
If you don’t get the joke, there is a movie called Meet the Fockers and I am always afraid of saying the wrong thing. The same thing applies to Faget’s sign.
Also known as Sphygmothermic dissociation. This is essentially a counterargument to the Liebermeister’s rule (which is in the running for the most epic named rule in medicine) – for every degree in centigrade the temperature increases, the heart rate will increase by 8 bpm. In Fahrenheit, each degree increase will yield an increase in 10bpm to the heart rate. Jean-Charles Faget, a French trained physician from New Orleans, noticed that those patients who acquired Yellow Fever tended to have slower pulses when febrile. His original paper can be seen here: https://archive.org/details/64430850R.nlm.nih.gov/page/n95/mode/2up
Of course, I do not speak French so have at it if you feel so compelled. Obviously, this was the time before beta blockers. Indeed beta blocker and CCB use tends to be the most common cause of relative bradycardia with fevers, so I will not focus on these. Other etiologies include CNS disease (like increased ICP), drug fevers, or significant hemorrhagic shock. While the vast majority of bradycardia in setting of fevers are iatrogenic, there are a variety of infections that tend to cause this clinical phenomena.
It has been proposed (1) that relative bradycardia can be applied to cases with temperature >102F, as it may be difficult to detect significant differences in the heart rate below these temperatures. The mechanism, however, is still up in the air. One review (2) proposed that pro-inflammatory cytokines may induce increased vagal tone, however how specific it is to the organisms that tend to cause this sign is unknown (I mean, all organisms cause release of cytokines so..).

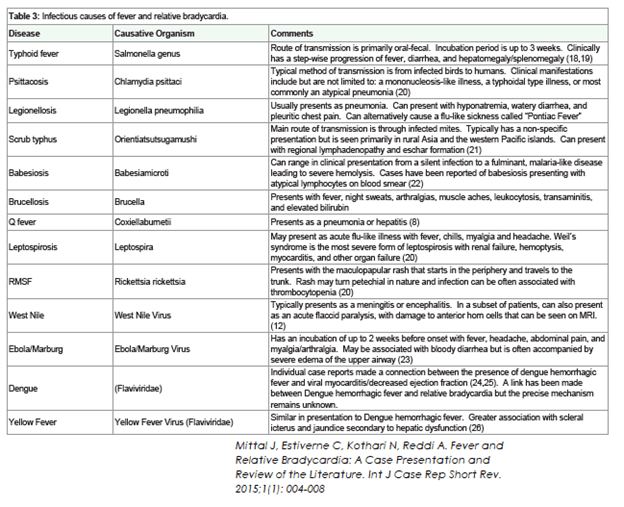
Having said that, there are several characteristics that these organisms share:
- Most are intra-cellular organisms, such as Legionella, Chlamydophila, Francisella tularensis, Salmonella Spp, Tick borne illnesses such as RSMF (goes to endothelial cells), Scrub typhus, and Babesia. The exception here is Leptospirosis, which is not intra-cellular.
- Most of the bacteria that cause this are gram negative.
- Viruses that cause this tend to be viral hemorrhagic fevers – Yellow Fever, Ebola, West Nile
Most of the data for each of these diseases tend to be limited to case reports or case series. Despite this, there is some strong data for this being a real phenomenon.
Salmonella spp.
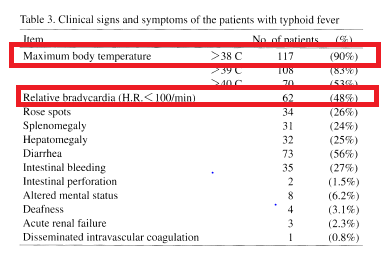
A retrospective study from Japan (4) evaluted 130 cases of typhoid fever from 1975-1998. The most common symptom in this population was fever in 90%, with diarrhea being the next symptom in 56%. In this population, 48% of patients had relative bradycardia, defined as a pulse <100 bpm despite elevated temperature:
In the interest of…well interest, most patients who received either chloramphenicol (90%), ampicillin/amoxicillin (75%) and fluroquinolones (98%) achieved clinical cure in this cohort.
