
Fever, thrombocytopenia, and transaminitis. I can be describing full blown septic shock with DIC, HIT (especially if you get a clot in this setting) and TTP (again, clots causing fever and Budd Chiari). Having said that, there is a selection of infections that tend to cause this pattern of fever, low platelets, and elevated LFTs.
Tick Borne Illnesses
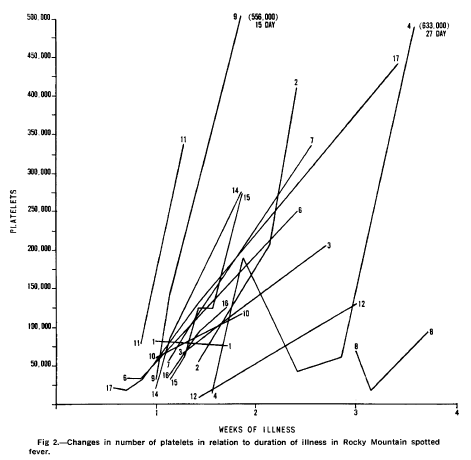
One of the earlies examples of thrombocytopenia was seen in a retrospective study of 17 patients (1) (mostly pediatric), where initial platelet counts ranged from 7,000 up to 105,000:
In a retrospective study from Arizona (2), evaluating an outbreak that occurred within an Indian reservation in 2003 linked to the brown dog tick, 205 patients with RMSF were evaluated and compared to 175 controls. The triad of fever, rash, and tick exposure were more likely in the cases. Platelets were significantly lower in the RMSF group when compared to the control group. Further, cases were more likely to have elevated transaminases:
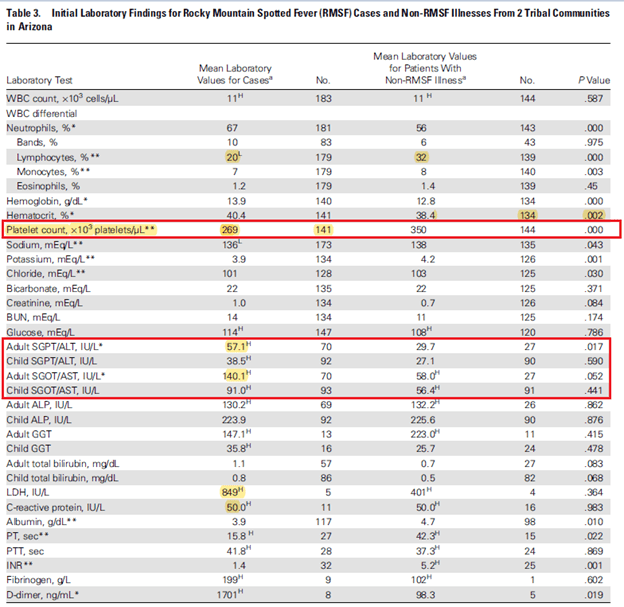
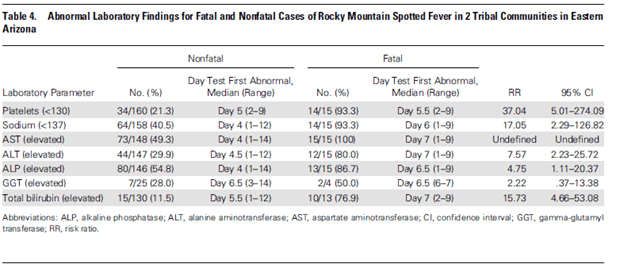
Those with RMSF were more likely to have significant thrombocytopenia, with 17 patients having platelets <130,000 (12%) when compared to 2 out of 144 cases (1.4%). In a companion study (3) in the same issue of CID evaluating the risk factors for death, severe thrombocytopenia, elevated ALT, and hyponatremia were associated with late treatment with doxycycline and thus, death:
Another retrospective study on Anaplasmosis from China (4) evaluated 83 patients in terms of their clinical features and laboratory findings. Of these, 92.8% had thrombocytopenia with 50% having platelets <50k, and ~92% had transaminitis:
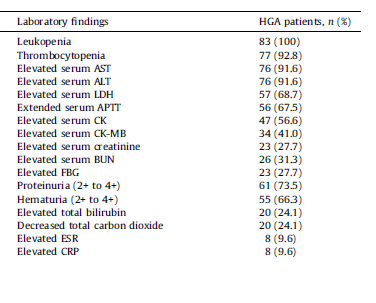
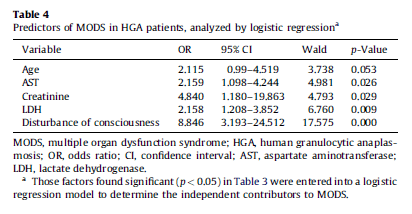
Therapy with doxycycline improved temperature within 4 days and normalized lab abnormalities within 7 days. Notably, within this cohort, 45.8% met SIRS criteria and 30.1% had multiorgan dysfunction syndrome, with age, AST, creatinine, LDH, and altered mentation being risk factors for MODS:
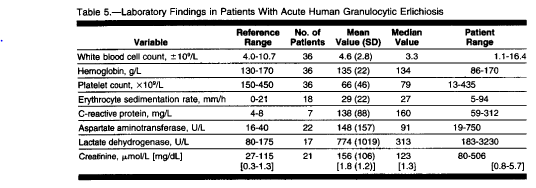
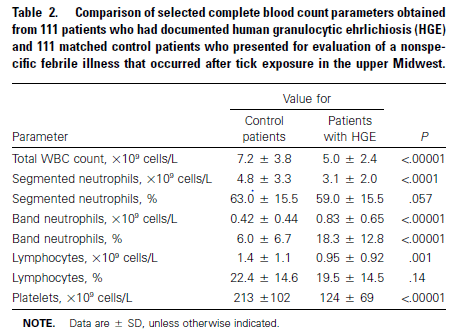
An older study (5) on Anaplasmosis (known as Human Granulocytic Ehrlichiosis) evaluated 41 patients with HGE. The most common symptoms were fever, malaise, rigors, myalgias, headaches, and seats. Patients generally had lower platelet counts and higher AST values:
And those who were hospitalized had lower platelet counts and higher liver function tests:
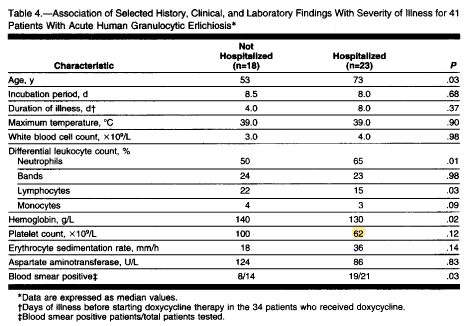
Doxycycline therapy abated fever within 2 days in 97% of patients and normalized lab values within 7 days as well.
A review of European cases of HGE (6) found that thrombocytopenia with platelets <150k and elevated transaminitis was a common occurrence as well:

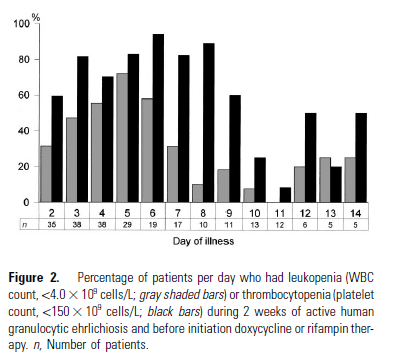
Another study (7) evaluated the proportion of patients who developed hematological abnormalities. In this cohort, 77.8% of patients had thrombocytopenia in at least one or more days of the illness and anywhere from 59.6% to 94.1% were found to have thrombocytopenia on any given day from day 2 through day 9:
Comparing cases to controls, cases had lower platelets and higher bands when compared to controls:
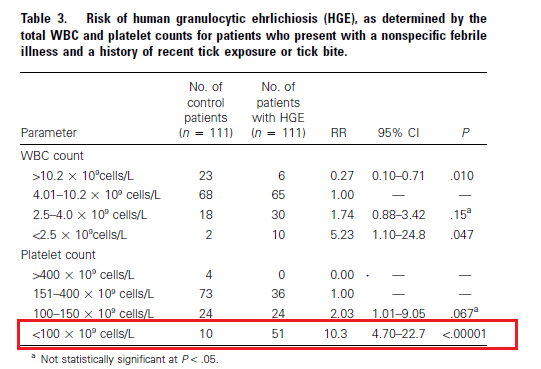
And those with thrombocytopenia with platelets <100k were 10 times more likely to have HGE when using this parameter alone:
These data points (i.e. platelets and LFTs) have been used to screen patients for anaplasmosis. For instance, a 2 phase study (8) was done evaluating both CBC and LFTs as a screening tool prior to ordering anaplasma PCR for diagnosis. Patients who tested positive for anaplasma by PCR were more likely to be lymphocytopenic, have transaminitis, and thrombocytopenia:
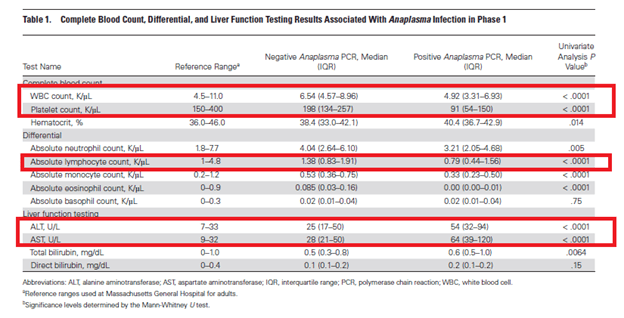
They were able to use an algorithm to screen patients prior to ordering PCR and found pretty good results with it. In a “mock” implementation, they had accepted 96% of the true positive PCRs and only rejected 4%.
