
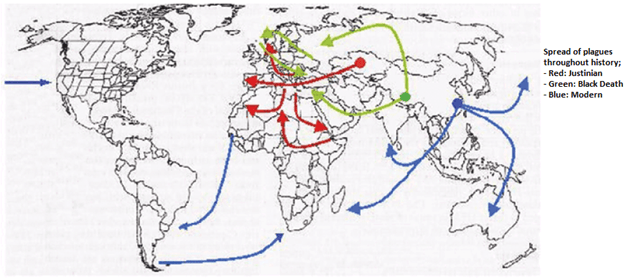
The history of plague and its place in human history is difficult to argue. There are 3 major pandemics that are attributed to the organism Yersinia Pestis:
- The “Justinian” Plague during the Byzantine Empire
- The “Black Death” during Medieval Europe
- The “Third Pandemic” that began in the late 19th Century and likely ongoing until today
Between those major pandemics, there were also small epidemics that occurred in various areas of the word, including an epidemic Germany, England, France, Switzerland, Russia, and Egypt from 1603-1611, a set of epidemics in Africa, Turkey, Poland, Austria, Germany, England, and the Netherlands from 1663-1611, as well as an outbreak in China in 1855.
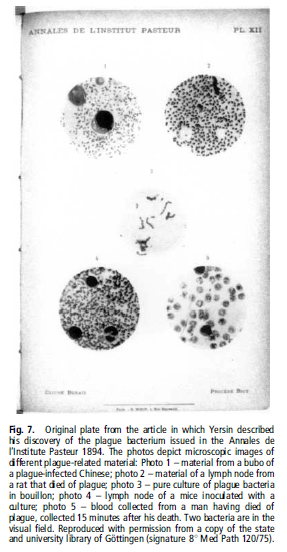
When the Third Plague reached Hong Kong in 1894, the Japanese and the French governments sent out microbiologist to explore the new plague. The Japanese sent a microbiologist by the name of Shibasaburo Kitasato, while the French sent out Alexandre Yersin. Both attempted to discover the pathogen underlying the plague and Kitasato published his findings first in the Lancet. Yersin’s findings were more found to be more accurate, however, including describing the organism as a gram negative and non-motile, contradicting Kitasato:
The organism has undergone many names, including
- Bacterium pestis
- Bacillus pestis
- Pasteurella pestis
- Yersinia pestis (since 1970)
It is believed the organism was originally an enteric organism and evolved from Yersinia pseudotuberculosis over ~20,000 years to become a flea-vector pathogen. During this time, it has acquired multiple virulence factors that distinguish it from Y. pseudotuberculosis:
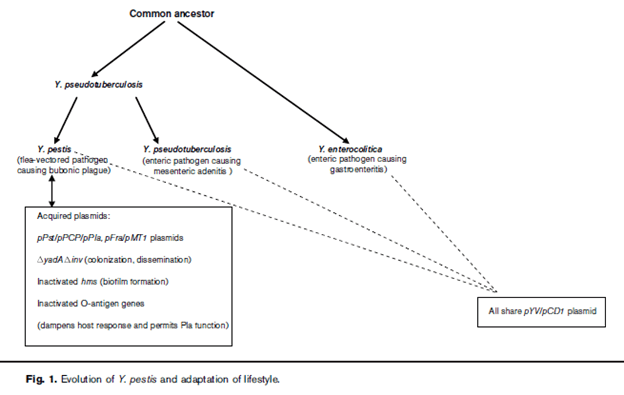
3 strains of Y.pestis have been identified, including Antigua, Orientalis, and Medievalis. Orientalis strains seems to be the cause of the third pandemic.
