COVID vaccine news, shorter antibiotics for pneumonia, and odd bugs in odd places.
Kortela E, Kanerva MJ, Puustinen J, Hurme S, Airas L, Lauhio A, Hohenthal U, Jalava-Karvinen P, Nieminen T, Finnilä T, Häggblom T, Pietikäinen A, Koivisto M, Vilhonen J, Marttila-Vaara M, Hytönen J, Oksi J. Oral Doxycycline Compared to Intravenous Ceftriaxone in the Treatment of Lyme Neuroborreliosis: A Multicenter, Equivalence, Randomized, Open-label Trial. Clin Infect Dis. 2021 Apr 26;72(8):1323-1331. doi: 10.1093/cid/ciaa217. PMID: 32133487.
This is a cool one. This was a multicenter, open-label, randomized study evaluating 4 weeks of doxycycline vs 3 weeks of ceftriaxone for the treatment of lyme neuroborreliosis. Inclusion criteria were CSF pleocytosis and intrathecal production of antibodies, or detection of B. burgdorferi DNA in CSF. Primary endpoint was improvement of the patient as evaluated by the change in the visual analogue scale (0-10, 10 being worst) at 12 months. 210 patients were recruited, with mean change in the VAS score being -3.9 in the doxycycline group (SD 2.5) and -3.8 in the CXT group (SD 2.4), mean difference 0.17 (95% CI 0.59 to 0.92). Similar results were found in the ITT population:

In patients whose initial leukocyte count was >50 cells/uL, there was no difference in the change of CSF cells from initiation to week 3:

Suheyla S Senger, George R Thompson, III, Palash Samanta, Jillian Ahrens, Cornelius J Clancy, M Hong Nguyen, Candida Empyema Thoracis at Two Academic Medical Centers: New Insights Into Treatment and Outcomes, Open Forum Infectious Diseases, Volume 8, Issue 4, April 2021, ofaa656, https://doi.org/10.1093/ofid/ofaa656
This retrospective study evaluated 81 patients with Candida empyema. This is more a of a descriptive study, but still interesting. 33% of patients had some sort of malignancy, with the majority having esophageal cancer, and 14% had solid organ transplant. 65% of the patients had some sort of surgery or invasive procedure in the preceding 90 days. Most common source was intrathoracic, followed by intra-abdominal source and then esophageal rupture:

85% of patients got an antifungal, with most receiving fluconazole (58% vs 22% for echinocandin). 98% ot some sort of pleural drainage. Notably, mortality was lowest for those whose empyema had unclear source, while those who had a spontaneous esophageal rupture had the highest mortality:

One interesting thing was that the use of caspofungin was associated with higher risk of mortality at 100 days (p=0.05) in univariate analysis, while in multivariate analysis, the OR was 4.55 (95% CI 1.1-18.8). In multivariate analysis, spontaneous esophageal rupture was also associated with increased mortality (OR 10.5, 95% CI 2.2-49.7 in one model, OR 14, 95% CI 2.4-81.3 in another model). It is interesting to note the association of increased mortality for caspofungin when compared to fluconazole. I am not aware of any studies of pharmacokinetics of azoles in comparison to echinocandins, but given the lack of their (echinocandins) utility in certain infections, I cannot say I am surprised. The range of therapy length was 14-35 days, with a median of 21 days.
Christopher Radcliffe, Savanah Gisriel, Yu Si Niu, David Peaper, Santiago Delgado, Matthew Grant, Pyomyositis and Infectious Myositis: A Comprehensive, Single-Center Retrospective Study, Open Forum Infectious Diseases, Volume 8, Issue 4, April 2021, ofab098, https://doi.org/10.1093/ofid/ofab098
This is another descriptive study, mostly with pyomysoitis and myositis. 43 patients with pyomyositis and 18 patients with myositis (inflammation of muscle due to a nearby infection, not infected muscle) were evaluated. Mean age was 48 years and most were men. Symptoms included muscle pain (95%), tenderness to palpation (69%), fever (49%) and malaise (41%). Sixty-two percent of patients grew with culture positive pyomyositis staphylococcus, with 15% growing streptococcus, and 22% growing other organisms. Of the 61 total cases, 16 were culture negative. The length of antibiotic therapy was the longest for staphylococcus and shortest for streptococcus, with a majority of patient having some sort of drainage. 84% of patients had favorable outcomes, with the lowest being in the “other” category (which included actinomyces, MAC, Nocardia, Cutibacterium, cryptococcus, E.coli, Eikenella).

