
Klebsiella pneumoniae is an organism that is typically seen as the cause of pneumonia in people with diabetes and alcoholics, and it also causes nosocomial bacteremia and urinary tract infections. This is a fairly common organism to deal with in the inpatient setting, however one particular type of Klebsiella has been more frequently described in the past 40 years for its predilection to cause monomicrobial liver abscesses and its propensity to cause metastatic infections that would make Staph aureus blush.
This syndrome was first reported in 1986 in Taiwan in a case series of patients with Klebsiella pneumoniae liver abscess that were complicated by endophthalmitis, with 6 of those losing their eyesight (1). A later study of 187 patients with liver abscesses found that the majority of the 23 patients with metastatic complications had K. pneumoniae (2). With time, more reports have emerged of a similar syndrome, mostly from the Asian Pacific Rim and has also been described in Korea and China (3). . A review on the topic found that patients presenting with infection with hypervirulent K. pneumoniae tended to present predominantly with liver abscesses, and most had diabetes:

As noted, anywhere from 8-15% presented with metastatic complication, including endophthalmitis (3). This, of course, is very different from the run-of-the-mill Klebsiella infection (also known as “classic K. pneumoniae) and as such, several virulence factors have been identified.
Virulence Factors
The most widely described virulence factors include the mucus viscosity-associated gene A (magA), regulator of mucoid phenotype A gene (rmpA), and aerobactin (3). The hypervirulent phenotype of Klebsiella Pneumoniae is distinguished by the amount of capsular material compared to the classic K. pneumo bacteria (4). Hypervirulent phenotype expression is mediated by the rmpA/A2 (regulator of mucous phenotype). Furthermore, the capsular polysaccharide also plays a role in virulence by its virtue of conferring increased resistance to complement, antimicrobial peptides and phagocytosis. There are 8 capsular serotypes that have been identified (K1, K2, K5, K16, K20, K54, K57) though most infections are due to K1/K2. One of the easy ways to detect this phenotype is by doing the “string test” which involves running an inoculation loop and stretching the colonies by at least 5mm in length:
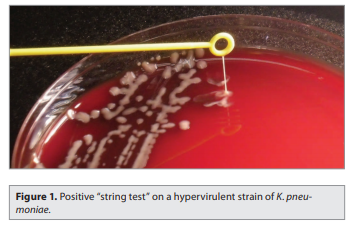
It should be noted, however, that not all K1 and K2 are hypervirulent, but rather the presence of rmpA and aerobactin play a bigger role, and K1 tends to have both of these virulence factors in spades (3).

This is seen clinically. A study of 73 isolates from patients with Klebsiella pneumoniae liver abscesses found that the majority were due to K1 and K2 (5):

magA was present in the 34 isolates serotyped as K1 and absent in all others. 89% of the 73 isolates were positive for rmpA, accounting for all K1 isolates, all 15 K2 isolates, and 24 non-K1/K2 isolates. Notably, K1 and K2 isolates were more resistant to phagocytosis, and those non-K1/K2 isolates that were rmpA+ were more resistant relative to the rmpA- isolates:

Intraperitoneal injection with K1 or K2 serotype strains into mice resulted in 100% within 2 weeks, compared to rmpA- and non K1/K2 serotypes:

These suggest the role of K1/K2 serotypes and rmpA positivity in its virulence. Another study evaluated 53 strains of K. pneumo that caused liver abscesses with 42 non-invasive strains (6) and found that 98% of the invasive strains were hyperviscous compared to only 17% in the non-invasive strains (p <0.0001). magA was present in 52/53 invasive strains compared to 15/52 non-invasive strains. Invasive strains were also more resistant to phagocytosis and serum killing compared to wild type strains:

The K1 serotype is associated with metastatic complications. A single-center retrospective study from Taiwan of 177 patients with liver abscesses found an occurrence rate of CNS/ocular complications of 13% (7). Patients infected with K1 serotypes were more likely to have CNS or ocular complications compared to non K1 serotypes (19% vs 5%, p=0.007). Univariate and multivariate analysis found that infection with K1 serotype was associated with CNS/ocular complications along with immunosuppressive therapy:

rmpA has been associated with both mortality and increased risk of metastatic infection (see later).
Risk Factors
Despite the fact that the Asian Pacific Rim has described the vast majority of cases, it has been seen both in North American and western Europe (8, 9), with a case series from France (9) noting most of those with liver abscesses were positive for rmpA.