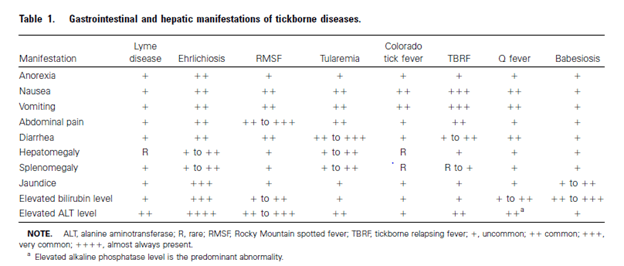
Another review (9) found that in most tick-borne illnesses, elevated ALT tended to be present in most:
Leptospirosis
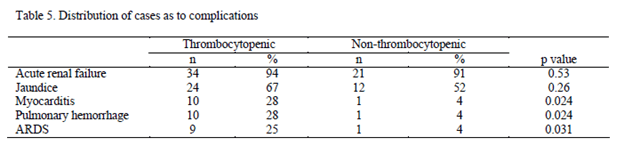
Leptospirosis is also a cause of this triad. For instance, a retrospective study (10) evaluated the incidence of thrombocytopenia during a time period in 1995 and 1996. 59 patients were evaluated and 36 (61%) of these were thrombocytopenic, usually within 4 days of presentation. Those who were thrombocytopenic were more likely to experience pulmonary hemorrhage, ARDS, and myocarditis. Notably, there were no statistical difference between groups in Jaundice.
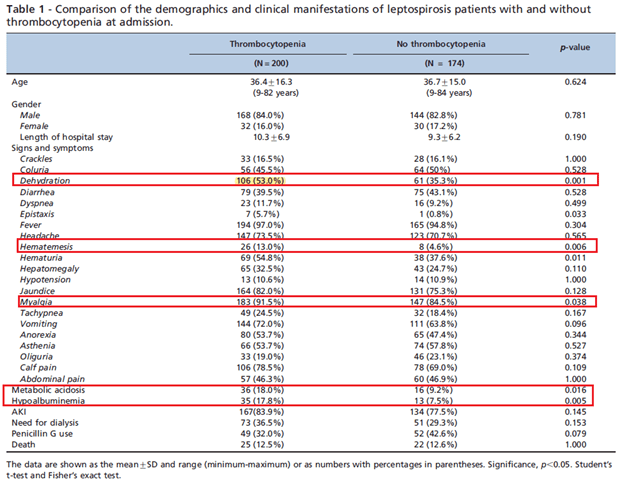
In another retrospective study (11) of 374 patients from Brazil, 200 patients (53.3%) admitted with Leptospirosis were found to have thrombocytopenia, with an additional 150 (40.3%) developing thrombocytopenia during their admission. Notably, thrombocytopenia was a marker of disease severity as these patients were more likely to have hypovolemia, hematemesis, myalgias, metabolic acidosis, and hypoalbuminemia:
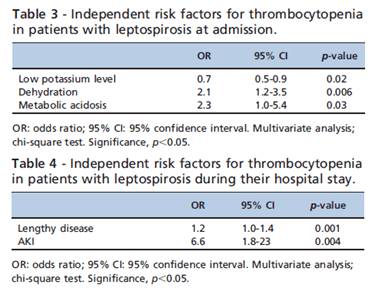
Low potassium, dehydration, and metabolic acidosis were found to be associated with initial TCP, while development of AKI was found to be associated with development of TCP during the admission:
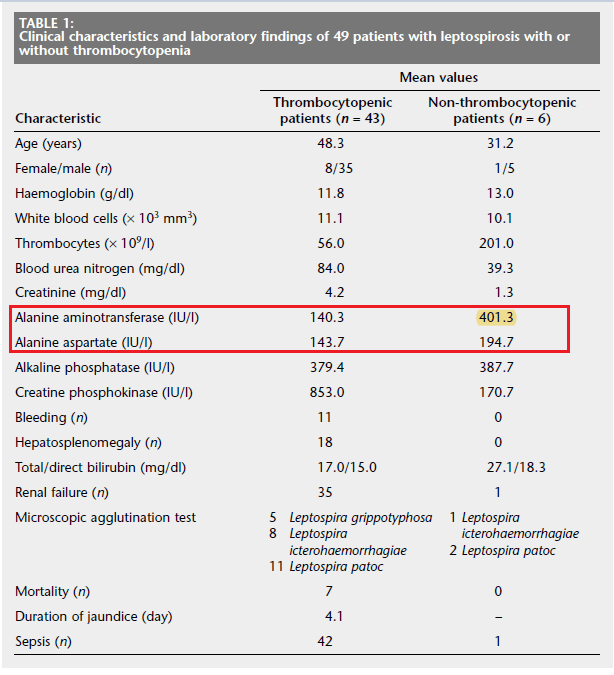
