The duration of therapy in vertebral osteomyelitis tends to be prolonged, usually 6 weeks of more. If there is anything to take away from this, is that at least 6 weeks of antibiotics for vertebral osteomyelitis is usually fine, but there are certain exceptions that may warrant longer duration of therapy.
Some well cited data include a 10 year retrospective cohort (1) evaluated risk of recurrence in patients treated for 6 weeks with antibiotics or greater than 6 weeks and found no overall difference in the rate of recurrence in those patients treated for >6 weeks or 6 weeks
Further data comes from a relatively large study in the Lancet (2), which is likely the largest study of its kind. This French multicenter, open-label, non-inferiority RCT evaluated the effectiveness of antibiotics for 6 weeks vs 12 weeks for vertebral osteomyelitis. Patients were followed up to 12 months for a primary outcome of non-inferiority comparison of cure at 1 yr. In this study, in the ITT analysis, 160/176 (90.9%) of the 6 week group achieved a cure compared to 159/175 (90.9%) of those in the 12 week group (Difference in proportion of patients +0.1 95% CI -6.2 to 6.3). This held true in the per protocol analysis (137/146, 93.8% in 6 week group vs 132/137, 96.4%, 95% CI -8.2 to 2.9). The average length of IV therapy was roughly 14 days in both groups. One thing to note here is that only a few percentage of patients actually had abscesses (19%) and that, while about 41% of the patients enrolled in the trial had Staph aureus, only a grand total of 8 patients had MRSA. Further, the guidelines in France advocate for the use of FQ and rifampin as first line therapies; IV antibiotics tend to be oxacillin or other PCN.
Another observational cohort study from Korea evaluating 345 patients with hematogenous vertebral osteomyelitis and looking at risk factors for either microbiological and/or clinical recurrence (2). A univariate and multivariate analysis showed that ESRD, MRSA infection, and paravertebral abscesses were all associated with a high risk of recurrence:
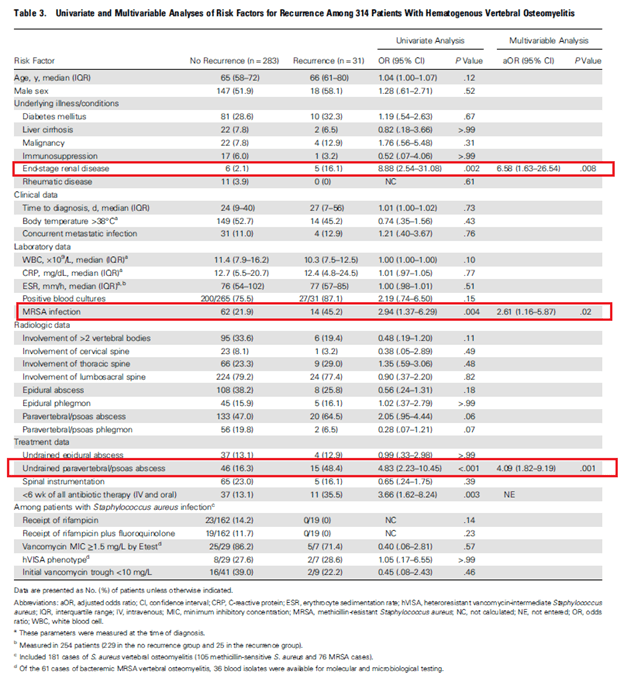
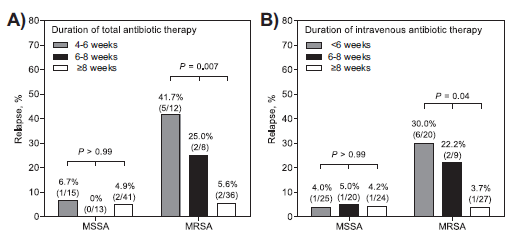
Further, they saw that in those with high-risk features, increasing total duration of antibiotic therapy (Both PO and IV) correlated with decreased recurrence. For 4-6 weeks, 34.8 experienced recurrence, 29.6% experienced recurrence in the 6-8 week group in 9.6% of those who got >8 weeks of antibiotics had recurrence (p-value 0.002). Those with low risk recurrence, the difference was less so but still significant (12% in the 4-6 week group, 6.3% in the 6-8 week group, and 2.2% >8 week group, p-value 0.02):
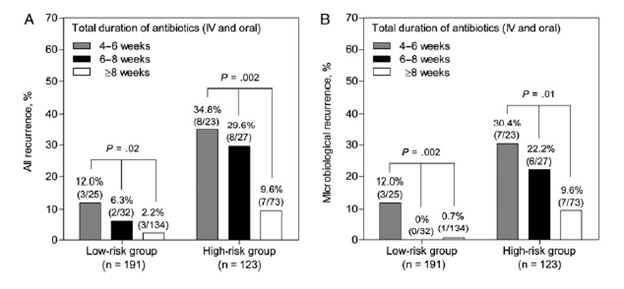
In low risk patients, those who received a total of <6 weeks of IV antibiotic had significant higher recurrences compared to those who got at least 6 weeks or more.
This was similar to those patients with high risk of recurrence and using an 8 week cut off for antibiotics.

