
At any rate, at approximately one-quarter to twelve that night, I remember distinctly getting up from my chair and from the table, where my books lay, and taking off my suit coat. No sooner had I removed the left arm of my coat, than there was on the ventral aspect of my left wrist a sight which I shall never forget until I die. There greeted my eyes about fifteen or twenty bright red, slightly raised, hemorrhagic spots about 1 millimeter in diameter which did not fade on pressure and which stood defiant as if they were challenging the very gods of Olympus. … I took one glance at the pretty little collection of spots and turned to my sister-in-law, who was standing nearby, and calmly said: ‘I shall be dead within six months (1)
These are the descriptions of infective endocarditis from Alfred S. Reinhart, a Harvard medical student who was afflicted with the disease in 1931. He would unfortunately succumb to the illness in that same year, but his description of the illness, from his salvos of palpitations to his identification of embolic phenomena which included strokes, remain haunting. If there is any validation to the “second-year medical student syndrome” this is it. Since then, however, we have gotten much better at diagnosing infective endocarditis before death. The journey through this has been difficult, however. Allow me to take you through the initial definitions of endocarditis to the most well known, the modified Duke criteria.
Defining the Problem
Historically, the study of endocarditis has been difficult given the myriad of symptoms as well as the fact it can mimic other diseases. One of the first documented cases of endocarditis was described by Lazare Riviere, in a patient who presented with most likely atrial fibrillation and was found to have “round carbuncles” in the left ventricle, filling up to the aorta (2). Later on, Jean-Nicolas Corvisart described mitral valve endocarditis and introduced the term “vegetation.” William Senhouse Krikes described various cases of infective endocarditis with peripheral embolization, providing a window into the pathophysiological consequences of IE. The problem here, of course, is the diagnosis is not able to be done until autopsy, which is not ideal. Further, defining the type of endocarditis remained difficult given the variety of presentations. It wasn’t until Bill Olser’s Gulstonian lectures where he recommended the simplification of IE definitions, settling on simple (few symptoms) and malignant (prominent, destructive valvular lesions and several other symptoms, 3). He also made several descriptions into the pathological consequences in heart valves, and recommended the use of gram stain to identify the causative organism. Many of the phenomena that came to be associated with endocarditis bear his name (Osler nodes, anyone?). The definition of types of IE, along with the use of gram stain to identify the organism and the use of the physical exam made diagnosis a bit simpler. Despite this, however, there was no consensus as to the diagnostic definitions prior to death.
First Definitions
One of the first definitions came from Pelletier and Petersdorf (4), who performed a retrospective study on 125 patients from the University of Washington. They were one of the first authors to give a pretty in depth study on infective endocarditis (their paper is 27 pages, but it’s worth a read). Interestingly, they defined 3 different categories of infective endocarditis which may be familiar to some of you:

As you will likely notice, to be diagnosed with “definite IE” you need tissue with infected endocardial vegetation. There is no leeway here, however probable endocarditis has many of the elements we recognize with the modern diagnosis: positive blood cultures in someone with known heart disease and emboli. This was the 1970s (1977 to be exact) so this definition wouldn’t do. Next came the Beth Israel definition, also known as the Von Reyn definition (5). One change is the criteria for blood cultures; changing from requiring uniformly positive blood cultures to persistently positive, allowing some leeway here (i.e. if you have 4/6 blood cultures positive, you would be persistently positive). Further, the authors also clarified what predisposing heart conditions would lead to endocarditis, namely valvular or congenital heart disease.

Using these definitions, 19 cases were classified as definite, 44 as probable, 41 as possible, and 19 were rejected. Similar to the first criteria, however, definite endocarditis required pathological evidence from surgery or autopsy, but added that a gram stain or culture from a peripheral emboli can be used to satisfy this definition. We also see under the probable definition some definitions of what would be used in the subsequent, and more well known definition (i.e. blood cultures + something else = think of IE).
It wasn’t until more than a decade later where a fairly useful imaging tool would be incorporated into the diagnostic criteria for infective endocarditis. Echocardiogram allowed the visualization of heart valves while they were still used by a living person, meaning it was a less invasive way to secure a diagnosis. Using this new tool, a new set of criteria that were reminiscent of the Jones criteria for rheumatic fever with its major and minor signs and symptoms, were generated by the Duke endocarditis service (6; thankfully, this service does not exist anymore though, and has been replaced by a lot of transplant stuff). Here, a cohort of 353 patients were evaluated to generate this criteria. The major criteria here were positive blood culture and positive echocardiogram, both having the same weight when it came to diagnosis. Minor criteria included predisposition to IE, fever, vascular phenomena, immunological phenomena, suggestive echocardiogram findings, and suggestive microbiological findings.