Further data comes from this Turkish retrospective study (12), where 49 patients were evaluated with 43 patients (87.8%). Bone marrow aspirations revealed hypercellularity with increased megakaryocytes in those with thrombocytopenia. Of interest, those without TCP had a significant higher ALT than those with TCP (though both had fairly elevated TCP):
Another prospective study (13) found that 46% of patients with leptospirosis had overt DIC (meaning they scored >5 points on the DIC score according to the International Society of Thrombosis and Hemostasis). In all aspects of coagulation tests, those with leptospirosis tended to have longer PT and PTT as well higher D-dimers when compared to controls:
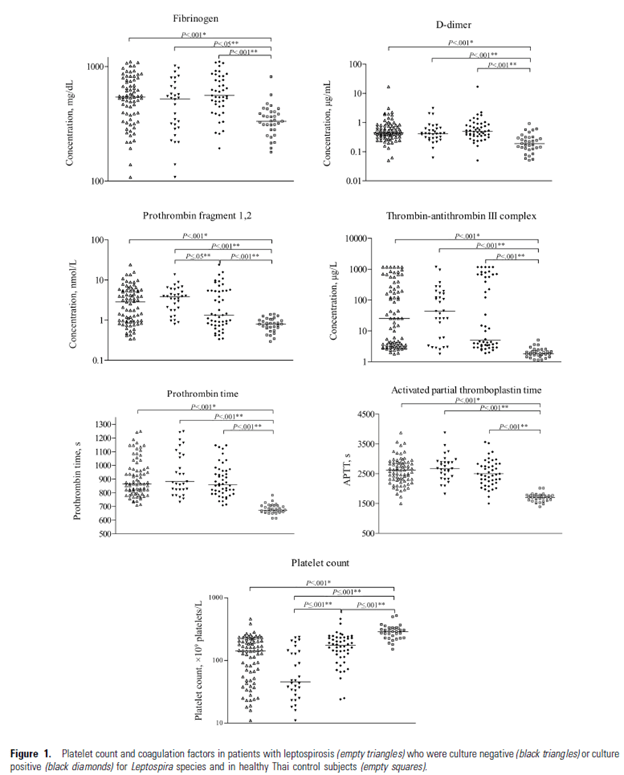
Clinical bleeding, however, was correlated with thrombocytopenia rather than other coagulation parameters.
Brucellosis
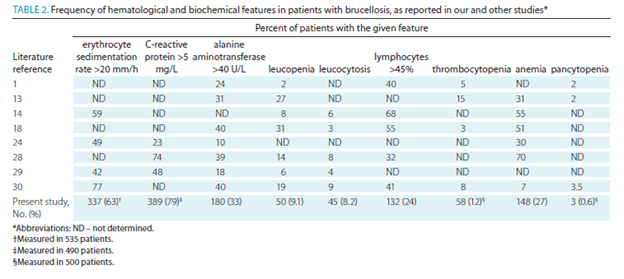
Brucella has been implicated in causing a similar acute presentation in terms of low platelets, however data suggest this is an infrequent finding. Most of the data comes from the Mediterranean. In a retrospective study (14) of 550 patients from 1998-2007, the most common clinical manifestation of Brucellosis was arthralgia, malaise, and fevers. A small percentage of patients (12%) had thrombocytopenia on admission. The most common lab abnormality in this series was elevated CRP.
