
This post will not cover the clinical course or risk factors. We’ll be going over the direct fluorescence antibody, PCR, as well as the elusive beta-D glucan as well as taking a brief look at the original ways we used to diagnose PJP (or in some places, how they still diagnose it.
In the days of cancer and steroids, the way to diagnose PJP was usually at autopsy or staining with one of several methods that we do not use routinely today, including methenamine silver, Giemsa, Celluflour, Pap (yep), etc.. These methods tend to be fairly sensitive and specific, but of course this depends on who is taking a look at the slide (see below). In other words, the B-team will likely either overcall something or miss other slides.
Here is a table highlighting the relative specificities of each stain, in both induced sputum and BAL (1).
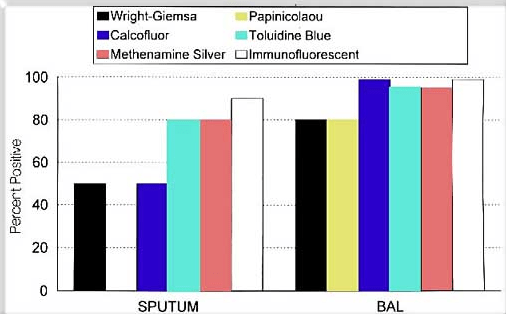
- Wright-Giemsa stain – straight forward, no fixation required, but you can confused clumped Neutrophils for PJP. Can detect any stage of the Pneumocystis
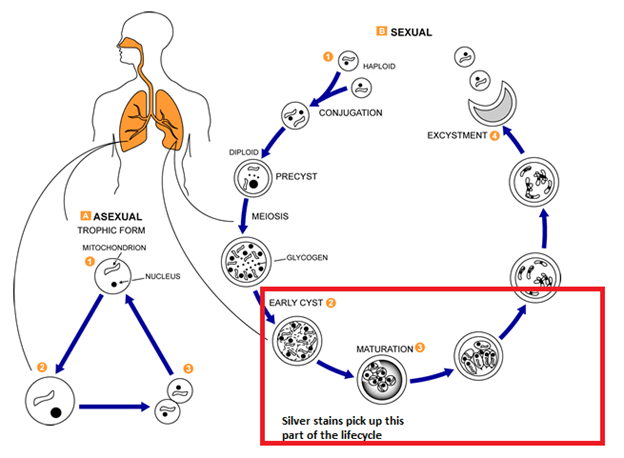
- Silver stains (Methenamine Silver, Toluidine blue) – “gold standard” for a while. They stain the wall of the cystic form and can be used on imprint smears or tissue sections. But takes for ever.
- Diff Quick – a more “quick” form of a silver stain. One disadvantage here is that you can confuse PJP For crypto or
- Pap smear- detects foamy eosinophilic infiltrate
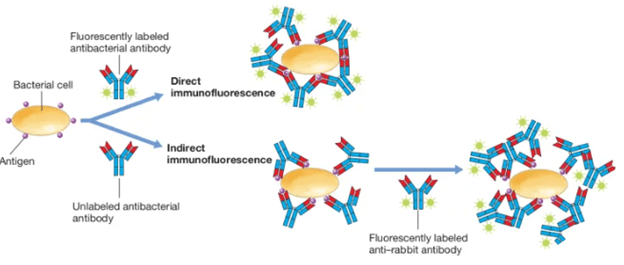
Further, in non-HIV patients, these methods tend to be less sensitive (5), as the idea was there is less organisms in those who are not as immunosuppressed to catch in a stain. In the 70s, direct fluorescence antibody was implemented for the diagnosis of PJP. This was essentially a tagged antibody that would shine a light when it found its antigen:
One of the early studies (2) found that DFA sensitivity was 82% and specificity was 100% when compared to autopsy reports. When compared to clinical “gestalt” the sensitivity was roughly 91% but specificity dropped to 57%. A later study (3) found that when compared to the GMS stain, DFA had a sensitivity of 77% overall when pooling BAL and induced sputum samples together. Note that in this sample, 66/104 were HIV positive. The specificity, however, was >99%. In HIV patients, the sensitivity of spectorated (i.e. whatever you cough up) sputum was 71% while specificity was 60% when compared to PCR (4). In another prospective study (5) study comparing DFA with calcofluor white found that both were reasonable comparable, but DFA performed better with expectorated sputum.