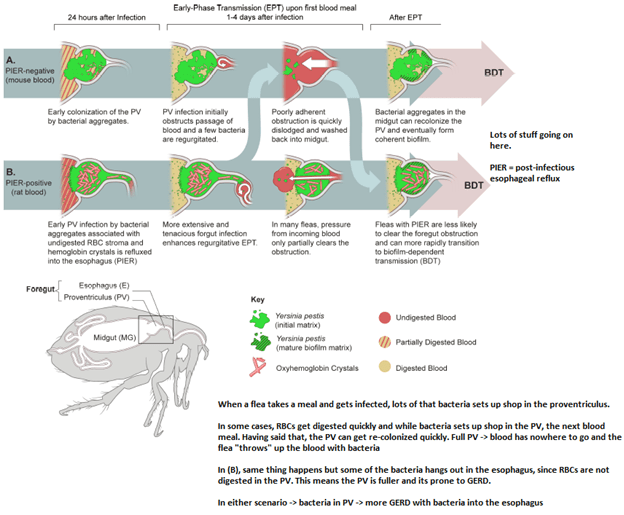
So how does the mighty flea able to wreck such havoc? Unlike mosquitoes, Y. Pestis actually causes some damage to the flea:
The Justinian Plague
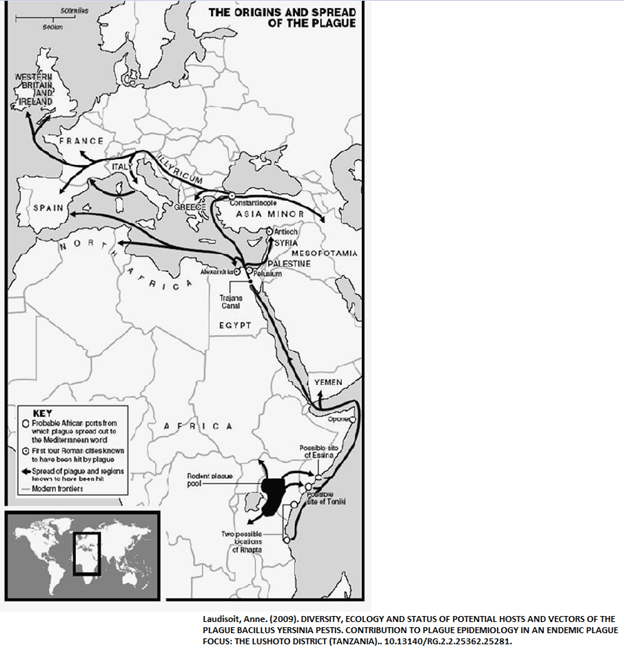
Named after the emperor of the Byzantine empire, or the Eastern Roman empire, it originated around 532 in Northern African and spread through the Middle East and Mediterranean basin. The plague reached the city of Constantinople and Greece around 541/543 and according to Procopius of Caesarea (aka the guy who stuck around the general Belisarius and wrote everything about Justinian’s reign), the plague may have killed around half of the inhabitants of the Byzantine Empire by the year 565. Though again, this is the guy who also wrote a book called “Secret History” about how Justinian was a literal demon…so take that figure with a grain of salt.
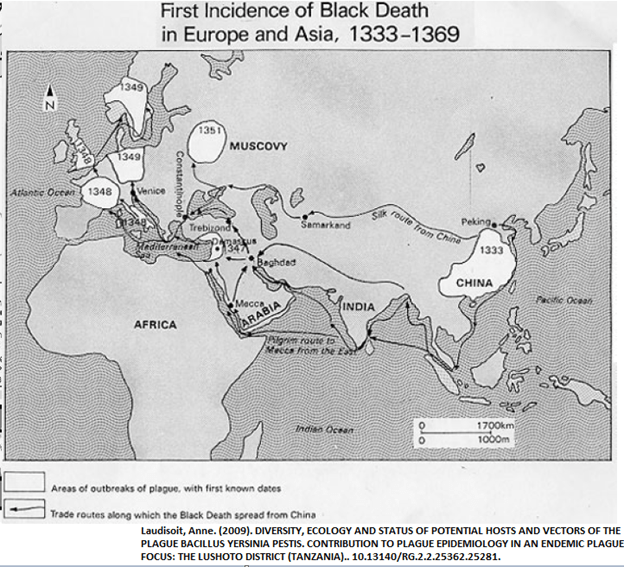
The Black Plague
This is the more well-known plague. It is believed the second plague began to spread from the Himalayas westward along three major trade routes (including the Silk Road…not the deep web site) from 1332 to 1346. Once it was introduced to Europe in 1347, several epidemics began to prop up during the next few years. During this time, it is believed that in Venice 100,000 people died, 50,000 to 80,000 in Paris, 100,000 in London, and at least 40,000 in Genoa. By the end of 1350, it is believed the plague killed roughly 15 to 23.5 million Europeans. In the centuries afterwards, the plague would become a sporadic epidemic, but not to the scale of the Black Death.
The Third Plague
This one probably originated in the Chinese providence of Yunnan around 1855, with local outbreaks occurring until the plague reached Hong Kong in 1894. Since then, the epidemic spread quickly throughout the world, landing in Calcutta and Bombay by 1896 and to San Francisco in 1899. Since then, the natural distribution of plague has expanded to nearly every continent except Antarctica. Currently, the Southwestern US remains an endemic region for plague following the introduction of the plague into urban populations in the late 19th century, including port cities such as Seattle, New Orleans, Galveston, and Pensacola. In the early 1900s, plague had been spread from rats to squirrels and by 1938, cases of plague had spread to prairie dogs in New Mexico. Since then, most of the cases have occurred in New Mexico, Arizona, Colorado, and California.
So why the history lesson on Plague since I will likely never see it? There were a few articles a few months ago on plague in CID so I figured it would be a good time to go over them:
Nelson, Christina A., et al. “Antimicrobial Treatment of Human Plague: a Systematic Review of the Literature On Individual Cases, 1937-2019.” Clinical Infectious Diseases : an Official Publication of the Infectious Diseases Society of America, vol. 70, no. Supplement_1, 2020, pp. S3-S10.