In another retrospective study (15) of 418 patients, thrombocytopenia was noted only in a small subset of patients, including 4% of those with occupational exposure and 3.6% in the non-occupational exposure group. ALT was elevated in a higher percentage of patients, 31.5% in the occupational exposure group vs 35.5% in the non-occupational exposure.
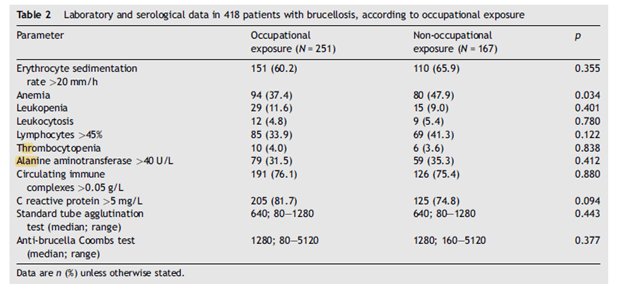
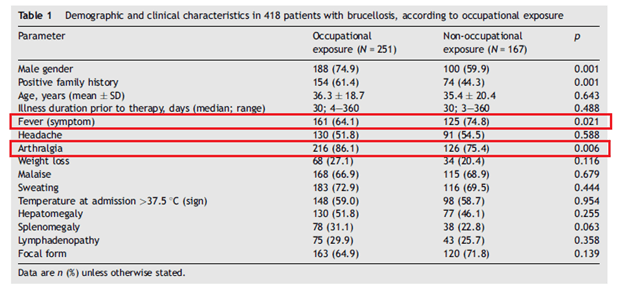
Like the prior study, the most common presentation in both groups was arthralgia, sweats, and fever:
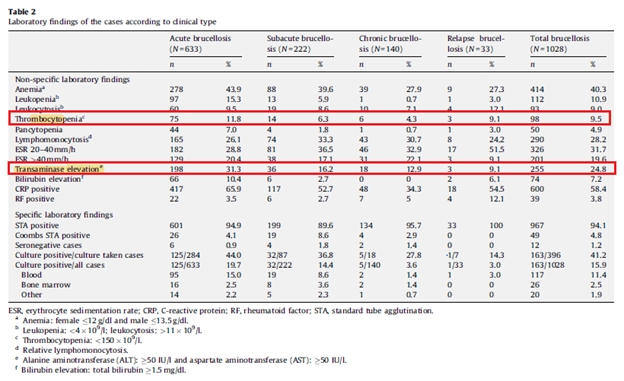
The largest retrospective study in the clinical characteristics of Brucellosis involves 1028 patients from Turkey during a 10 year period from 1/1998 to 9/2007 (16).. Across the spectrum of presentation, from acute to subacute to chronic brucellosis, the percentage of patients with thrombocytopenia was not impressive. The highest percentage was in acute Brucellosis, with 11.8% and decreasing to 4.3% in chronic brucellosis. LFT elevation was present in 31.3% of chronic brucellosis cases an only in 12.9% of chronic brucellosis.
All this to say, while Brucellosis may be cited as a cause of the unholy trinity, I am not terribly convinced thrombocytopenia is a prominent finding here. Everything else seems non-specific.
What is going on here?