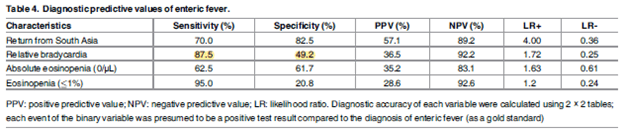
A more recent study (5) specifically evaluted the utility of relative bradycardia and eosphinophilia in the diagnois of enteric fever. In this case-control study, 40 patients with enteric fever were matched with 120 patients without enteric fever. After adjusting for confounders, they found that 88% of patients with enteric fever had relative bradycardia when compared to 51% of patients without enteric fever:
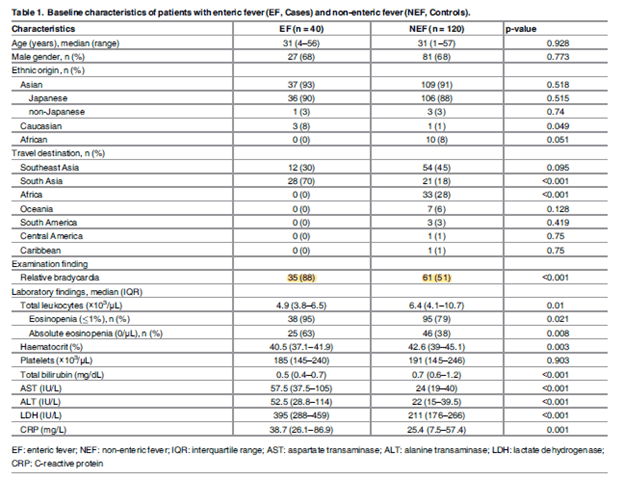
It should be noted that those without enteric fever had a hodgepodge of infections with either malaria (13%), dengue (11%), leptospirosis (2%), and rickettsia (1%). This may have influenzed the degree of relative bradycardia in the non-enteric fever group. As mentioned by the authors, when comparing enteric fever to each disease, relative bradycardia was significantly less common in cases than controls with malaria and dengue fever. Further, logistic regression demonstrated that relative bradycardia had an OR of 6.77 (95% CI 2.48-18.46) and adjusted OR of 11.69 (3.21-42.51):
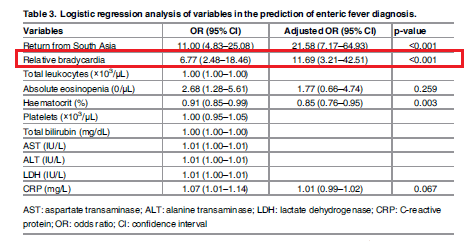
Sensitivity was fairly high, though not surprisingly the specificity of bradycardia was not great. Notably, the positive likelihood ratio here was 1.73 (not great), but negative likelihood ratio was 0.25:
Legionella
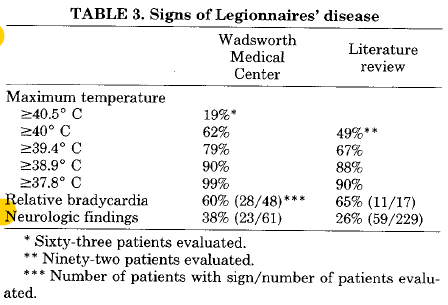
Probably the sasquach of atypical pneumonias, since I have found only like 2 thus far. An old paper (6) evaluated the incidence of Legionella pneumonia in a VA center in Seattle from 1977-1978. They also evalauted the literature up to that point. 65 patients were evaluated. Cough (92%), chills (77%), and diarrhea (47%) where the most common symptoms. 54% of their patients had hyponatremia, while their lit review revealed 68% incidence of hyponatremia. 28/48 of the patients evaluated experienced relative bradycardia, and in their literature review, they found an additional 11/17 with relative bradycardia:
