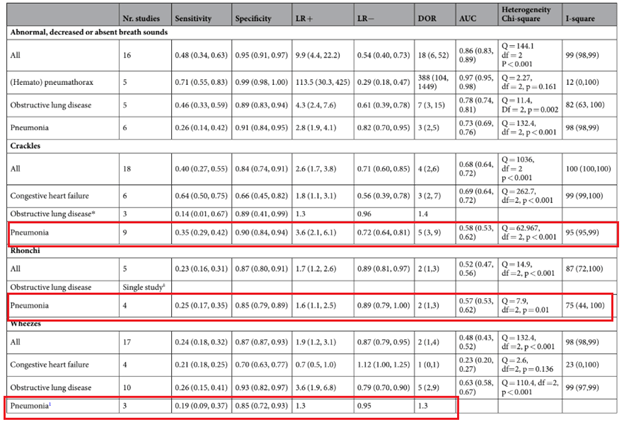
More recently, a meta-analysis (5) evaluated the diagnostic accuracy of lung auscultation for 4 common diseases, including CHF, pneumothorax, pneumonia, and obstructive lung disease. 34 studies, including 14814 patients, were included. The overall pooled sensitivity for lung auscultation was 37% (95% CI 30-47%) and specificity 89% (95% CI 85-92%). This was also seen when evaluating the studies for pneumonia:
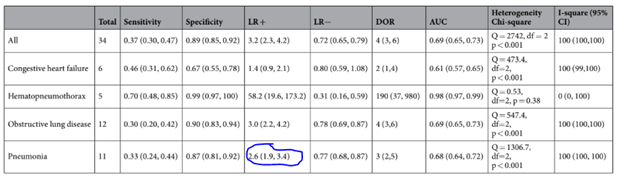
Further delineating specific breath sounds, crackles had the highest sensitivity and second to highest specificity while wheezing had the lowest sensitivity for pneumonia:
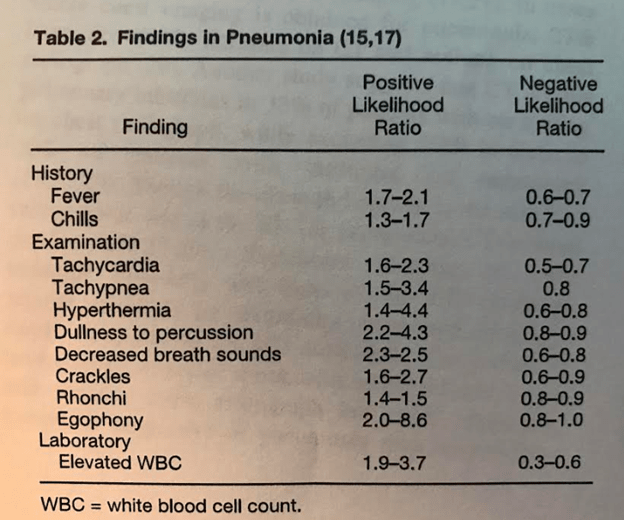
In another review (6) of ER patients with suspected community acquired pneumonia, the most common signs of pneumonia when compared to imaging included
- Cough (79-91%)
- Fever (up to 80%)
- Increased sputum production (up to 65%)
- Pleuritic chest pain (up to 50%)
- RR >24 (45-70%)
- Dyspnea (70%)
Further review of signs and symptoms noted that dullness to percussion, decreased breath sounds, and egophony were the most reliable physical exam findings for pneumonia:
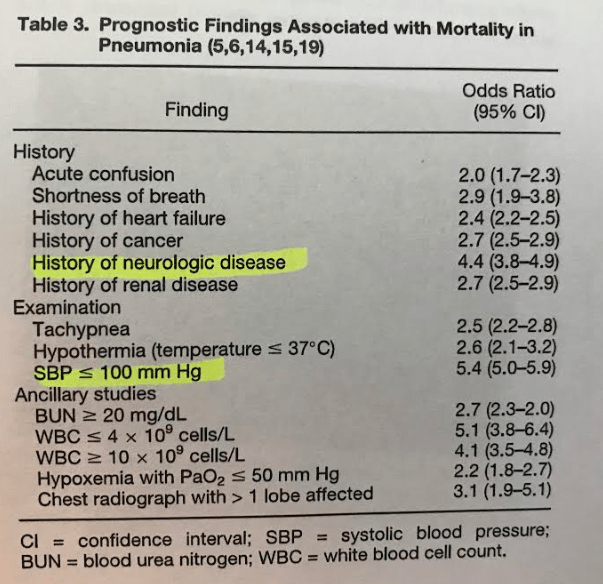
The most helpful prognostic markers for pneumonia based on their metanalysis include history of neurological disease, SBP <100 and lymphopenia:
What about using biomarkers such as CRP or ESR?