This suggest that those patient with MRSA have a higher risk of recurrence up front and they should receive a longer course of antibiotics. Indeed, a 2013 observational study evaluated outcomes of vertebral osteomyelitis in 139 patients (4), 77 (55.4%) of which were due to MSSA and 62 (44.6%) due to MRSA. Those with MRSA vertebral osteomyelitis were older, had hospital acquire infections, and were more likely to have malignancy, T2DM, and infected intravascular access:
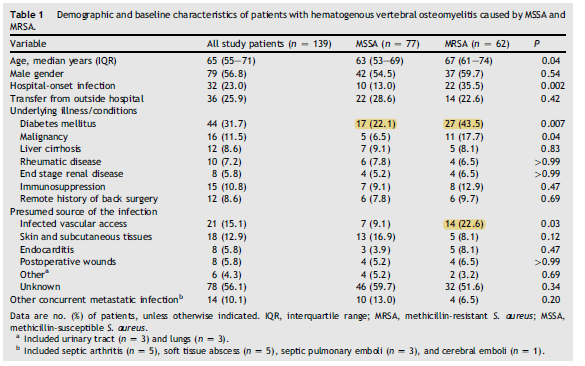
Overall, patients with MRSA were more likely to have longer hospital stays, persistent bacteremia, and higher frequency of relapse:
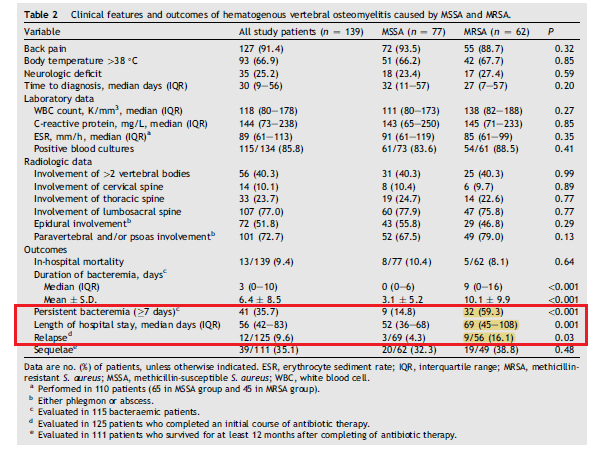
In univariate analysis, both MRSA (OR 4.21, 95% CI 1.08-16.40, p-value 0.04) and therapy <8 weeks of length (OR 3.65, 95% CI 1.04 – 12.88, p-value 0.04) were associated with relapse. In multivariate analysis, both MRSA (OR 4.83, 95% CI 1.2-19.44, p-value 0.03)and length <8 weeks (OR 4.21 , 95% CI, 1.15-15.44, p-value 0.03) were still significant factors in relapse and longer duration of therapy in MRSA cases lead to lower relapse rates:
Intravenous antibiotics were given for a median duration of 50 days, ranging from 34-64 days overall.
Further data comes from another Korean study (….from the same principal investigator…hmm) on therapeutic outcomes in patients who underwent spinal surgery (5). In this retrospective observational cohort, 153 patients were evaluated for risk of death and recurrence following spinal surgery (either debridement +/- implantation of a device such as a rod, etc). While only 53% of patients had Staph aureus (and of those with staph, 38% had MRSA), they found a correlation between length of antibiotic therapy and risk of recurrence, regardless of surgical plan:
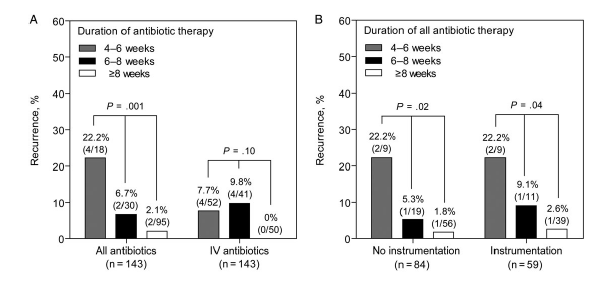
This data (mostly from Korea, from the same guy), suggests that MRSA should receive a minimum of 8 weeks of antibiotic therapy (can step down to PO). What about data for other organisms? For instance, gram negative rods? (since Baston’s Plexus can lead to a vertebral osteomyelitis). Unfortunately, due ot the relatively rareity, ther is litte data dedicated to GNR vertebral osteomyelitis. One study (6) found that in those with GNR vertebral osteomyelitis, the rates of recurrence also differ by antibiotic length of therapy:40% in the 4-6 week group, 33.3# in the 6-8 week group, and 2.1% in the group treated for >8 weeks (p value 0.002)
This suggest that, in general, 6 weeks of antibiotic therapy should suffice for most patients, however those who benefit from at least 8 weeks include those with MRSA (or other resistant infections), high risk of recurrence such as dialysis patients or those whose central access cannot be removed, and abscesses. Seems the sweet spot for most of these infections tends to be a minimum of 6 weeks with possibly extension to 8 weeks in some cases, if not most of the cases. Those with MRSA as the etiology would benefit from a total of more than 8 weeks of antibiotics, perhaps 12.