Deshpande A, Richter SS, Haessler S, Lindenauer PK, Yu PC, Zilberberg MD, Imrey PB, Higgins T, Rothberg MB. De-escalation of Empiric Antibiotics Following Negative Cultures in Hospitalized Patients With Pneumonia: Rates and Outcomes. Clin Infect Dis. 2021 Apr 26;72(8):1314-1322. doi: 10.1093/cid/ciaa212. PMID: 32129438; PMCID: PMC7901260.
This retrospective study of 164 US hospitals evaluated the de-escalation practices and outcomes in patients who presented with possible pneumonia and had negative cultures. Patients had to have been on anti-MRSA and anti-pseudomonal antibiotics (excluding fluoroquinolones) to be enrolled. Outcome was the association of de-escalation on day 4 with all-cause mortality through day 14 as well as transfer to ICU, vasopressor use, mechanical ventilation, and C. diff infection. 14710 patients were evaluated, with 1924 patients having been de-escalated from both antibiotics by day 4. Patients who were de-escalated by day 4 were younger (74 vs 76), were less likely to need dialysis (4.5 vs 7.1), had higher comorbidity score (3 vs 4), and were more likely to be in the ICU and require mechanical ventilation. Notably, the rate of de-escalation was largely hospital dependent (i.e. if you were at an institution that tended to de-escalate, you were more likely to do so), though those with low mortality risk also had higher rates of de-escalation:

De-escalation by day 4 was not associated with difference in 14 day all-cause mortality, though it was associated with a lower likelihood of late ICU admission, late mechanical ventilation shorter LOS, and late vasopressor use, though no difference in C. diff infection:

This supports the idea of early de-escalation from broad spectrum antibiotics in the absence of positive cultures, which make sense as MRSA and pseudomonas are not subtle and pop up in cultures easily if they are present. Though the rate of de-escalation (13%) is a bit concerning, it is not surprising as I still see VAP/HCAP antibiotics being used for a whole course despite negative cultures in certain populations.
Dinh A, Ropers J, Duran C, Davido B, Deconinck L, Matt M, Senard O, Lagrange A, Makhloufi S, Mellon G, de Lastours V, Bouchand F, Mathieu E, Kahn JE, Rouveix E, Grenet J, Dumoulin J, Chinet T, Pépin M, Delcey V, Diamantis S, Benhamou D, Vitrat V, Dombret MC, Renaud B, Perronne C, Claessens YE, Labarère J, Bedos JP, Aegerter P, Crémieux AC; Pneumonia Short Treatment (PTC) Study Group. Discontinuing β-lactam treatment after 3 days for patients with community-acquired pneumonia in non-critical care wards (PTC): a double-blind, randomised, placebo-controlled, non-inferiority trial. Lancet. 2021 Mar 27;397(10280):1195-1203. doi: 10.1016/S0140-6736(21)00313-5. PMID: 33773631.
Now to move on to community acquired pneumonia. This was a French double-blind, randomised, placebo-controlled, non-inferiority trial in patients with moderately severe community acquired pneumonia treated with beta-lactam comparing 3 day therapy vs 8 day therapy. Patients were randomized in a 1:1 fashion after 72h of beta-lactam therapy to either PO amoxicillin-clavulanate for an additional 5 days or placebo. Primary outcome was cure 15 days after the start of antibiotic therapy (apyrexia, resolution/improvement of signs/symptoms, no additional antibiotic therapy). 310 patients were randomized, with both groups being fairly well balanced though the placebo group had higher CRP (134 vs 104) and PCT (0.55 vs 0.20). At day 15, 77% of patients in the placebo group and 68% of the patients in the beta-lactam group were cured (between-group difference 9.42%, 95% CI -0.38 to 20) in the ITT. Results were similar in the per protocol analysis:

Subgroup analysis based on PSI scores also did not show any difference in cure rates:

The recent trend has been to shorten courses of antibiotics for uncomplicated infections. This study is similar to the Uranga et al study from 2016 which evaluated 5 days of antibiotics against CAP vs standard of care at the time and found no difference in cure rates at 10 days since admission. Both studies allowed the inclusion of severely ill patients, though the difference in this study was that only beta-lactams were used compared to the Uranga study, where most used fluoroquinolones. Unfortunately, only the amox-clav combination PO was used here. Nevertheless, this provides evidence that beta-lactams would be as useful as quinolones for non-complicated CAP.
Ricotta EE, Adjemian J, Blakney RA, Lai YL, Kadri SS, Prevots DR. Extrapulmonary Nontuberculous Mycobacteria Infections in Hospitalized Patients, United States, 2009-2014. Emerg Infect Dis. 2021 Mar;27(3):845-852. doi: 10.3201/eid2703.201087. PMID: 33622461; PMCID: PMC7920686.
This study evaluated the cases of extrapulmonary non-tuberculous mycobacteria in the United States. 988 unique species were reported from 831 patients at 89 hospitals. 39% of patients had skin-soft tissue infections, while 32% had disseminated infections (blood, blood and joint, CNS). The 6 year prevalence was 11 cases/100,000 inpatients:

Patients with disseminated infections were more likely to be male (60% vs 45%), younger (40yo vs 50yo), and Black (56% vs 13%). MAC accounted for 50% of the cases, with rapidly growing NTM accounting for 28%:

MAC was more common in the northeast and West, while rapidly growing NTM was more common in the South and West US:

I think the regional differences were a bit unexpected, with the South having higher rates of rapidly growing NTM compared to the Northeast. Either way, disseminated infection tends to remain fairly rare overall, with a small percentage of patients having immunosuppressive therapy and ~20% having HIV.
Sadoff J, Gray G, Vandebosch A, Cárdenas V, Shukarev G, Grinsztejn B, Goepfert PA, Truyers C, Fennema H, Spiessens B, Offergeld K, Scheper G, Taylor KL, Robb ML, Treanor J, Barouch DH, Stoddard J, Ryser MF, Marovich MA, Neuzil KM, Corey L, Cauwenberghs N, Tanner T, Hardt K, Ruiz-Guiñazú J, Le Gars M, Schuitemaker H, Van Hoof J, Struyf F, Douoguih M; ENSEMBLE Study Group. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N Engl J Med. 2021 Apr 21. doi: 10.1056/NEJMoa2101544. Epub ahead of print. PMID: 33882225.
This is a two-year, multicenter, randomized, double-blind, phase 3 trial evaluating the efficacy of the J&J Ad25.COV2.S vaccine. Patients were enrolled in a 1:1 ratio to receive either placebo or one dose of 5×1010 viral particles of the vaccine. Primary endpoint was the efficacy of the vaccine against first occurrence of centrally confirmed moderate to severe-critical COVID-19 within 14 days or 28 days in the per-protocol population. 44,325 patients were randomized, with 55% of patients having follow up data at 8 weeks.
In terms of safety, more patients in the vaccine group had adverse events when compared to the placebo group. Notably, more patients in the vaccine group had venous thrombosis, though more patients in the placebo group died:

In terms of efficacy, at 14-days, the vaccine efficacy for moderate to severe COVID was 66.9% (adjusted 95% CI 59 to 73) while the efficacy at 28 days was 66.1% (95% CI 55 to 75):
The efficacy was higher for those with severe-critical COVID (77% efficacy, 95% CI 55 to 89 at 14 days; 85% efficacy, 95 CI 55 to 97).

Efficacy for hospitalized patients ranged from 75 to 100%:

For asymptomatic infection, the vaccine efficacy was 65% (95% CI 40 to 81). 71% of the patients had the reference COVID sequence (i.e. the original strain), while 95% of the patients in South Africa had the B.1.351 variant. Despite this, the efficacy in severe cases was maintained:

It seems that one dose of the J&J vaccine has fairly good efficacy against severe COVID, which is reassuring, including against the South Africa strain (more on that in the next paper). While the clots are an issue still, given the high numbers of patients in this trial, it may not be a significant issue down the line.
Madhi SA, Baillie V, Cutland CL, Voysey M, Koen AL, Fairlie L, Padayachee SD, Dheda K, Barnabas SL, Bhorat QE, Briner C, Kwatra G, Ahmed K, Aley P, Bhikha S, Bhiman JN, Bhorat AE, du Plessis J, Esmail A, Groenewald M, Horne E, Hwa SH, Jose A, Lambe T, Laubscher M, Malahleha M, Masenya M, Masilela M, McKenzie S, Molapo K, Moultrie A, Oelofse S, Patel F, Pillay S, Rhead S, Rodel H, Rossouw L, Taoushanis C, Tegally H, Thombrayil A, van Eck S, Wibmer CK, Durham NM, Kelly EJ, Villafana TL, Gilbert S, Pollard AJ, de Oliveira T, Moore PL, Sigal A, Izu A; NGS-SA Group Wits–VIDA COVID Group. Efficacy of the ChAdOx1 nCoV-19 Covid-19 Vaccine against the B.1.351 Variant. N Engl J Med. 2021 Mar 16:NEJMoa2102214. doi: 10.1056/NEJMoa2102214. Epub ahead of print. PMID: 33725432; PMCID: PMC7993410.
This study deals with the AstraZeneca vaccine (ChAdOx1). But before that, I think I should probably explain a bit about the variants. Remember that SARS-CoV2 has spike proteins (which make it look like a crown) and within these, there is a receptor binding domain:
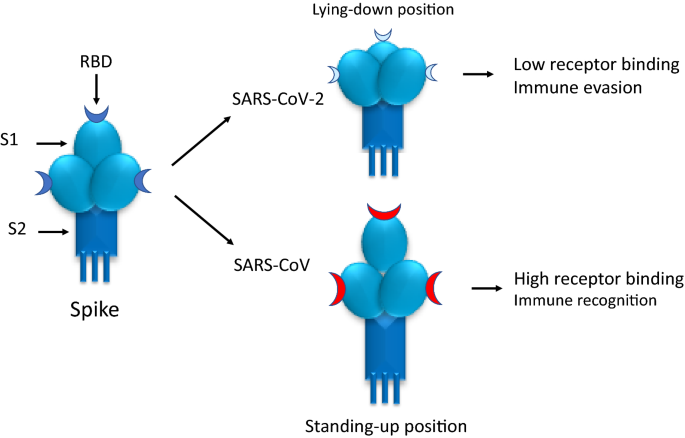
This receptor binding domain are the targets of the antibody response that are elicited by vaccines. As such, when mutations in the RBD are accumulated and changed, antibodies targeted to the original RBD will have no effect on the mutated RBD. There are a few mutations:
- N501Y: causes increased affinity of the virus to ACE2 receptors
- E484K, K417N: allows neutralizing antibody escape
There are other mutations, but you get the gist. The variants can have one or more of these mutations. For instance the B.1.1.7 (UK) variant has the N501Y mutation, while the B.1.351 (South Africa) variant actually has 3 RBD mutations.
This multisite, double-blind, randomized, placebo controlled trial was conducted in South Africa to evaluate the safety and efficacy of two doses of the AstraZeneca vaccine. Primary endpoint was efficacy against NAAT-confirmed COVID-19 infection 14d or more after the second injection (both injections separated by 21 to 35 days). 2026 patients were enrolled, with most being enrolled between June 24 and November 9, 2020 (the variant was identified in mid-November). There were 42 cases of COVID-19, 15 in the vaccine recipients and 17 in the placebo. No cases of severe disease were reported. The vaccine efficacy more than 14 days after the second dose was 21.9% (95% CI -9.9 to 59.8) in the seronegative group, dropping to 10.6% (95% CI -66 to 52) in the seropositive group. Of the 42 cases, 41 were sequenced. 39 of the cases were caused by the B.1.351 variant while 2 were caused by the B.1.1.1 and B.1.144 lineages. As seen below, the efficacy against the South Africa variant was around 10%, though post hoc analysis of those who received one dose of the vaccine up until October 31, 2020 (prior to the variant coming into play) demonstrated an efficacy of 75.4% (95% CI 8.7 to 95.5).

One interesting tidbit here is the investigators evaluated the serum in 25 participants who had neutralizing antibodies against the original virus; 6 of these did not get the vaccine so they were likely infected. 6 of the 13 vaccine recipients had no neutralization activity against an RBD triple mutant pseudovirus, while 11/13 had no neutralizing activity against the South African variant:

Furthermore, in patients who received the vaccine, there was lower live virus neutralizing antibody activity against the South African variant when compared to the B.1.1.117:

This finding is similar to that of the Moderna (lower neutralizing activity by a factor of 8.6) or the Pfizer (factor of 6.5) vaccines against the South African variant. While it is disappointing the vaccine efficacy, the reassuring bit here was the lack of severe cases (that has to count for something, right?). I do not know if the fact that enrollment ended by November, then the variant was detected, played a role in the results of the study, though the pseudovirus and live-virus neutralizing activity seem to suggest the relative lack of efficacy of the vaccine. We will have to wait and see how this pans out, though I have a suspicion this will end up being another flu that we may have to worry about down the line.
Clancy et al. (Mar 2021). Bacterial Superinfections Among Persons With Coronavirus Disease 2019: A Comprehensive Review of Data From Postmortem Studies. Open Forum Infectious Diseases. https://doi.org/10.1093/ofid/ofab065
This is a post-mortem review of patients with COVID-19 to evaluate the rate of bacterial superinfections. 621 patients whose histopathology was known were evaluated, most of which were taken prior to March 2020. Patients with proven superinfections (bacteria in lung tissue and histopathological findings of superinfection) or possible superinfections (histopathology consistent with superinfection but no bacteria seen) were classified as potential superinfections. 200/621 patients had histologic findings consistent with potential superinfection (32%). 95% of these had either bronchopneumonia, lobar pneumonia, or diffuse pneumonia, and only 3.5% had lung abscess or empyema. Only 8% of the entire cohort had proven bacterial infections and they were the cause of death in 3% of the entire cohort for whom a cause of death was assigned (or 16% of those with potential bacterial superinfections in which a cause of death was assigned). The microbiology here is presented in an incredibly large table of the studies, but had everything, including Staph aureus, Pseudomonas, E. coli, K. pneumoniae, Streptococcus, and Proteus but in most it was not stated. I think this study may have biased the results in terms of the overall prevalence of bacterial superinfection, as these came from dead patients early on in the pandemic who were likely sicker. Nevertheless, I think if you have a patient with severe COVID in the ICU, adding antibiotics may be a reasonable thing, though I would have liked to know the microbiology to better target the antibiotics (though if you do not culture anything, see above).