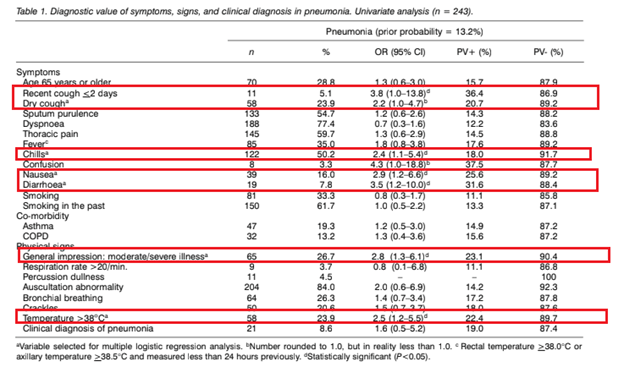
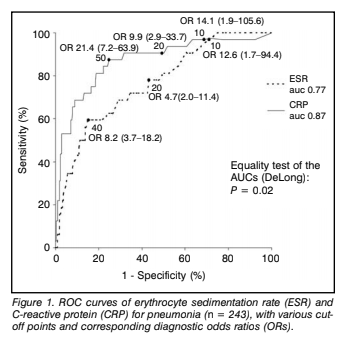
The diagnostic value of signs, symptoms, and ESR/CRP was evaluated in comparison to CXR in the outpatient setting (7). 246 patients were included, and pneumonia was diagnosed based on imaging in 32 patients (13%). Signs that were associated with pneumonia included chills, nausea, diarrhea while physical exam findings that were associated with pneumonia included fevers and “looking ill.”
Comparing both inflammatory markers, CRP at all cutoff values was significantly better than ESR in the diagnosis of pneumonia:
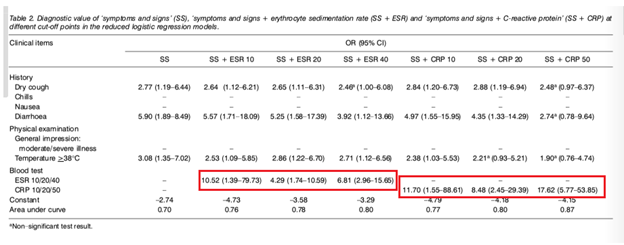
And combining clinical parameters with either CRP or ESR yielded a higher diagnostic value. For instance, combining CRP with signs and symptoms (cough, chills, nausea or diarrhea) yielded an OR of 17.62. In comparison, using dry cough or temperature by itself yielded an OR of 2.77 and 3.08 respectively.
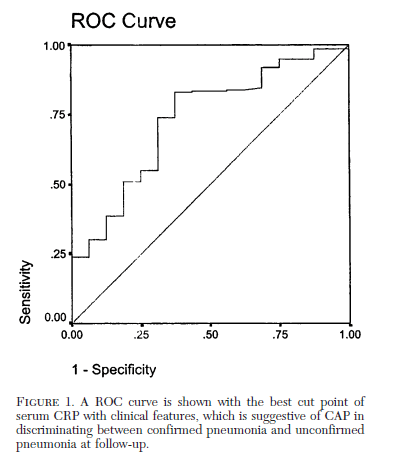
Data from a case cohort study (8) was used to evaluate the usefulness of CRP in the diagnosis of pneumonia. Patients with confirmed pneumonia had higher CRP levels (median 110.7 95% CI 8-182) compared to unconfirmed pneumonia (median 31.9 95% CI 1.5-160) and healthy controls (median 1.9 95% CI 0.3-11). Using a cutoff of 11, the sensitivity was 94% and specificity was 95% for discriminating CAP/unconfirmed CAP from healthy controls. Using a cut-off of 33.2 yielded a sensitivity of 83% and specificity of 62.5% for differentiating CAP and unconfirmed CAP:
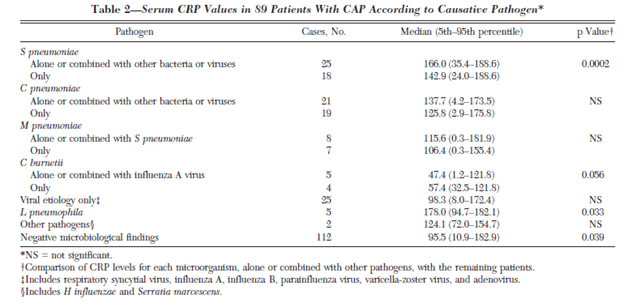
Median CRP levels were highest for Streptococcal pneumonia and legionella when compared to viral etiologies:
CRP was also higher for those who were admitted compared to those treated as outpatients:
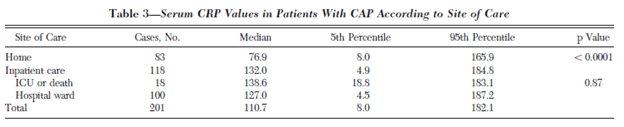
Notably, patients with co-morbidities had higher CRP levels. For instance, those without illnesses had a median CPR of 99.5 (95% CI 4.2-178), those with one co-morbidity had a median CRP 105.9 (95% CI 8 to 183) and those with 2 illnesses had a median CRP of 144 (95% CI 12 to 188.6, p-value 0.03).