What about IV vs PO?
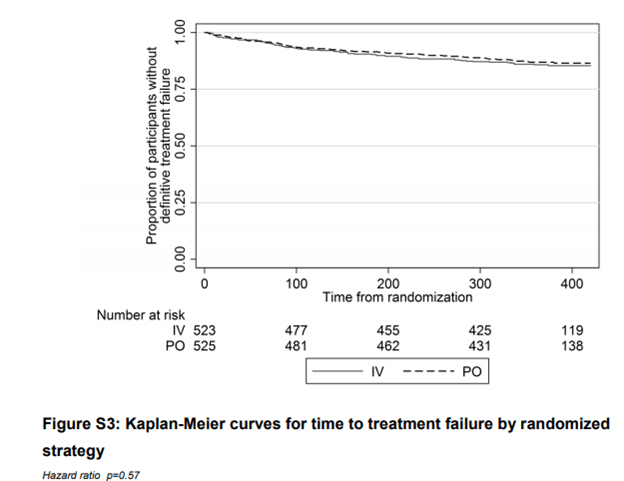
The largest multicenter, non-blinded, randomized controlled trial comparing IV to PO therapy in bone infections (7) evaluated 1015 patients to either an all IV strategy or stepdown to PO within 5 days. Primary outcome here was treatment failure at one year. They only had a total of 72 patients with spinal infections (37 in the IV group and 35 in the PO group). While the overall number of vertebral infections is small, in the grand scheme of other infections, it is quite a large number of patients. The Kaplan-Meyer curve for all patients is as follows:
Most of the oral antibiotics used included doxycycline, quinolones (usually cipro), oral penicillin’s. In a retrospective study (8) of 61 patients with vertebral osteomyelitis, 43 patients (72%) were switched to PO antibiotics after a median time of IV therapy of 19 days (14-27 days). At one year follow up, only 2 patients had died from metastatic carcinomas and none had recurrent disease or relapse. By far, the most common antibiotic being given were quinolones alone or in combination with either rifampin or clindamycin.
TL;DR
- In uncomplicated infections (i.e. no abscess, resistant infections such as MRSA, no lines), a minimum of 6 weeks of total antibiotics seems to be a safe option
- If there is an uncomplicated infection, patients can be stepped down to a PO antibiotic within 1-2 weeks (note this needs to be a highly bioavailable antibiotic)
- If there is a risk of relapse (i.e. co-morbidities, resistant infection, abscess), at least 8 weeks and up to 12 weeks of therapy total would be the best bet (how this is spilt is typically up to personal preference. Having said that, if you have hematogenous MRSA, you are essentially stuck treating presumptive endocarditis even with a negative echo. So minimum of 6 weeks of IV therapy and rest of PO tends to be a reasonable approach here).
References:
- Roblot, F & Besnier, J.M. & Juhel, L & Vidal, C & Ragot, S & Bastides, Fred & Moal, G & Godet, C & Mulleman, Denis & Azaïs, I & Becq-Giraudon, B & Choutet, P. (2007). Optimal Duration of Antibiotic Therapy in Vertebral Osteomyelitis. Seminars in arthritis and rheumatism. 36. 269-77. 10.1016/j.semarthrit.2006.09.004.
- Bernard, Louis, et al. “Antibiotic Treatment for 6 Weeks Versus 12 Weeks in Patients With Pyogenic Vertebral Osteomyelitis: an Open-label, Non-inferiority, Randomised, Controlled Trial.” Lancet (London, England), vol. 385, no. 9971, 2015, pp. 875-82.
- Park, Ki-Ho, et al. “Optimal Duration of Antibiotic Therapy in Patients With Hematogenous Vertebral Osteomyelitis at Low Risk and High Risk of Recurrence.” Clinical Infectious Diseases : an Official Publication of the Infectious Diseases Society of America, vol. 62, no. 10, 2016, pp. 1262-1269.
- Park, Ki-Ho, et al. “Clinical Characteristics and Therapeutic Outcomes of Hematogenous Vertebral Osteomyelitis Caused By Methicillin-resistant Staphylococcus Aureus.” The Journal of Infection, vol. 67, no. 6, 2013, pp. 556-64.
- Park, Ki-Ho, et al. “Therapeutic Outcomes of Hematogenous Vertebral Osteomyelitis With Instrumented Surgery.” Clinical Infectious Diseases : an Official Publication of the Infectious Diseases Society of America, vol. 60, no. 9, 2015, pp. 1330-8.
- Park KH, Cho OH, Jung M, et al. Clinical characteristics and outcomes of hematogenous vertebral osteomyelitis caused by gram-negative bacteria. J Infect. 2014;69(1):42-50. doi:10.1016/j.jinf.2014.02.009
- Li, Ho-Kwong, et al. “Oral Versus Intravenous Antibiotics for Bone and Joint Infection.” The New England Journal of Medicine, vol. 380, no. 5, 2019, pp. 425-436.
- Babouee Flury et al.: Is switching to an oral antibiotic regimen safe after 2 weeks of intravenous treatment for primary bacterial vertebral osteomyelitis? BMC Infectious Diseases 2014 14:226.