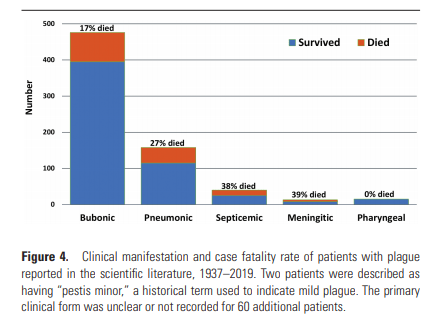
The first one is a review of cases of plague (Y. pestis) from 1937-2019. They included 762 cases, with the most common manifestation being Bubonic plague (62.5%), followed by pneumonic (20.7%) and septicemic (5.2%). The overall case fatality rate was 20.1%. The breakdown per disease are as follows.
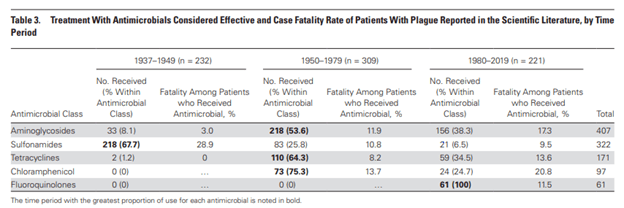
The most common antibiotic classes used included aminoglycosides (53.4%), usually streptomycin (42.4%), sulfa (23%), Tetracyclines (22.4%), and FQs (8.0%).

Notably, sulfas and chloramphenicol were associated with the highest mortality. This pattern held true even when breaking down each major disease classification:

Having said that, it seems that this was driven by the fact this was during the early stages of antibiotic therapy in general (i.e. we didn’t really have much in the 1940s or 1950s, and critical care has advanced a lot since then, like I think we have patients like 30 of peep if we had vents).
Either way, chloramphenicol still sucks. Further they found that 13.0% of 193 patients who were treated within 2 days of symptom onset died, compared with 28.1% of 139 patients who were treated ≥ 3 days after symptom onset died. Fatality differences among patients treated within 2 days of symptom onset compared with those treated ≥ 3 days after symptom onset were also seen for those bubonic (9.0% fatality vs. 24.0% fatality), pneumonic (20.0% vs. 33.3%), and septicemic plague (18.2% vs. 55.6%). They didn’t find any difference for combination therapy vs monotherapy, though those who had the combination of aminoglycoside + fluroquinolone had a 20% case fatality rate vs ~5% of those with FQ monotherapy. Aminoglycoside + sulfa had a 5.5% CFR vs sulfa alone, having a CFR of 30.1%
Godfred-Cato, Shana, et al. “Treatment of Human Plague: a Systematic Review of Published Aggregate Data On Antimicrobial Efficacy, 1939-2019.” Clinical Infectious Diseases : an Official Publication of the Infectious Diseases Society of America, vol. 70, no. Supplement_1, 2020, pp. S11-S19.
The second review found 2631 cases from 1939-2019. Again, the most common type of plague was 93.6% had bubonic plague, 5.9% had pneumonic, and 0.5% had septicemic plague. No meningitic plague was reported. The overall CFR here was 13.6% (bubonic 14.2%, pneumonic 31.1%, and septicemic 20%). As contrast to the other study, the found that combination therapy yielded a CFR of 6.9%, compared to monotherapy withy 13.1%.

The antibiotics that were associated with higher mortality were sulfa drugs (20%) and penicillin (75%).
TL;DR – lots of the data is difficult to interpret since much of the mortality from early plague may have been due to lack of advances in critical care. Having said that:
- Aminoglycosides tend to be the preferred agent, with gentamicin having replaced streptomycin
- Doxycycline as adjunct is also a reasonable option
- Quinolones tend to be second line if you cannot use either of the above agents
- TMP-SMX may be a viable option but not preferred
References:
Williamson, E D., and P C F. Oyston. “The Natural History and Incidence of Yersinia Pestis and Prospects for Vaccination.” Journal of Medical Microbiology, vol. 61, no. Pt 7, 2012, pp. 911-918.
Zietz, Björn P., and Hartmut Dunkelberg. “The History of the Plague and the Research On the Causative Agent Yersinia Pestis.” International Journal of Hygiene and Environmental Health, vol. 207, no. 2, 2004, pp. 165-78.
Bland, David M., et al. “Infectious Blood Source Alters Early Foregut Infection and Regurgitative Transmission of Yersinia Pestis By Rodent Fleas.” PLoS Pathogens, vol. 14, no. 1, 2018, pp. e1006859.
Laudisoit, Anne. (2009). DIVERSITY, ECOLOGY AND STATUS OF POTENTIAL HOSTS AND VECTORS OF THE PLAGUE BACILLUS YERSINIA PESTIS. CONTRIBUTION TO PLAGUE EPIDEMIOLOGY IN AN ENDEMIC PLAGUE FOCUS: THE LUSHOTO DISTRICT (TANZANIA).. 10.13140/RG.2.2.25362.25281.