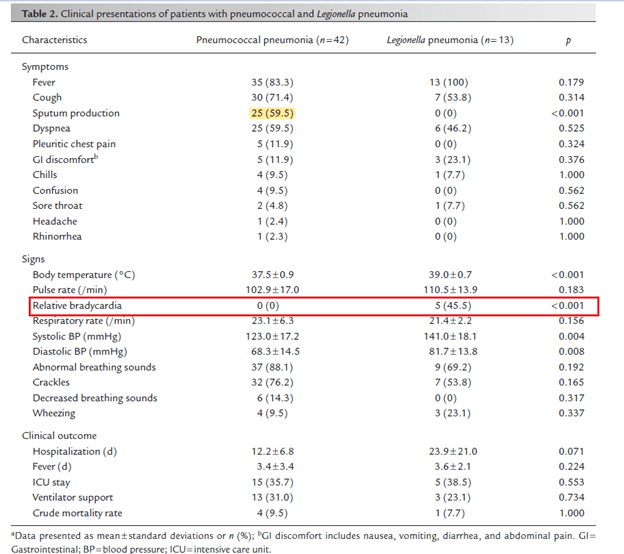
In another retrospective study (7), 42 patients with Pneumococcal pneumonia and 13 patients with legionella pneumonia were evaluated to determine distingushing characteristics of both disease. Notably, pneumococcus had a higher incidence (using urine antigen testing) when cmopared to Legionella, 28.4% vs 1.65% respectively. Patients with legionella were more likely to have relative bradycardia when compared to pneumococcus:
Tick Borne Illnesses
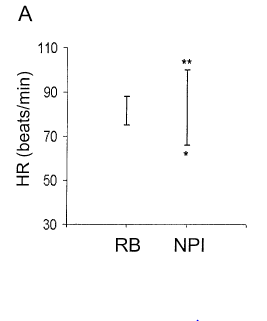
I decided to put a bunch of studies under this category, though surprisingly I did not find any good data on RMSF. In a case series of 17 patients with babesiosis (8) 8 of the 9 patients who presented with fever were found to have relative bradycardia. In another prospective study (9) of Orientia tsutsugamushi (aka Scrub Typhus), 100 febrile patients were examined to determine the relationship between heart rate and temperature. 53 patients had relative bradycardia (<10 beats/min increase per degree C):
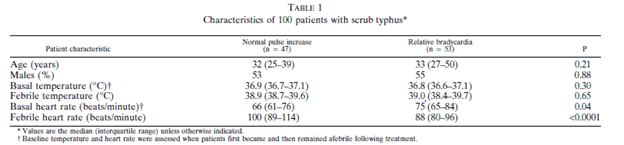
Those patients who had relative bradycardia had lower heart rates than the normal pulse increase cohort:
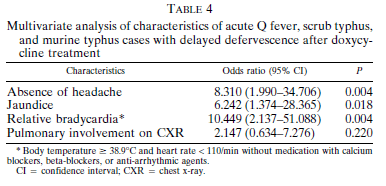
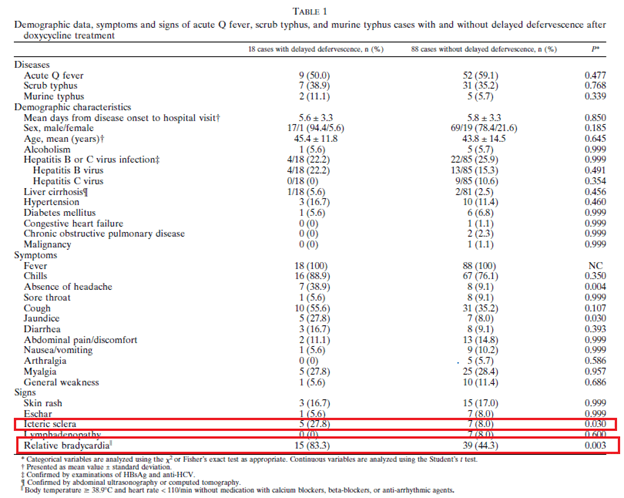
In a prospective study (10) evaluating the clinical characteristics of delayed defervescence in Q fever, scrub typhus, and murine typhus relative bradycaria was found to have an OR of 10.449 (95% CI 2.137-51.088) for delayed defervescence despite doxycycline treatment:
Relative bradycardia was found in 83.3% of those who had delayed defervescence and in 44.3% of those who did not:
This suggest that relative bradycardia may be used as a prognostic marker, especially in light of ongoing therapy.
