Hyperammonemia is the accumulation of ammonia within the blood that leads to cerebral edema, herniation, and death in patients with inborn errors of metabolism and hepatic failure. These are the types of patients where we would commonly see such accumulation of ammonia. In absence of liver failure, inborn errors of metabolism, urea cycle disorders, or kidney failure tend to be etiologies to look for. In the transplant population, however, there is more literature suggesting the role of urea-splitting organisms such as ureaplasma and Mycoplasma spp in fatal hyperammonemia syndrome.
What is the deal here?
As you may or may not know, ammonia is a metabolite of the human body, usually being broken down within the gut where portal circulation transports this metabolite into the liver, of which 10% is converted to glutamine via glutamine synthetase (1). Kidneys can also regulate the amount of ammonia, so things that damage liver and kidneys can lead to ammonia accumulation, which leads to accumulation of ammonia and their uptake into astrocytes. This is then converted to glutamine via glutamine synthetase in the astrocytes of the CNS and causing astrocyte impairment and subsequent altered mental status, lethargy, seizures, ataxia, and death. Most common causes of elevated ammonia include liver failure and inborn errors of metabolism. This, however, is not my interest here (though if you come across this on the wards or ICU, then think of urea cycle disorders). This phenomena has been seen more and more in the transplant and immunosuppressed population.
This was first described in 1991 in a bone marrow transplant patient (2) and subsequently has been described following lung transplant (3). Recently, infection with Ureaplasma and Mycoplasma spp have been implicated as possible contributing factors in this population. Ureaplasma urelyticum has been found to take up urea and produce ammonia via the urea hydrolysis, a defining feature of this organism (4). The possible connection was explored in an animal model of immunosuppressed mice with Ureaplasma infection (5) found that immunosuppressed mice challenged with intraperitoneal or intratracheal ureaplasma had significantly higher ammonia levels when compared to immunosuppressed mice without infection, and non-immunosuppressed mice:

A small retrospective study (6) found a causal relationship between Ureaplasma spp and hyperammonemia syndrome. They found that 6 patients who were either immunosuppressed or had undergone lung transplant and had elevated ammonia levels were PCR positive for U. parvum or U. urealyticum. 20 controls with normal ammonia levels and recent lung transplants were negative by PCR of ureaplasma spp. Another case notes a male who underwent a bilateral lung transplant who subsequently developed mental status changes and was found to have elevated ammonia level (7). PCR sequencing from his pleural fluid identified Ureaplasma spp along with positive BAL cultures for Ureaplasma spp. He was treated with doxycycline and sodium phenylbutyrate.
Despite the connection between lung transplantation and ureaplasma spp induced hyperammonemia, other immunosuppressed states have been reported to be associated with this phenomena. For instance, a case of hyperammonemia was described in a 12-year old girl with AML who developed altered mental status and was found to have a blood ammonia level >1600umol/L (8). She was found to have U. parvum off her blood, urine, and sputum off PCR and was treated with doxycycline and azithromycin along with CVVHD which normalized her ammonia levels:

A similar case was seen in a renal transplant patient who presented with normal liver function tests and status epilepticus along with elevated ammonia was found to have Ureaplasma spp infection (9). 2 other cases described include a patient with B cell ALL who presented with seizures and cerebral edema and another with a kidney transplant who presented with altered mentation and seizures (10). In both of these cases, PCR returned positive for either Ureaplasma or Mycoplasma, suggesting a connection between infection and elevated ammonia levels.
Treatment:
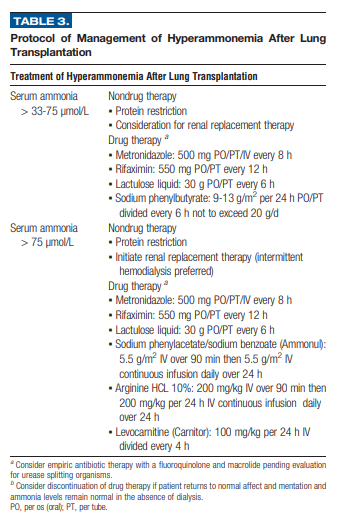
I’ve alluded to this, but therapy tends to involve 2 concepts: minimize ammonia production and accelerate nitrogen removal. Studies have attempted to use CVVHD for removal as well as binders such as sodium phenylacetate or sodium benzoate (2) with varying degrees of success. One retrospective case series of over 800 lung transplant patients evaluated 8 patients who were diagnosed with hyperammonemia (11). Treatments ranged from renal replacement therapy, protein restriction, and bowel decontamination from urea producing organism with rifaximin, lactulose, or metronidazole. A modified protocol is shown below:
Therapy with antibiotics targetted towards Ureaplasma or Mycoplasma have been shown to drop the levels of ammonia in patients (6):