Another prospective study (9) of patients presenting to an outpatient clinic with lower respiratory tract symptoms evaluated the utility of clinical signs and inflammatory markers on the diagnosis of pneumonia. A CRP >20 had a sensitivity of 0.73 and specificity of 0.65 for predicting radiographic pneumonia. Adding the CRP to a clinical diagnosis decreased the sensitivity to 0.49 and increased the PPV from 0.24 to 0.32. The NPV decreased from 0.94 to 0.91. In other words, a negative CRP may be a good screening out tool, but a positive CRP (at least >20) did not guarantee a diagnosis of pneumonia, which is not surprising given the non-specific nature of CRP.

So what is the takeaway here? CRP, in the right clinical context, in conjunction with physical exam, can be used to diagnose pneumonia in the absence of radiographic evidence. On the in-patient setting, where everyone who passes through the ER gets a CXR, the utility may not be there especially with the overall non-specific nature of the test. Either way, not one test, symptom, or exam finding is very sensitive or specific for pneumonia (go figure). Each of the exam findings, by themselves, are not useful but the clinical syndrome, in combination with either imaging or inflammatory markers, is the best bet to diagnose pneumonia upfront.
TL;DR
- Sensitivity for each exam finding is very low and subject to interobserver differences. Having said that, egophony tends to be more sensitive than crackles in most studies
- The triad of fever, cough, and sputum production does not guarantee the presence of pneumonia.
- The most sensitive signs include fever, tachycardia, and tachypnea
- The presence of 4 signs/symptoms, such as fever, tachycardia, low oxygen saturation, and crackles, has a high specificity but low sensitivity
- CRP and other inflammatory markers may help rule out pneumonia in the right clinical setting (i.e. the outpatient setting with no risk factors), but a positive CRP may not help rule in disease.
References:
- Metlay JP, Kapoor WN, Fine MJ. Does this patient have community-acquired pneumonia? Diagnosing pneumonia by history and physical examination. JAMA. 1997;278(17):1440-1445.
- Wipf JE, Lipsky BA, Hirschmann JV, et al. Diagnosing pneumonia by physical examination: relevant or relic?. Arch Intern Med. 1999;159(10):1082-1087. doi:10.1001/archinte.159.10.1082
- Moore M, Stuart B, Little P, et al. Predictors of pneumonia in lower respiratory tract infections: 3C prospective cough complication cohort study. Eur Respir J. 2017;50(5):1700434. Published 2017 Nov 22. doi:10.1183/13993003.00434-2017
- Arts L, Lim EHT, van de Ven PM, Heunks L, Tuinman PR. The diagnostic accuracy of lung auscultation in adult patients with acute pulmonary pathologies: a meta-analysis. Sci Rep. 2020;10(1):7347. Published 2020 Apr 30. doi:10.1038/s41598-020-64405-6
- Groeneveld GH, van ‘t Wout JW, Aarts NJ, et al. Prediction model for pneumonia in primary care patients with an acute respiratory tract infection: role of symptoms, signs, and biomarkers. BMC Infect Dis. 2019;19(1):976. Published 2019 Nov 20. doi:10.1186/s12879-019-4611-1
- Long B, Long D, Koyfman A. Emergency Medicine Evaluation of Community-Acquired Pneumonia: History, Examination, Imaging and Laboratory Assessment, and Risk Scores. J Emerg Med. 2017;53(5):642-652. doi:10.1016/j.jemermed.2017.05.035
- Hopstaken RM, Muris JW, Knottnerus JA, Kester AD, Rinkens PE, Dinant GJ. Contributions of symptoms, signs, erythrocyte sedimentation rate, and C-reactive protein to a diagnosis of pneumonia in acute lower respiratory tract infection. Br J Gen Pract. 2003;53(490):358-364.
- Almirall J, Bolíbar I, Toran P, et al. Contribution of C-reactive protein to the diagnosis and assessment of severity of community-acquired pneumonia. Chest. 2004;125(4):1335-1342. doi:10.1378/chest.125.4.1335
- Holm A, Nexoe J, Bistrup LA, et al. Aetiology and prediction of pneumonia in lower respiratory tract infection in primary care. Br J Gen Pract. 2007;57(540):547-554.
