
Nocardia spp is an interesting bug. It is a filamentous gram positive rod that is present in the environment, usually found in soil and organic matter aka the environment. Usually patients who are immunosuppressed (i.e. solid-organ transplant, high dose steroids, HIV) tend to be those who are at highest risk of infection. The most common site of infection is lungs, leading to pulmonary nocardiosis. One of the odd things about nocardia is its predilection for CNS infection, usually in the form of abscesses. This ultimately leads to prolonged therapy, usually about a year.
Having said that, one of the recommendations that are made whenever Nocardia is diagnosed outside of the CNS is brain imaging, either CT or MRI. Does every patient with pulmonary or cutaneous Nocardia need CNS imaging? The easiest way to answer this is to look at the prevalence of Nocardia CNS infection.
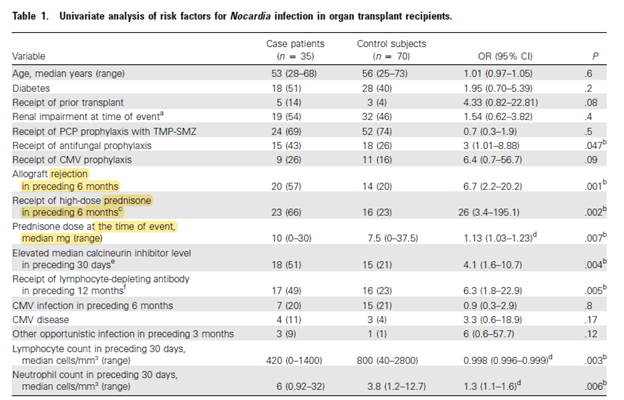
The following two studies evaluated the risk factors for Nocardia spp infection in the SOT population. In a single center study of 35 patients (1) with Nocardia matched with 70 controls, univariate analysis of risk factors associated with nocardia infection included allograft rejection and high dose prednisone in the prior 6 months:
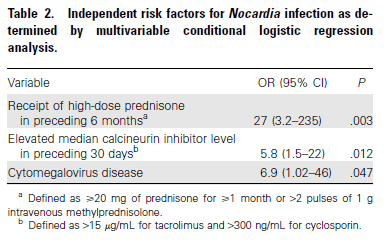
In the multivariate analysis, CMV disease and elevated calcineurin inhibitor level in the prior 30 days were risk factors identified for invasive disease:
CNS disease was found in 3 patients, however only 18 patients had any sort of neuro imaging done (leading to a prevalence of ~17% of CNS nocardiosis, at least in those who were imaged):
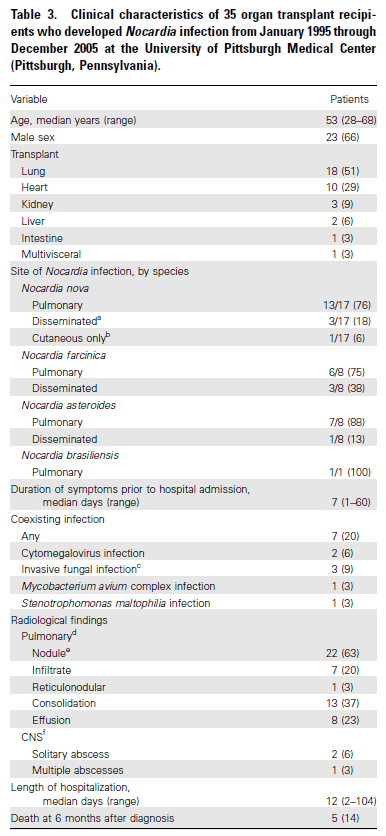
The authors defined disseminated infection as involvement of >2 non-contiguous organs OR disease of CNS. Counting these, there were 7 cases of disseminated Nocardia infection, counting the 3 known CNS nocardia infection.
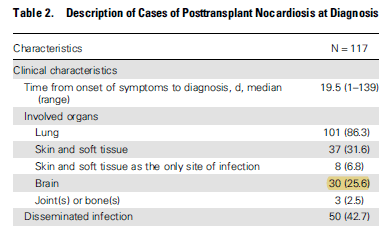
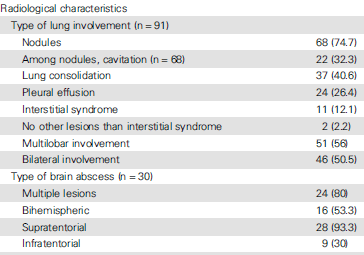
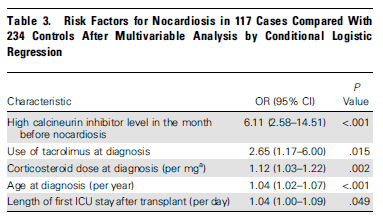
In another multicenter retrospective study (2), 117 cases of Nocardia were matched with 234 controls. In this cohort, 30 patients (25.6%) were identified as having CNS disease, making it the third most common site of infection after pulmonary and skin and soft tissue infection:
The most common radiological finding of CNS nocardia was multiple lesions and supratentorial location:
Risk factors by univariate analysis included donor age, length of stay in ICU after transplant, and acute rejection in the prior 6 months. In multivariate analysis, high CNI levels, use of FK, steroid use, and length of ICU stay were identified as risk factors:
Given this was a larger study, I am more tempted to believe the prevalence of CNS disease is the SOT population matches this cohort more than the previous one. Indeed, another review found that CNS nocardia was found in 2 out of 13 patients evaluated (3). Most of these tend to present with pulmonary disease. In another study of 20 patients with CNS nocardia (4), 11 were found to have concurrent pulmonary infections while 4 had skin and soft tissue infections. 2 of the 20 patients were asymptomatic in terms of CNS disease and were found to have CNS disease after Nocardia was found elsewhere. A review of the literature also found that CNS nocardia had a case fatality rate of 23.8%.