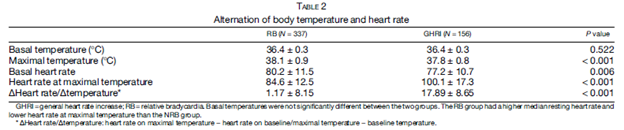
In the largest retrospective study (11), 493 patients with scrub typhus were evaluated over a period of 10 years. In 337 of these, relative bradycardia was seen with a significant higher temperature and lower heart rate at maximal temperature seen:
Viral Hemorrhagic Fevers:
One of the most well known causes of Faget’s is Yellow Fever. In a comprehensive study (12) of YF patients, sinus bradycardia was seen in 24% of patients, with 44% of patients how had undergone Holter monitoring having a HR of <60 bpm. The more severe patients tended to have more EKG abnormalities, 52% in those with mild-moderate disease vs 77% of those with severe disease. In another retrospective study (13) of Yellow Fever requiring ICU admissions, 51.8% of 114 admitted patients were found to have relative bradycardia. More suprisingly, this was found to be associated with reduced mortality when comparing survivors and non-survivors (HR 0.24 95% CI 0.13-0.44 p-value <0.01).
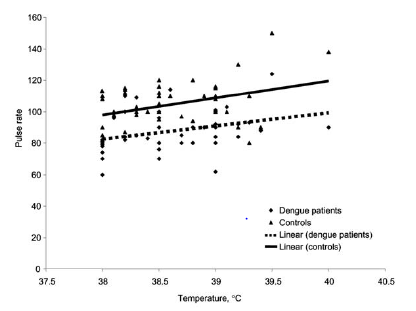
Dengue hemorrhagic fever has also been found to be associated with relative bradycardia. For instance, in one case report, a 36yo patient was found to have a fever of 104 degrees F and a pulse of 52 beats per minute (14). In another case-control study (15), dengue patients were found to have lower heart rates (87.6 +/- 12.5 bpm) when compared to controls (104.6 +/- 14 bpm; p-value <0.0001). At all temperatures, those with dengue were more likely to have lower heart rates:
TL;DR
- Faget’s sign refers to the lack of significant rise of heart rate in setting of increase temperature. Your HR goes up by 10bpm per one degree F.
- Intracellular gram negatives and viral hemorrhagic fevers tend to be the culprits. The one exception to this is Leptospirosis, because spirochetes are strange.
- The mechanism is unclear, but seems these infections increase vagal tone by some mythical mechanism.
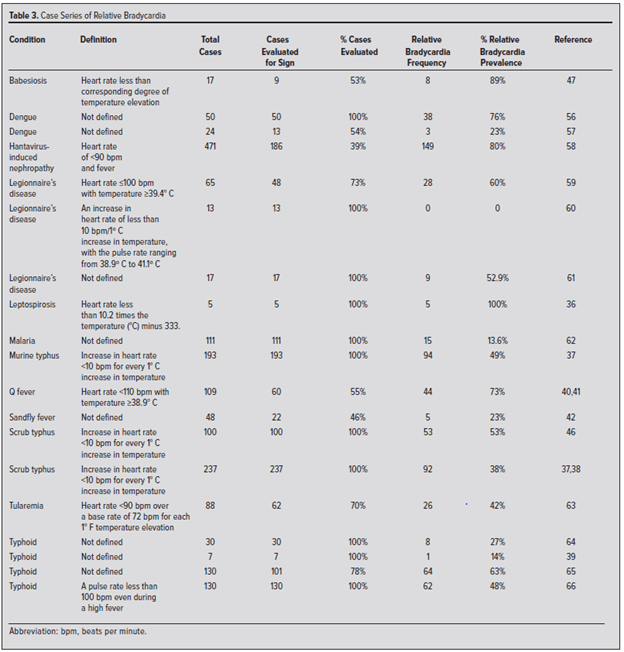
- Summary of data is below:
References:
- Cunha BA. The diagnostic significance of relative bradycardia in infectious disease. Clin Microbiol Infect. 2000;6(12):633-634. doi:10.1046/j.1469-0691.2000.0194f.x
- Ye F, Hatahet M, Youniss MA, Toklu HZ, Mazza JJ, Yale S. The Clinical Significance of Relative Bradycardia. WMJ. 2018;117(2):73-78.