A review (12) suggested that the sensitivity of IFA was 92%, compared to that of Giemsa stain (76%) and T.blue stain (80%). Further, Giemsa staining was found to be the least sensitive when compared to DFA and IFA; however DFA was the least specific.
TL;DR – stains are great if you have an experienced pathologist looking at them. DFA and IFA takes a lot of the work out, and has greater sensitivity overall when compared to stains but may have lower specificity.
PCR:
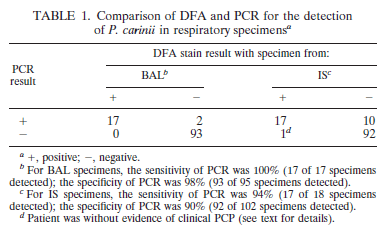
This is the more common testing you will find out there. As such, a lot of the literature over the past few years has focused on this modality. This was developed as there was concern about lack of sensitivity in non-HIV Patients. One early study (6) comparing PCR and DFA found that in both induced sputum and BAL specimens the sensitivity and specificity was quite high, both reaching either 90% or above:
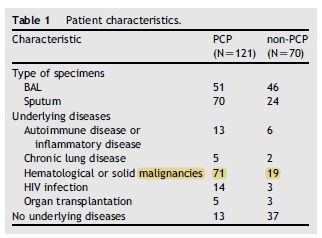
The authors do not give details as to who was HIV positive or not. Further data (7) in HIV Positive patients suggested that the specificity of induced sputum PCR and BAL PCR was nearly 100%, while the sensitivity was 100% for BAL PCR specimens and 86% for induced sputum. This contrasts with the sensitivity of 43% for indirect immunofluorescence. In a more heterogeneous population (8), the impact of PCR for diagnosis seems to change. In this study, 121 patients with PJP and 70 patients without PJP had BAL or IS evaluated for the utility of PCR as a diagnostic modality. PJP patients were those who had clinical characteristics and responded to PJP therapy. Table 1 shows how heterogeneous these patients were:
Further, the use of prophylaxis was not widespread. Pooling all the data:
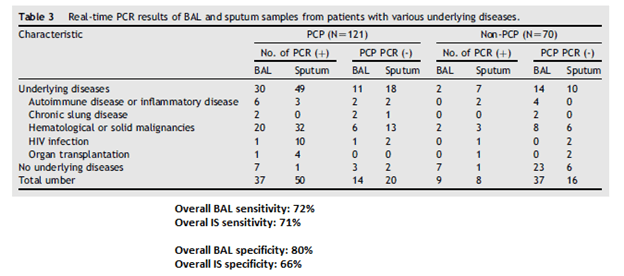
The authors do mention “In this study, 14 (27%) of the 51 BAL specimens and 20 (29%) of the 70 sputum samples from patients with PCP were PCR negative. Among these 34 patients, 12 were
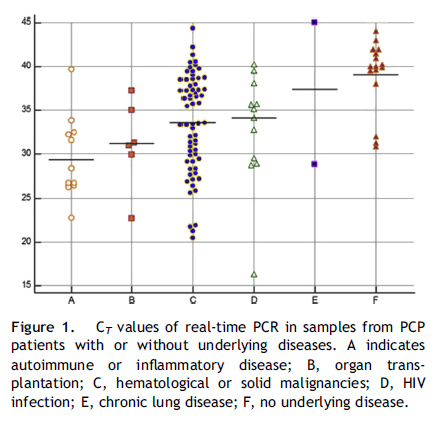
treated or had prophylaxis for PCP. Such treatments might have cleared P. jirovecii infections or prevented the development of PCP.” One of the interesting things they did was they evaluated the cycle threshold for PJP in patients with different diseases. Not surprisingly, those who had no underlying immunosuppression, had a higher cycle threshold (i.e. lower fungal load), suggesting that sputum from full blown AIDS patients or bad heme malignancies are more sensitive due to the higher burden of disease.
