
Thwaites GE, et al. “Adjunctive rifampicin for Staphylococcus aureus bacteraemia (ARREST): a multicentre, randomised, double-blind, placebo-controlled trial”. The Lancet. 2017. 391(10121):668-678.
This is a multicenter, randomized, double blind placebo controlled trial on the use of adjunctive rifampin (or if you’re in the UK, rifampicin) for Staph aureus bacteremia. The inclusion criteria was either MSSA/MRSA from at least one BCx, <96h of antibiotic therapy at the time of enrollement, and no pre-existing evidence of Rif resistance (or, non-susceptibility…)
Primary outcome was time to bacteriologically confirmed treatment failure or disease recurrence, or all cause death at 12 weeks (failure = signs and symptoms of infection for >14d after randomization with Staph isolated from blood cultures OR a sterile site; recurrence = isolation of Staph from a sterile site after 7d of apparent improvement. Rif was given for at least 14 days. One thing to note was that all-cause mortality by 14 days was also going to be a primary endpoint (i.e. there were going to be two co-primary endpoints), but this was dropped in favor of the aforementioned endpoint because of slow recruitment. This was done by the funder.
758 patients were enrolled, 388 in placebo and 370 in the rif group. All were well balanced:
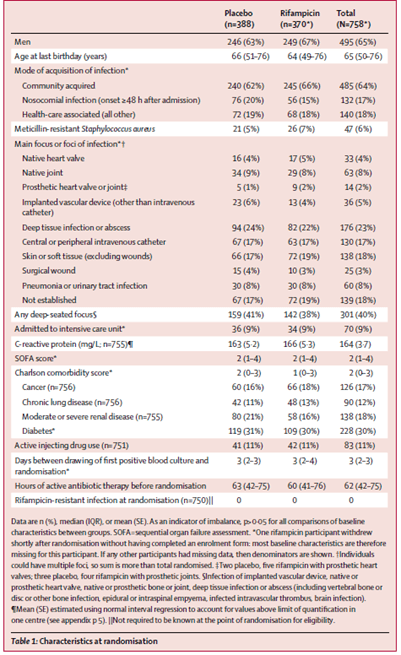
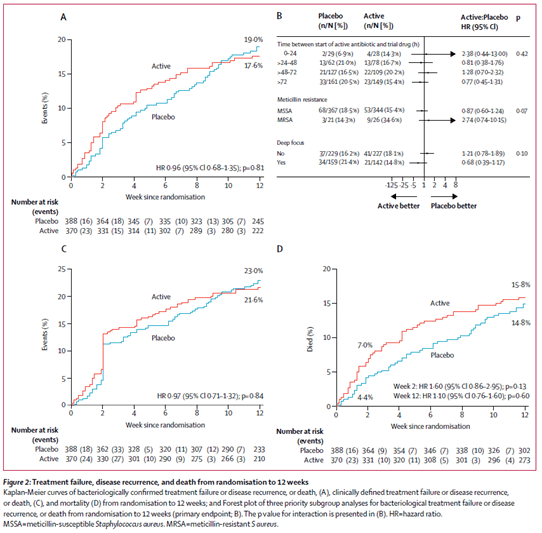
Though notably only 14 had a prosthetic valve or joint, 36 had some prosthetic material. About 82% of all patients were treated with flucloxacillin at any point, 50% with either vanco or teicoplanin. Average length of antibiotic therapy was 29 days in both groups. At the end of 12 weeks, primary outcome had occurred in 62 (17%) patients in the rif group vs 71 (18%) of patients in the placebo group (absolute risk difference -1.4%, 95% CI -7 to 4.3, HR 0.96; 0.68-1.35, p-value 0.81). Looking at this in more detail:

So it seems that in both, bacteriological and clinical failure, recurrence occurred less often in the rifampin group:
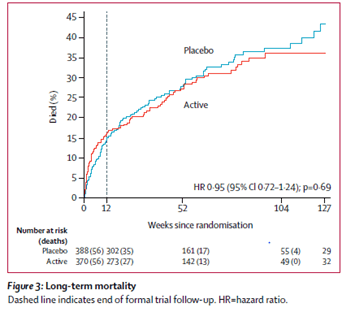
There were no differences in adverse events between the 2 groups, though there were more drug interactions in the rifampin group (24) vs the placebo group (6, p-value 0.0005). So rifampin doesn’t do much, though it needs to be said that here there were not a lot of prosthetic joint or valve infections, where rifampin tends to theoretically play a bigger role. The recurrence bit is interesting, but in the grand scheme of things, I do not know what to make of it. Perhaps we should give the rif in staph bacteremia issue… a rrest (https://www.thelancet.com/action/showPdf?pii=S0140-6736%2817%2933294-4)
Ma, Huan, et al. “Adjunctive Rifampin for the Treatment of Staphylococcus Aureus Bacteremia With Deep Infections: a Meta-analysis.” PloS One, vol. 15, no. 3, 2020, pp. e0230383.
The above study was included in a recent meta analysis of adjunctive rifampin in the treatment of SAB with respect to death rate, microbiological failure, and relapse. The meta-analysis included 7 studies, of which 5 were RCTs and 2 were retrospective cohorts that contained 979 and 636 patients treated with and without rifampin, respectively. Several studies included deep infections such as pneumonia, IE, osteomyelitis, and device infections. Primary outcome here was pooled analysis of mortality, while secondary outcomes included microbiological failure and rate of relapse.
In terms of mortality, there was no difference between groups (RR 0.771; 95% CI 0.442 to 1.347), though in the non-MRSA group (why not just call it MSSA??), there was some mortality benefit (RR 0.509, 95% CI 0.372 to 0.697). There was also no difference in rate of microbiological failure (RR 0.602, 95% CI 0.198 to 1.825) or rate of relapse (RR 0.574, 95% CI 0.106 to 3.112). So more of the same.
All in all, it seems that Rifampin’s time in the limelight of SAB not involving hardware is coming to an end. It may play a role in more complicated infections, however given the fact it interacts with everything under the sun, I am less excited to use it for the most part.