Further data comes from a retrospective study (5) of 84 patients with Nocardia. In this study, 5 patients with CNS disease were identified (incidence of ~6%). Notably, 2 of these patients had pulmonary involvement, while the remaining 3 had primary CNS infection. 4 of these 5 patients had nonspecific generalized symptoms and 2 additional patients had an Aspergillus co-infection. In their review of additional 84 CNS nocardia cases, of which 54 patients were considered to have primary CNS nocardia, 27 patients (32.1%) were found to have concurrent pulmonary involvement. Imaging consisted of either CT or MRI of brain, with 39 having a single-ring enhancing lesions and 39 with multiple ring enhancing lesions. Mortality ranged from 15.3% of patients treated with TMP-SMX up to 32% in those who did not get TMP-SMX.
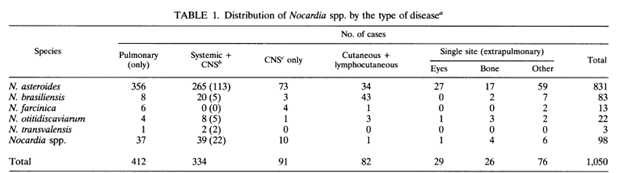
The largest review (6) evaluated 1050 cases from the literature, of which 238 cases (22.67%) involved the CNS. 44% of patients with systemic nocardiosis also had CNS infections, with lungs being the most common site of primary infection. More worrisome, however is that 91 patients (38.2%) with CNS infections actually had no other site of primary infection.
This suggests that anywhere from 20-40% of patients with pulmonary or systemic Nocardia may harbor CNS disease, of which many may actually have no symptoms whatsoever. Because of this prevalence, as well, as the multiple risk factors of these patients and length of therapy needed for CNS infection, all patients with pulmonary Nocardia should get brain imaging with either CT or MRI if suspicion is high with negative CT. Further, cutaneous disease should also prompt imaging of lungs and brain if there are risk factors such as SOT, HIV, high steroid dose.
TL;DR
- Patients with SOT, HIV, steroid use are at high risk of pulmonary Nocardiosis
- The prevalence of CNS disease with Nocardia ranges from ~15-44%, depending on the study.
- Many patients will be asymptomatic, despite having CNS disease
- IF pulmonary disease found, CT imaging of head should be done to rule out CNS disease, as these patients require a prolonged length of therapy.
References:
- Peleg AY, Husain S, Qureshi ZA, et al. Risk factors, clinical characteristics, and outcome of Nocardia infection in organ transplant recipients: a matched case-control study. Clin Infect Dis. 2007;44(10):1307-1314. doi:10.1086/514340
- Coussement J, Lebeaux D, van Delden C, et al. Nocardia Infection in Solid Organ Transplant Recipients: A Multicenter European Case-control Study. Clin Infect Dis. 2016;63(3):338-345. doi:10.1093/cid/ciw241
- Wadhwa T, Baveja U, Kumar N, Govil D, Sengupta S. Clinical manifestations of nocardiosis: Study of risk factors and outcomes in a tertiary care hospital. J Lab Physicians. 2017;9(4):288-295. doi:10.4103/JLP.JLP_111_16
- Rafiei N, Peri AM, Righi E, Harris P, Paterson DL. Central nervous system nocardiosis in Queensland: A report of 20 cases and review of the literature [published correction appears in Medicine (Baltimore). 2017 Jun 08;96(23):e7229]. Medicine (Baltimore). 2016;95(46):e5255. doi:10.1097/MD.0000000000005255
- Anagnostou T, Arvanitis M, Kourkoumpetis TK, Desalermos A, Carneiro HA, Mylonakis E. Nocardiosis of the central nervous system: experience from a general hospital and review of 84 cases from the literature. Medicine (Baltimore). 2014;93(1):19-32. doi:10.1097/MD.0000000000000012
- Beaman BL, Beaman L. Nocardia species: host-parasite relationships. Clin Microbiol Rev. 1994;7(2):213-264. doi:10.1128/cmr.7.2.213