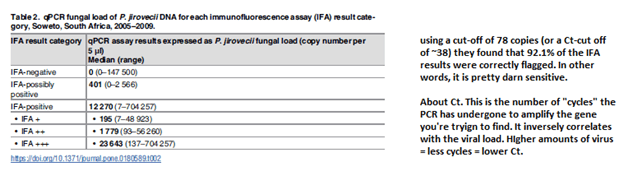
Another study compared the sensitivity and specificity of qPCR vs indirect immunofluorescence in a population of HIV positive individuals (9). Using the IFA as the “gold standard” they found the sensitivity and specificity was 98.2% and 70% respectively. The PPV and NPV were 80.1% and 96.5%, respectively. In other words, a negative in a low risk patient may be a true negative:

Further, they evaluated what the cut off for the number of copies needed in the PCR for it to flag positive (i.e how many copies do you need to have in order to have a “true” positive PCR) when compared to IFA.
One of the most complete meta-analysis (10) compared the performance of PCR across different patient populations as well as different modalities (i.e. oropharyngeal wash, BAL, IS). They found that, across all populations in those who had a high probability of PJP, the PCR performed quite well:
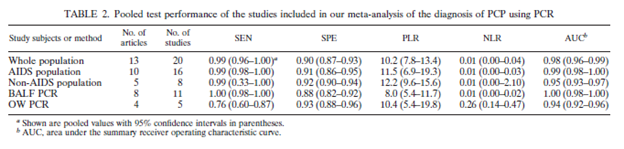
Having said that, the groups were very heterogeneous and there is no indication as to when PJP prophylaxis was used (which can impact the sensitivity of each modality). A recent meta-analysis (11) on the use of PJP PCR on BAL was done which showed a fairly high pooled sensitivity and specificity:

This suggest that, by far, PJP PCR is largely sensitive and specific for the diagnosis of PJP in the right patient population. This applies to both HIV and non-HIV patients with the right risk factors (I.e immunosuppressed liquid malignancy patients and s/p SOT patients). Having said that, it seems that those with HIV tend to have higher fungal loads. For instance, one review (12) suggested that AIDS patients had a diminished inflammatory response when compared to immunosuppressed patients without AIDS, noting that the median neutrophils in AIDS patients was 2.3% when compared to the 18.5% in non-AIDS patients in lower respiratory tract samples.
Another earlier study (20) evaluating PJP fungal load and neutrophils in BAL samples from HIV and non-HIV patients found that HIV patients have both higher fungal loads and lower neutrophil counts. They also found that arterial oxygen tension was significantly higher in AIDS patient than non-AIDS patient, suggesting that neutrophils may play a role in the pathophysiology of hypoxemia (hence the steroid issue). Indeed, this may explain why PJP in HIV patients tend to be more of an indolent disease while patients with non-HIV types of immunosuppression tend to come in crashing with hypoxemic respiratory failure much more quickly (21).
Of note, when dealing with PCR, one of the things to watch out for is false positives. HIV patients can be colonized with PJP (again, going back to what we mentioned above; less neutrophils -> less inflammation and more fungus). In one study (13), 8 patients who were asymptomatic for PJP tested positive by PCR. Six of these ended up becoming symptomatic within a year, suggesting that 1) PCR can pick up colonization and 2) those who are colonized can become symptomatic. Further, another study found that a significant portion (46%) of patients tested for PCP PCR had discordant results when comparing IS/trach aspirates vs BAL (14). The authors theorized this was due to the BAL not going to densely infiltrative (?) areas of the lung. Whatever that means
TL;DR – PCR seems to be highly sensitive and specific, both being greater than 90% (though not 100%). However, it can also pick up colonization in HIV patients.