- Mittal J, Estiverne C, Kothari N, Reddi A. Fever and Relative Bradycardia: A Case Presentation and Review of the Literature. Int J Case Rep Short Rev. 2015;1(1): 004-008
- Hoshino Y, Masuda G, Negishi M, et al. Clinical and bacteriological profiles of patients with typhoid fever treated during 1975-1998 in the Tokyo Metropolitan Komagome Hospital. Microbiol Immunol. 2000;44(7):577-583. doi:10.1111/j.1348-0421.2000.tb02536.x
- Matono T, Kutsuna S, Kato Y, et al. Role of classic signs as diagnostic predictors for enteric fever among returned travellers: Relative bradycardia and eosinopenia. PLoS One. 2017;12(6):e0179814. Published 2017 Jun 23. doi:10.1371/journal.pone.0179814
- Kirby BD, Snyder KM, Meyer RD, Finegold SM. Legionnaires’ disease: report of sixty-five nosocomially acquired cases of review of the literature. Medicine (Baltimore). 1980;59(3):188-205.
- Hung YP, Wu CJ, Chen CZ, et al. Comparisons of clinical characters in patients with pneumococcal and Legionella pneumonia. J Microbiol Immunol Infect. 2010;43(3):215-221. doi:10.1016/S1684-1182(10)60034-5
- Kim N, Rosenbaum GS, Cunha BA. Relative bradycardia and lymphopenia in patients with babesiosis. Clin Infect Dis. 1998;26(5):1218-1219. doi:10.1086/520302
- Aronoff DM, Watt G. Prevalence of relative bradycardia in Orientia tsutsugamushi infection. Am J Trop Med Hyg. 2003;68(4):477-479.
- Lai CH, Huang CK, Weng HC, et al. Clinical characteristics of acute Q fever, scrub typhus, and murine typhus with delayed defervescence despite doxycycline treatment. Am J Trop Med Hyg. 2008;79(3):441-446.
- Jung LY, Jeon M, Choi SH, Hwang JH, Lee CS, Rhee KS. Relative Bradycardia in Scrub Typhus. Am J Trop Med Hyg. 2017;97(5):1316-1318. doi:10.4269/ajtmh.17-0259
- Paixão GMM, Nunes MCP, Beato BDVG, et al. Cardiac Involvement by Yellow Fever(from the PROVAR+ Study). Am J Cardiol. 2019;123(5):833-838. doi:10.1016/j.amjcard.2018.11.032
- de Ávila RE, José Fernandes H, Barbosa GM, et al. Clinical profiles and factors associated with mortality in adults with yellow fever admitted to an intensive care unit in Minas Gerais, Brazil. Int J Infect Dis. 2020;93:90-97. doi:10.1016/j.ijid.2020.01.039
- Arif, S., Ahmed, H., Khokon, K., Azad, A., & Faiz, M. (1). Dengue Haemorrhagic Fever with Bradycardia. Journal of Medicine, 10(1), 36-37. https://doi.org/10.3329/jom.v10i1.2004
- Lateef A, Fisher DA, Tambyah PA. Dengue and relative bradycardia. Emerg Infect Dis. 2007;13(4):650-651. doi:10.3201/eid1304.061212