A review of thrombocytopenia implied that many mechanisms are involved in thrombocytopenia. A few of the more compelling mechanisms include direct infection of platelets by bacteria, endothelial damage leading to platelet consumption, and hypersplenism. Whatever the case, the finding of both elevated LFTs and low platelets in conjunction with a rash OR high risk occupation should prompt an investigation for a tick-borne illness. Doxycycline up-front can be both a diagnostic and therapeutic tool. The one exception seems to be the “North American Bad Air” (Aka babesia), which needs more than Doxycycline. A response to doxycycline in terms of the fever curve should occur within 48-72hrs. Having said that, make sure to not miss the following non-interesting (read: non-infectious) diseases that can look like this, otherwise you’re going to have a bad time:
- Thrombotic thrombocytopenic purpura/Hemolytic Uremic Syndrome
- Heparin induced thrombocytopenia
- DIC complicated septic shock
References:
- Rubio T, Riley HD Jr, Nida JR, Brooksaler F, Nelson JD. Thrombocytopenia in Rocky Mountain spotted fever. Am J Dis Child. 1968;116(1):88-96. doi:10.1001/archpedi.1968.02100020090014
- Traeger MS, Regan JJ, Humpherys D, et al. Rocky mountain spotted fever characterization and comparison to similar illnesses in a highly endemic area-Arizona, 2002-2011. Clin Infect Dis. 2015;60(11):1650-1658. doi:10.1093/cid/civ115
- Regan JJ, Traeger MS, Humpherys D, et al. Risk factors for fatal outcome from rocky mountain spotted Fever in a highly endemic area-Arizona, 2002-2011. Clin Infect Dis. 2015;60(11):1659-1666. doi:10.1093/cid/civ116
- Li H, Zhou Y, Wang W, Guo D, Huang S, Jie S. The clinical characteristics and outcomes of patients with human granulocytic anaplasmosis in China. Int J Infect Dis. 2011;15(12):e859-e866. doi:10.1016/j.ijid.2011.09.008
- Bakken JS, Krueth J, Wilson-Nordskog C, Tilden RL, Asanovich K, Dumler JS. Clinical and laboratory characteristics of human granulocytic ehrlichiosis. JAMA. 1996;275(3):199-205.
- Blanco JR, Oteo JA. Human granulocytic ehrlichiosis in Europe. Clin Microbiol Infect. 2002;8(12):763-772. doi:10.1046/j.1469-0691.2002.00557.x
- Bakken JS, Aguero-Rosenfeld ME, Tilden RL, et al. Serial measurements of hematologic counts during the active phase of human granulocytic ehrlichiosis. Clin Infect Dis. 2001;32(6):862-870. doi:10.1086/319350
- Turbett, Sarah E., et al. “Use of Routine Complete Blood Count Results to Rule Out Anaplasmosis Without the Need for Specific Diagnostic Testing.” Clinical Infectious Diseases : an Official Publication of the Infectious Diseases Society of America, 2019.
- Zaidi SA, Singer C. Gastrointestinal and hepatic manifestations of tickborne diseases in the United States. Clin Infect Dis. 2002;34(9):1206-1212. doi:10.1086/339871
- Casiple LC. Thrombocytopenia and Bleeding In Leptospirosis. Phil J Microbiol Infect Dis. 1998;27(1):18-22
- Daher EF, Silva Junior GB, Silveira CO, Falca˜ o FS, Alves MP, Mota JA, et al. Factors associated with thrombocytopenia in severe leptospirosis (Weil’s disease). Clinics. 2014;69(2):106-110
- Turgut M, Sünbül M, Bayirli D, Bilge A, Leblebicioğlu H, Haznedaroğlu I. Thrombocytopenia complicating the clinical course of leptospiral infection. J Int Med Res. 2002;30(5):535-540. doi:10.1177/147323000203000511
- Chierakul W, Tientadakul P, Suputtamongkol Y, et al. Activation of the coagulation cascade in patients with leptospirosis. Clin Infect Dis. 2008;46(2):254-260. doi:10.1086/524664
- Bosilkovski M, Krteva L, Dimzova M, Vidinic I, Sopova Z, Spasovska K. Human brucellosis in Macedonia – 10 years of clinical experience in endemic region. Croat Med J. 2010;51(4):327-336. doi:10.3325/cmj.2010.51.327
- Bosilkovski M, Krteva L, Dimzova M, Kondova I. Brucellosis in 418 patients from the Balkan Peninsula: exposure-related differences in clinical manifestations, laboratory test results, and therapy outcome. Int J Infect Dis. 2007;11(4):342-347. doi:10.1016/j.ijid.2006.10.002
- Buzgan T, Karahocagil MK, Irmak H, et al. Clinical manifestations and complications in 1028 cases of brucellosis: a retrospective evaluation and review of the literature. Int J Infect Dis. 2010;14(6):e469-e478. doi:10.1016/j.ijid.2009.06.031
- L Pantanowitz. Mechanisms of Thrombocytopenia in Tick-Borne Diseases. The Internet Journal of Infectious Diseases. 2002 Volume 2 Number 2.