To summarize the above
- Stains are ok in general, very specific but you need good people to read them
- PCR is amazing; good sensitivity/specificity (both >90%) but there is a risk of catching “colonization.”
- BAL > IS > expectorated. If possible, I would err on just inducing sputum (I know, its annoying to the patient) as this will allow you the greatest sensitivity.
- PCR > stains.
- There tends to be more PJP in HIV-individuals compared to other immunosuppressed folks
BD Glucan
Given how HIV-negative patients who are still immunosuppressed are still susceptible to PJP, and how HIV status affects the sensitivity of PJP PCR, it stands to reason we would look for another avenue for diagnosis (That does not involve biopsing or bronching someone). Enter BD glucan! There are several advantages of BD glucan, and it tends to performed differently in both HIV negative and positive population.
In a prospective observational study composed of mostly SOT patients (all HIV negative; 15), those who were PJP Positive had significantly higher BD glucan:
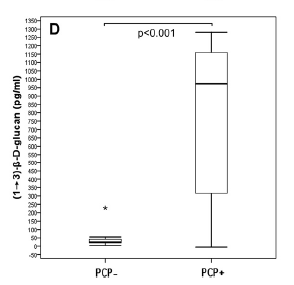
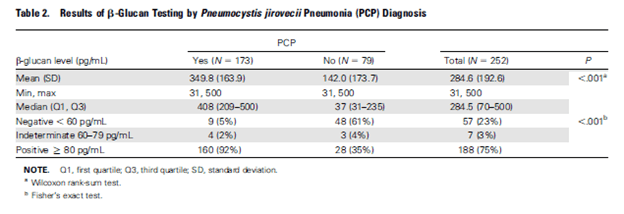
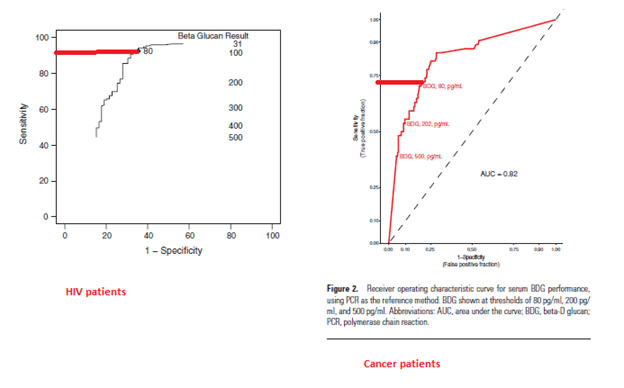
A 2011 study evaluated 252 patients with HIV for the utility of BD glucan and PJP (18). By far, those with PJP had significantly higher levels of BD glucan:
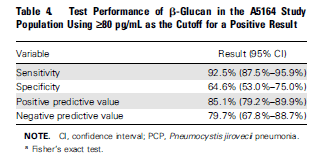
At a cutoff value of >80 pg/mL, BD glucan had fairly good sensitivity but ok specificity:
In a study of hematological malignancy patients (19), 53 patients were retrospecrtively evaluated for PJP pneumonia with both PJP PCR and BD glucan. The sensitivity and specificity are highlighted below:
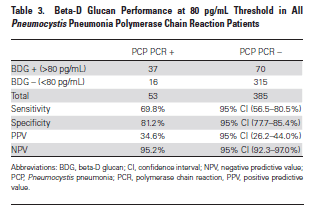
In putting the ROC of both studies side by side:
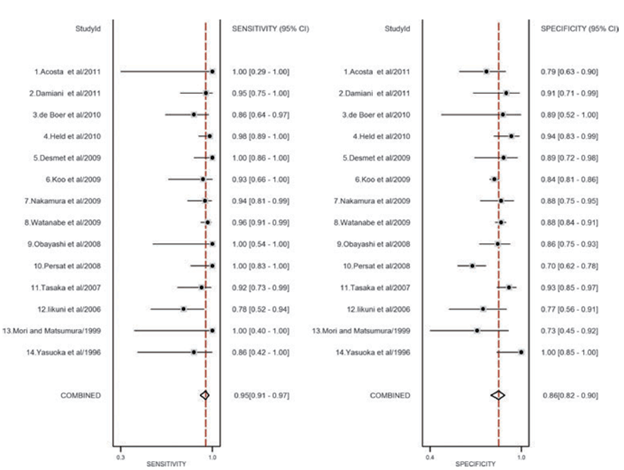
In a meta-analysis (16), consisting of mostly retrospective studies as well as a mix of immunosuppressive states, the overall sensitivity and specificity seems to be fairly high:
Another meta-analysis had similar findings overall for HIV and non-HIV patients in terms of sensitivity, but lower specificity (17):
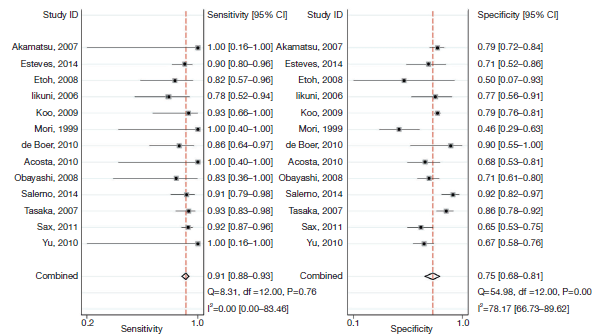
When breaking down this a bit further, the HIV sensitivity for BD glucan was a bit higher when compared to that of non-HIV Patients:

So BD glucan is a fairly sensitive but not terribly specific non-invasive method of diagnostics. It may be helpful in those patients who may be colonized and the clinical syndrome is not suggestive of PJP (though, if someone is immunocompromised enough, they may have risk of other fungal infections). Either way, by itself maybe not the best test but in conjunction with clinical data it is helpful.
TL;DR
- PJP is difficult to culture. BAL > Induced sputum if you are able to get it. PCR > stains, since it is more sensitive (though not nearly as specific).
- The sensitivity of all diagnostic modalities (PCR, stains, BD glucan) is higher in HIV population, given the higher burden of disease
- Note that certain HIV patients can be colonized with PJP.
- BD glucan is useful as an adjunct to clinical data as well as PCR (i.e. it can tell you if PJP PCR is a colonizer if BD glucan is negative or the real deal if positive).
References:
- Baughman RP, Liming JD. Diagnostic strategies in Pneumocystis carinii pneumonia. Front Biosci. 1998;3:e1-e12. Published 1998 Jan 1. doi:10.2741/a363
- Lim, S K., et al. “Direct Fluorescent-antibody Method for the Diagnosis of Pneumocystis Carinii Pneumonitis From Sputa or Tracheal Aspirates From Humans.” Applied Microbiology, vol. 27, no. 1, 1974, pp. 144-9.
- Wolfson JS, Waldron MA, Sierra LS. Blinded comparison of a direct immunofluorescent monoclonal antibody staining method and a Giemsa staining method for identification of Pneumocystis carinii in induced sputum and bronchoalveolar lavage specimens of patients infected with human immunodeficiency virus. J Clin Microbiol. 1990;28(9):2136-2138.
- Choe, Pyoeng Gyun, et al. “Diagnostic Value of Direct Fluorescence Antibody Staining for Detecting Pneumocystis Jirovecii in Expectorated Sputum From Patients With HIV Infection.” Medical Mycology, vol. 52, no. 3, 2014, pp. 326-30.
- Aslanzadeh, J, and P S. Stelmach. “Detection of Pneumocystis Carinii With Direct Fluorescence Antibody and Calcofluor White Stain.” Infection, vol. 24, no. 3, 1996, pp. 248-50.
- Caliendo, A M., et al. “Performance of a PCR Assay for Detection of Pneumocystis Carinii From Respiratory Specimens.” Journal of Clinical Microbiology, vol. 36, no. 4, 1998, pp. 979-82.
- Roux, P, et al. “Usefulness of PCR for Detection of Pneumocystis Carinii DNA.” Journal of Clinical Microbiology, vol. 32, no. 9, 1994, pp. 2324-6.