They generated three categories: definite by either pathologic or clinical criteria, possible, or rejected. The authors also looked at 69 pathologically confirmed cases. 80% of the pathologically confirmed cases were classified as clinically definite IE by the Duke criteria, compared to the Beth Israel criteria’s 51%. The Duke criteria did not reject any of the pathologically confirmed cases compared to 12 of the Beth Israel criteria. Further, in the rest of the cases, 135 were classified as definite by the Duke criteria compared to only 71 by the Beth Israel criteria, suggesting a higher sensitivity.
These new criteria proved to be quite useful. A retrospective cohort of 410 patients compared the criteria with the diagnosis of 3 independent observers (7) and found that rate of agreement was high when comparing those who were classified by the Duke criteria as definite/probable (81%) with sensitivity/specificity being high as well (83 and 77%, respectively). When expanded, the Duke criteria sensitivity increased to 99.5% when the definite and possible definitions were used. The specificity was found to be around 99% when evaluating a cohort of 100 patients presenting with fever of unknown origin (8):

Other studies would confirm the superiority of the Duke criteria compared to the Von Reyn/Beth Israel definitions. One study compared 27 patients with histologically confirmed IE (9). When applying both definitions to this cohort, 22 would have been classified as definite IE by the Duke criteria compared to 12 as probable IE in the Beth Israel criteria. No patients would have been rejected by the Duke criteria compared to 5 for the Beth Israel criteria. The calculated sensitivity was statistically higher for the Duke criteria (82% vs 44%).

Similarly, the sensitivity of the Duke criteria was higher than Von Reyn’s criteria when possible IE was considered as true positive (100% vs 69%, p < 0.001) and when possible cases were considered as rejected IE (76% vs 51%, p < 0.01, 10). Notably, when comparing both criteria with surgically confirmed endocarditis, 6 cases were rejected by the Von Reyn criteria compared to none by the Duke criteria:

Specificity was 88% for the Duke criteria and 91% for Von reyn’s criteria. In another study (11), the Duke criteria was able to classify 114 episodes as “definite IE” compared to 64 by the “Beth Israel” criteria, however when adding the possible to the Beth Israel total, the difference was non-significant (114 vs 95, p = 0.1).

When looking at the 64 who had histopathological confirmation, 46 cases were defined as definitive by the Duke criteria compared to 33 who were defined as probable IE by the Beth Israel criteria. Further, 26 patients in this cohort would have been rejected by the Beth Israel criteria if surgical intervention had not been performed.

Finally, a retrospective study of 93 patients (12) found that sensitivity was superior when using the Duke criteria (76% vs 56%, p< 0.0001). Notably, 11 patients who were misclassified by the Beth Israel criteria were appropriately classified by the Duke criteria due to their echocardiogram findings. This suggests the utility of TTE in the diagnosis of endocarditis.
The Duke criteria also has a good ability to diagnose those with prosthetic valve IE when compared to the Beth Israel criteria. In one study of 25 patients (13) with pathologically confirmed PVE, the Duke criteria was able to classify 19 cases as definite and 6 cases as possible compared to 6 probable and 14 possible for the Beth israel criteria. This resulted in a sensitivity of 76% for the Duke criteria for PVE compared to 24% for the Beth Israel criteria. Similarly, both the modified and the original Duke criteria (14) performed better in prosthetic valve endocarditis compared to the Beth Israel criteria:

The Modification of the Duke Criteria
The greatest asset of the Duke criteria is the use of echocardiogram in the diagnosis of IE (indeed, one study of 69 surgical patients did not find any difference between surgical findings and TTE, 15). Since then, however, the Duke criteria have undergone some modifications in part due to several criticisms of the diagnostic requirements (16). One of the first issues was that a patient could be classified as “possible IE” if they had only one minor criteria, essentially allowing anyone with a fever to be classified as such. Due to this, the modified criteria required anyone with “possible IE” to have at least 3 minor or 1 major and 1 minor criteria. When looking at 100 pathologically confirmed cases, the addition of minor criteria did not change the classification of any cases:

Further, the minor criteria that called for “echocardiogram consistent with IE but not meeting major criteria” was eliminated.

