
This is a retrospective, observational cohort study from Detroit evaluating the frequency of IV to PO switch and the population for which this is use, as well as to figure out the factors associated with failure. They recruited 492 patients with MRSA bacteremia (basically anyone with the exception of polymicrobial bacteremia and those with wither 2 or 8 weeks of IV therapy for SAB). Primary endpoint was 90 day clinical failure (composite of 90d SAB recurrence + deep seated MRSA infection + all cause mortality). The groups were not well balanced, as you would expect:
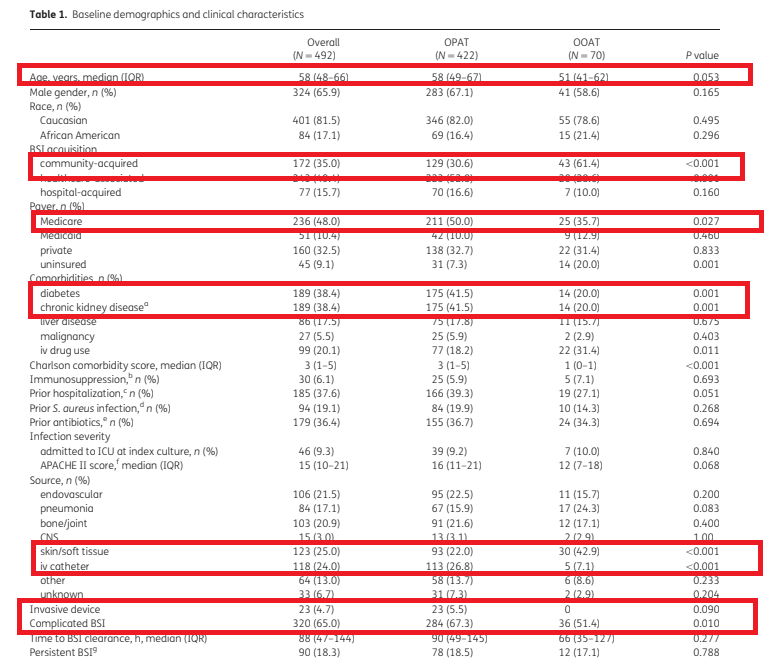
Obvoiusly, those who are at a lower risk of complicated infections OR could not pay for IV therapy were given PO. Most got linezolid (50%), TMP-SMX (34.3%) and clindamycin (15.7%). Given the difference between the groups, they did some fancy statistical yedi tricks (aka inverse probability of inverse weighting, a form of propensity matching). They noted that 5 patients (7.1%) in the PO group had clinical failure, compared to 63 (14.9%) in the OPAT group (unadjusted p- 0.08). Further broken down, comparing PO vs IV:
- Recurrence 4.3% vs 8.5%
- Invasive MRSA 1.4% vs 2.8%
- 90d all cause mortality 1.4% vs 5.5%
- All were not statistically significant
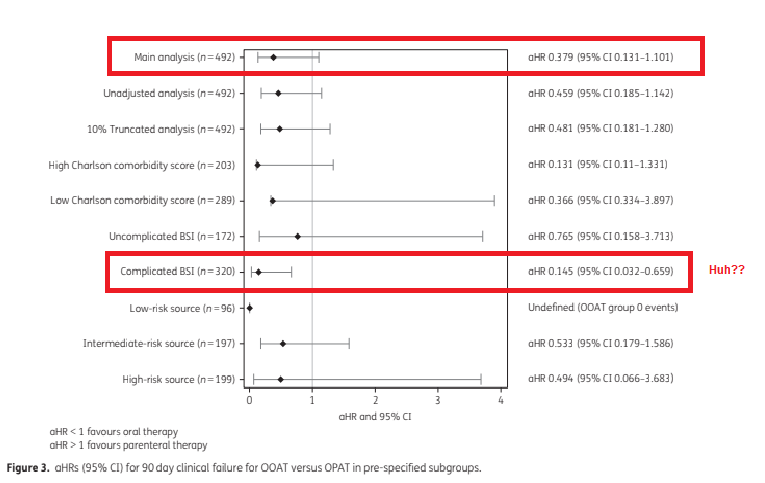
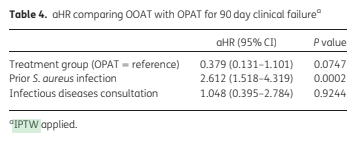
They also note that 219 patients were readmitted within 90 days, but the PO group had a significantly lower readmission rate (aHR 0.603 95% CI 0.388-0.937). Rates of readmission were similar for uncomplicated and complicated BSI for the entire cohort. Further, they found that prior S. aureus infection was a risk factor for clinical failure but not ID consultation.
I am in no way knowledgeable when it comes to statistics. There are so many issues with this study, and so many risks for biases that I do not know if statistical wizardy will get rid of. Having said that, this is as best as we can do until someone does the unthinkable (aka RCT). I am unconvinced to use PO for complicated SAB, but this does give me some comfort for when I have to use PO in someone who has low risk of complications from SAB and I have a clear source (i.e SSTI).