- Yang, Shu-Li, et al. “Diagnosis of Pneumocystis Pneumonia By Real-time PCR in Patients With Various Underlying Diseases.” Journal of Microbiology, Immunology, and Infection = Wei Mian Yu Gan Ran Za Zhi, 2019.
- Moodley, Bhavani, et al. “Comparison of Quantitative Real-time PCR and Direct Immunofluorescence for the Detection of Pneumocystis Jirovecii.” PloS One, vol. 12, no. 7, 2017, pp. e0180589.
- Lu, Yuan, et al. “PCR Diagnosis of Pneumocystis Pneumonia: a Bivariate Meta-analysis.” Journal of Clinical Microbiology, vol. 49, no. 12, 2011, pp. 4361-3.
- Fan, Li-Chao, et al. “Evaluation of PCR in Bronchoalveolar Lavage Fluid for Diagnosis of Pneumocystis Jirovecii Pneumonia: a Bivariate Meta-analysis and Systematic Review.” PloS One, vol. 8, no. 9, 2013, pp. e73099.
- Turner, D, et al. “Induced Sputum for Diagnosing Pneumocystis Carinii Pneumonia in HIV Patients: New Data, New Issues.” The European Respiratory Journal, vol. 21, no. 2, 2003, pp. 204-8.
- Elvin K, Olsson M, Lindman C, Bjorkman A. Detection of asymptomatic Pneumocystis carinii infection by polymerase chain reaction: predictive for subsequent pneumonia. AIDS 1996; 10: 1296–1297.
- Pennington, Kelly, et al. “Positive Pneumocystis Jirovecii Sputum PCR Results With Negative Bronchoscopic PCR Results in Suspected Pneumocystis Pneumonia.” Canadian Respiratory Journal, vol. 2018, 2018, p. 6283935.
- de Boer MG, Gelinck LB, van Zelst BD, et al. β-D-glucan and S-adenosylmethionine serum levels for the diagnosis of Pneumocystis pneumonia in HIV-negative patients: a prospective study. J Infect. 2011;62(1):93-100. doi:10.1016/j.jinf.2010.10.007
- Karageorgopoulos DE, Qu JM, Korbila IP, Zhu YG, Vasileiou VA, Falagas ME. Accuracy of β-D-glucan for the diagnosis of Pneumocystis jirovecii pneumonia: a meta-analysis. Clin Microbiol Infect. 2013;19(1):39-49. doi:10.1111/j.1469-0691.2011.03760.x
- Li, Wei-Jie, et al. “Diagnosis of Pneumocystis Pneumonia Using Serum (1-3)-β-D-Glucan: a Bivariate Meta-analysis and Systematic Review.” Journal of Thoracic Disease, vol. 7, no. 12, 2015, pp. 2214-25.
- Sax, Paul E., et al. “Blood (1->3)-beta-D-glucan as a Diagnostic Test for HIV-related Pneumocystis Jirovecii Pneumonia.” Clinical Infectious Diseases : an Official Publication of the Infectious Diseases Society of America, vol. 53, no. 2, 2011, pp. 197-202.
- Morjaria, Sejal, et al. “Clinical Performance of (1,3) Beta-D Glucan for the Diagnosis of Pneumocystis Pneumonia (PCP) in Cancer Patients Tested With PCP Polymerase Chain Reaction.” Clinical Infectious Diseases : an Official Publication of the Infectious Diseases Society of America, vol. 69, no. 8, 2019, pp. 1303-1309.
- Limper, A H., et al. “Pneumocystis Carinii Pneumonia. Differences in Lung Parasite Number and Inflammation in Patients With and Without AIDS.” The American Review of Respiratory Disease, vol. 140, no. 5, 1989, pp. 1204-9.
- Tasaka, Sadatomo. “Recent Advances in the Diagnosis and Management of Pneumocystis Pneumonia.” Tuberculosis and Respiratory Diseases, vol. 83, no. 2, 2020, pp. 132-140.