As far as major criteria go, Q fever serology (antiphase I) IgG titer >1:800 was added as a major criteria and TEE was added as recommended for those who had prosthetic valves and had at least “possible IE.” Further, the presence of a single blood culture with Coxiella burnetti was considered a major criteria. The presence of staphylococcus aureus was still considered a major criteria.
The modified Duke criteria were evaluated in a prospective study of 241 patients (17). In this cohort, 131 patients were diagnosed with definitive IE, 79 patients with possible IE and 25 were found to have rejected IE. One of the important aspects of this study is the importance of echocardiogram for the criteria, with removal of this aspect changing 43% of cases from definite to possible, more so than the microbiological criteria:

Interestingly, the addition of microbiological criteria had a major impact of taking patients form possible to definitive diagnosis:

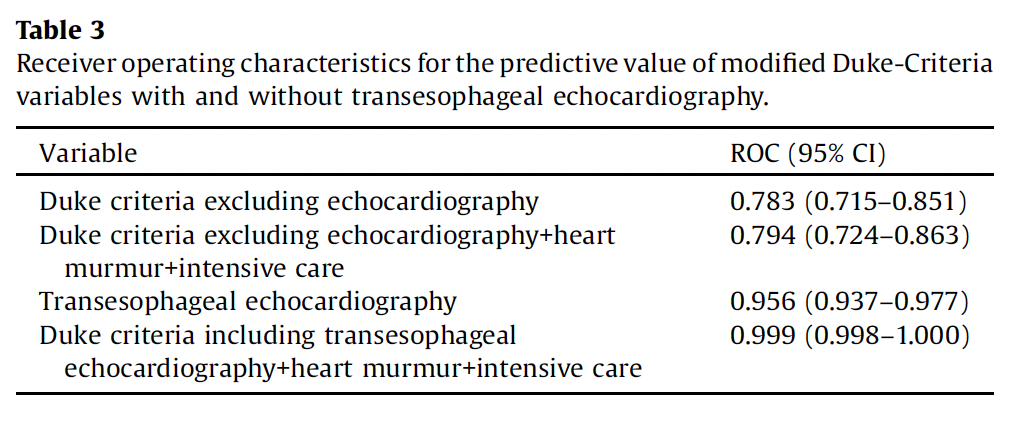
In another prospective study of 261 patients,of which 47 were diagnosed with IE, Multivariate analysis found that identification of a typical IE organism, embolic disease, and predisposing heart condition were highly associated with IE (18). Notably, fever, dermal vascular phenomena, and heart murmur were not statistically associated with IE.