Length of therapy is unclear, but some cases have used 7 days of a combination therapy of azithromycin, fluoroquinolone, or tetracyclines as some species can harbor resistance.
TL;DR
- Hyperammonemia in the transplant population may be due to infection with Ureaplasma or Mycoplasma spp
- Watch for altered mental status, coma, or seizures in the post-transplant period
- These are difficult to culture; if you suspect it, get a PCR and start dual therapy with a quinolone/tetracycline/macrolide along with ammonia binding therapy or dialysis.
References:
- Leger RF, Silverman MS, Hauck ES, Guvakova KD. Hyperammonemia Post Lung Transplantation: A Review. Clin Med Insights Circ Respir Pulm Med. 2020 Oct 26;14:1179548420966234. doi: 10.1177/1179548420966234. PMID: 33192115; PMCID: PMC7594252.
- Tse N, Cederbaum S, Glaspy JA. Hyperammonemia following allogeneic bone marrow transplantation. Am J Hematol. 1991 Oct;38(2):140-1. doi: 10.1002/ajh.2830380213. PMID: 1951305.
- Lichtenstein GR, Yang YX, Nunes FA, Lewis JD, Tuchman M, Tino G, Kaiser LR, Palevsky HI, Kotloff RM, Furth EE, Bavaria JE, Stecker MM, Kaplan P, Berry GT. Fatal hyperammonemia after orthotopic lung transplantation. Ann Intern Med. 2000 Feb 15;132(4):283-7. doi: 10.7326/0003-4819-132-4-200002150-00006. PMID: 10681283.
- Smith DG, Russell WC, Ingledew WJ, Thirkell D. Hydrolysis of urea by Ureaplasma urealyticum generates a transmembrane potential with resultant ATP synthesis. J Bacteriol. 1993 Jun;175(11):3253-8. doi: 10.1128/jb.175.11.3253-3258.1993. PMID: 8501029; PMCID: PMC204721.
- Wang X, Karau MJ, Greenwood-Quaintance KE, Block DR, Mandrekar JN, Cunningham SA, Patel R. Ureaplasma urealyticum Causes Hyperammonemia in an Experimental Immunocompromised Murine Model. PLoS One. 2016 Aug 18;11(8):e0161214. doi: 10.1371/journal.pone.0161214. PMID: 27537683; PMCID: PMC4990232.
- Bharat A, Cunningham SA, Scott Budinger GR, et al. Disseminated Ureaplasma infection as a cause of fatal hyperammonemia in humans. Science Translational Medicine. 2015 Apr;7(284):284re3. DOI: 10.1126/scitranslmed.aaa8419.
- Matson KM, Sonetti DA. Successful treatment of Ureaplasma-induced hyperammonemia syndrome post-lung transplant. Transpl Infect Dis. 2019 Feb;21(1):e13022. doi: 10.1111/tid.13022. Epub 2018 Nov 22. PMID: 30403322.
- Smith M, Crews JD, Cheek N, Srivastava R, Appachi E. Hyperammonemic Encephalopathy due to Ureaplasma parvumInfection in an Immunocompromised Child. Pediatrics. 2019 Aug;144(2):e20190601. doi: 10.1542/peds.2019-0601. Epub 2019 Jul 19. PMID: 31324704.
- Legouy C, Hu A, Mochel F, Weiss N, Collin A, Pereyre S, Perrin M, Engrand N. Ureaplasma parvum causes hyperammonemia presenting as refractory status epilepticus after kidney transplant. J Crit Care. 2020 Jun;57:79-83. doi: 10.1016/j.jcrc.2020.02.003. Epub 2020 Feb 5. PMID: 32062289.
- Nowbakht C, Edwards AR, Rodriguez-Buritica DF, Luce AM, Doshi PB, De Golovine A, Bynon JS, Nigo M. Two Cases of Fatal Hyperammonemia Syndrome due to Mycoplasma hominis and Ureaplasma urealyticum in Immunocompromised Patients Outside Lung Transplant Recipients. Open Forum Infect Dis. 2019 Mar 4;6(3):ofz033. doi: 10.1093/ofid/ofz033. PMID: 30863787; PMCID: PMC6405933.
- Chen C, Bain KB, Iuppa JA, Yusen RD, Byers DE, Patterson GA, Trulock EP, Hachem RR, Witt CA. Hyperammonemia Syndrome After Lung Transplantation: A Single Center Experience. Transplantation. 2016 Mar;100(3):678-84. doi: 10.1097/TP.0000000000000868. PMID: 26335916.