The ROC for TEE, when compared to the modified Duke criteria without imaging, was significantly higher, with the highest when the modified Duke criteria, TEE, and heart murmur were combined for diagnostic purposes:
Again, the main point here is the clinical utility of echocardiography. While traditionally the teaching of endocarditis has focused on clinical phenomena such as embolic events and heart murmurs, cardiac imaging has increased the speed with which IE is diagnosed so many of these phenomena do not have time to manifest. Other imaging modalities such as PET-CT and cardiac MRI are also increasingly being used for IE, however these are not standard of care yet. One question that gets brought up is the sensitivity of TTE vs TEE, which is the topic of the next post.
References:
- Flegel KM. Our medical past. Subacute bacterial endocarditis observed: the illness of Alfred S. Reinhart. CMAJ. 2002;167(12):1379-1383.
- Geller SA. Infective endocarditis: a history of the development of its understanding. Autops Case Rep. 2013 Dec 31;3(4):5-12. doi: 10.4322/acr.2013.033. PMID: 28584801; PMCID: PMC5453655.
- Osler, W. “The Gulstonian Lectures, on Malignant Endocarditis.” British medical journal vol. 1,1262 (1885): 467-70. doi:10.1136/bmj.1.1262.467
- Pelletier LL Jr, Petersdorf RG. Infective endocarditis: a review of 125 cases from the University of Washington Hospitals, 1963-72. Medicine (Baltimore). 1977 Jul;56(4):287-313. PMID: 875718.
- Von Reyn CF, Levy BS, Arbeit RD, Friedland G, Crumpacker CS. Infective endocarditis: an analysis based on strict case definitions. Ann Intern Med. 1981 Apr;94(4 pt 1):505-18. doi: 10.7326/0003-4819-94-4-505. PMID: 7011141.
- Durack DT, Lukes AS, Bright DK. New criteria for diagnosis of infective endocarditis: utilization of specific echocardiographic findings. Duke Endocarditis Service. Am J Med. 1994 Mar;96(3):200-9. doi: 10.1016/0002-9343(94)90143-0. PMID: 8154507.
- Sekeres MA, Abrutyn E, Berlin JA, Kaye D, Kinman JL, Korzeniowski OM, Levison ME, Feldman RS, Strom BL. An assessment of the usefulness of the Duke criteria for diagnosing active infective endocarditis. Clin Infect Dis. 1997 Jun;24(6):1185-90. doi: 10.1086/513657. PMID: 9195080.
- Hoen B, Béguinot I, Rabaud C, Jaussaud R, Selton-Suty C, May T, Canton P. The Duke criteria for diagnosing infective endocarditis are specific: analysis of 100 patients with acute fever or fever of unknown origin. Clin Infect Dis. 1996 Aug;23(2):298-302. doi: 10.1093/clinids/23.2.298. PMID: 8842267.
- Hoen B, Selton-Suty C, Danchin N, Weber M, Villemot JP, Mathieu P, Floquet J, Canton P. Evaluation of the Duke criteria versus the Beth Israel criteria for the diagnosis of infective endocarditis. Clin Infect Dis. 1995 Oct;21(4):905-9. doi: 10.1093/clinids/21.4.905. PMID: 8645838.
- Cecchi E, Parrini I, Chinaglia A, Pomari F, Brusasco G, Bobbio M, Trinchero R, Brusca A. New diagnostic criteria for infective endocarditis. A study of sensitivity and specificity. Eur Heart J. 1997 Jul;18(7):1149-56. doi: 10.1093/oxfordjournals.eurheartj.a015411. PMID: 9243150.
- Heiro M, Nikoskelainen J, Hartiala JJ, Saraste MK, Kotilainen PM. Diagnosis of infective endocarditis. Sensitivity of the Duke vs von Reyn criteria. Arch Intern Med. 1998 Jan 12;158(1):18-24. doi: 10.1001/archinte.158.1.18. PMID: 9437374.
- Habib G, Derumeaux G, Avierinos JF, Casalta JP, Jamal F, Volot F, Garcia M, Lefevre J, Biou F, Maximovitch-Rodaminoff A, Fournier PE, Ambrosi P, Velut JG, Cribier A, Harle JR, Weiller PJ, Raoult D, Luccioni R. Value and limitations of the Duke criteria for the diagnosis of infective endocarditis. J Am Coll Cardiol. 1999 Jun;33(7):2023-9. doi: 10.1016/s0735-1097(99)00116-3. PMID: 10362209.
- Nettles RE, McCarty DE, Corey GR, Li J, Sexton DJ. An evaluation of the Duke criteria in 25 pathologically confirmed cases of prosthetic valve endocarditis. Clin Infect Dis. 1997 Dec;25(6):1401-3. doi: 10.1086/516145. PMID: 9431386.
- Pérez-Vázquez A, Fariñas MC, García-Palomo JD, Bernal JM, Revuelta JM, González-Macías J. Evaluation of the Duke criteria in 93 episodes of prosthetic valve endocarditis: could sensitivity be improved? Arch Intern Med. 2000 Apr 24;160(8):1185-91. doi: 10.1001/archinte.160.8.1185. PMID: 10789613.
- Yuan XC, Liu M, Hu J, Zeng X, Zhou AY, Chen L. Diagnosis of infective endocarditis using echocardiography. Medicine (Baltimore). 2019 Sep;98(38):e17141. doi: 10.1097/MD.0000000000017141. PMID: 31567953; PMCID: PMC6756706.
- Li JS, Sexton DJ, Mick N, Nettles R, Fowler VG Jr, Ryan T, Bashore T, Corey GR. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis. 2000 Apr;30(4):633-8. doi: 10.1086/313753. Epub 2000 Apr 3. PMID: 10770721.
- Topan A, Carstina D, Slavcovici A, Rancea R, Capalneanu R, Lupse M. Assesment of the Duke criteria for the diagnosis of infective endocarditis after twenty-years. An analysis of 241 cases. Clujul Med. 2015;88(3):321-6. doi: 10.15386/cjmed-469. Epub 2015 Jul 1. PMID: 26609264; PMCID: PMC4632890.
- Mahabadi AA, Mahmoud I, Dykun I, Totzeck M, Rath PM, Ruhparwar A, Buer J, Rassaf T. Diagnostic value of the modified Duke criteria in suspected infective endocarditis -The PRO-ENDOCARDITIS study. Int J Infect Dis. 2021 Mar;104:556-561. doi: 10.1016/j.ijid.2021.01.046. Epub 2021 Jan 27. PMID: 33508475.