Because of this, it is helpful to figure out risk factors for this disease. The vast majority of these cases are community-acquired, and a 2-year retrospective study of 158 patients found that those with community-acquired bacteremia tended to have diabetes and biliary tract disease (10):

An early study found (2) of 23 patients with liver abscesses and metastatic infections found that diabetes and bacteremia were associated with increased risk for complications:
Further, community acquisition was associated with an intra-abdominal or urinary source, and a higher percentage of those infections were serotype K1, with most liver abscesses being attributed to those serotypes:

This suggests that K1/K2 serotypes tend to be more prevalent in the community, though diabetes seems to be another risk factor for overall infection. In an earlier study of 23 patients with liver abscess and metastatic infection, those with diabetes along with bacteremia were more likely to have metastatic complications (2)

Comparing monomicrobial liver abscess with klebsiella with polymicrobial abscesses found that K. pneumo abscesses were associated with higher rates of metastatic complications (12% vs 0, p <0.001), and also had higher rates of diabetes mellitus and were less likely to have intra-abdominal abnormalities:

Another retrospective study (11) evaluated the clinical and radiological features in K. pneumo and non-K pneumo associated pyogenic liver abscess. 131 patients were evaluated, 101 of which had K. pneumo. Most of these were rmpA positive and expressed aerobactin:

Patients with klebsiella liver abscess tended to have higher fasting blood glucose, less likely to present with abdominal pain, and were also more likely to have diabetes and less likely to have abdominal surgery:

Notably, 35% of K. pneumo abscesses had gas on sonogram, compared to 13% in non-K.pneumo. Finally, a prospective study of 455 patients with K. pneumo bacteremia found that of the 202 with community acquired infection, 25 had liver abscess, with 60% having underlying diabetes mellitus (12):

Multivariate analysis found that residence in Taiwan, diabetes mellitus, and renal failure were associated with the presence of liver abscess. In a retrospective study comparing 88 patients with K. pneumonia infection, risk factor for hypervirulent KP included presence of rmpA gene and community acquisition (13)

Metastatic Complications – Endophthalmitis
This is a dreaded complication that can lead to devastating loss of vision. In general, infectious endophthalmitis tends to have poor prognosis. A retrospective analysis of 58 cases with endophthalmitis found a favorable anatomical outcome in only 64.3% in patients without comorbidities while dropped to 45% in those with predisposing conditions (14). Culture negative cases had worse anatomical outcomes (38.5%) compared to culture positive cases (66%). A more specific retrospective case series (15) of 19 cases of K. pneumo endophthalmitis found that the most common symptoms included blurry vision in 47%, conjunctival injection in 79%, and hypopyon in 37%. Vitreous culture was positive in 38%. Of 15 patients who survived, 9 required evisceration. Presence of hypopyon was associated with evisceration (85% vs 25%), while loss of visual acuity or loss of fundal view on presentation were not associated with worse outcomes. In a study of 200 patients with K.pneumo liver abscess (16), 22 patients were found to have metastatic infection to the eyes (11%), with most having diabetes (68%). Notably, 45% of these patients had ocular symptoms prior to their symptoms, with patients having a median of 4 days of symptoms prior to diagnosis. 41% of the affected eyes underwent evisceration or enucleation with 85% of affected eyes suffering a total loss of vision. This was despite therapy with IV antibiotics (cephalosporin and aminoglycoside), and 82% receiving intravitreal antibiotics. The biggest risk factors, besides diabetes, was found to be infection with K1/K2 serotypes as found in a case series of 134 patients with liver abscess (17):

A retrospective study of 110 patients (19) with liver abscess due to K. pneumo found that risk factors for metastatic infections included APACHE II >20, septic shock, and presence of rmpA gene:

Risk factors for mortality were similar, including metastatic infection and gas formation on imaging:

Overall, the same risk factors for invasive K. pneumoniae infection seem to be at play for metastatic infection, with the presence of rmpA, K1 serotypes, and diabetes being the major players.
Antibiotic Resistance
This seems to not be such a big problem (yet) when it comes to therapeutics, with one retrospective study (13) finding that hvKP tended to be relatively susceptible compared to classic KP, though notably aminopenicillins and piperacillin tended to show significant amounts of resistance:

Indeed, a review on the topic (19) noted that resistance is thus far a fairly rare phenomena. Despite this, however, a study of 9 isolates (20) who were positive for string test found high resistance to cefotaxime, ceftazidime (100% for both), cefoxitin (57%), amikacin (43%), ciprofloxacin (57%), and pip-tazo (72%) and several had ESBL genes associated with them, suggesting that resistance may be forthcoming. Early therapy in Taiwan (21) included therapy with cefazolin plus gentamicin for 2 weeks and treatment for at least for 3 weeks prior to stepping down to an oral cephalosporin to prevent relapse. Given the toxicity of aminoglycosides, this may not be a feasible option. As such, therapy with third generation cephalosporins, along with drainage, is more commonly used in the US (3):

Duration is unclear, but this is typically based on imaging and clinical response.
TL;DR
- Hypervirulent K. pneumonia is a clinical entity that is associated with liver abscess and can cause metastatic infections, including endophthalmitis
- This is mostly seen in the Asian Pacific rim, but more cases in the Western world have been reported
- Risk factors include community acquisition and diabetes mellitus
- K1 and K2 serotypes are the most commonly associated with invasive disease, while rmpA is a major virulence factor. Both are associated with metastatic disease
- Therapy with third gen cephs and drainage is a viable option.
References:
- Liu YC, Cheng DL, Lin CL. Klebsiella pneumoniae liver abscess associated with septic endophthalmitis. Arch Intern Med. 1986 Oct;146(10):1913-6. PMID: 3532983.
- Cheng DL, Liu YC, Yen MY, Liu CY, Wang RS. Septic metastatic lesions of pyogenic liver abscess. Their association with Klebsiella pneumoniae bacteremia in diabetic patients. Arch Intern Med. 1991 Aug;151(8):1557-9. PMID: 1872659.
- Siu LK, Yeh KM, Lin JC, Fung CP, Chang FY. Klebsiella pneumoniae liver abscess: a new invasive syndrome. Lancet Infect Dis. 2012 Nov;12(11):881-7. doi: 10.1016/S1473-3099(12)70205-0. PMID: 23099082.
- Shon AS, Bajwa RP, Russo TA. Hypervirulent (hypermucoviscous) Klebsiella pneumoniae: a new and dangerous breed. Virulence. 2013 Feb 15;4(2):107-18. doi: 10.4161/viru.22718. Epub 2013 Jan 9. PMID: 23302790; PMCID: PMC3654609.
- Yeh KM, Kurup A, Siu LK, Koh YL, Fung CP, Lin JC, Chen TL, Chang FY, Koh TH. Capsular serotype K1 or K2, rather than magA and rmpA, is a major virulence determinant for Klebsiella pneumoniae liver abscess in Singapore and Taiwan. J Clin Microbiol. 2007 Feb;45(2):466-71. doi: 10.1128/JCM.01150-06. Epub 2006 Dec 6. PMID: 17151209; PMCID: PMC1829066.
- Fang CT, Chuang YP, Shun CT, Chang SC, Wang JT. A novel virulence gene in Klebsiella pneumoniae strains causing primary liver abscess and septic metastatic complications. J Exp Med. 2004 Mar 1;199(5):697-705. doi: 10.1084/jem.20030857. PMID: 14993253; PMCID: PMC2213305.
- Fang CT, Lai SY, Yi WC, Hsueh PR, Liu KL, Chang SC. Klebsiella pneumoniae genotype K1: an emerging pathogen that causes septic ocular or central nervous system complications from pyogenic liver abscess. Clin Infect Dis. 2007 Aug 1;45(3):284-93. doi: 10.1086/519262. Epub 2007 Jun 19. PMID: 17599305.
- Nadasy KA, Domiati-Saad R, Tribble MA. Invasive Klebsiella pneumoniae syndrome in North America. Clin Infect Dis. 2007 Aug 1;45(3):e25-8. doi: 10.1086/519424. Epub 2007 Jun 18. PMID: 17599300.
- Decré D, Verdet C, Emirian A, Le Gourrierec T, Petit JC, Offenstadt G, Maury E, Brisse S, Arlet G. Emerging severe and fatal infections due to Klebsiella pneumoniae in two university hospitals in France. J Clin Microbiol. 2011 Aug;49(8):3012-4. doi: 10.1128/JCM.00676-11. Epub 2011 Jun 15. PMID: 21677064; PMCID: PMC3147753.
- Tsay RW, Siu LK, Fung CP, Chang FY. Characteristics of bacteremia between community-acquired and nosocomial Klebsiella pneumoniae infection: risk factor for mortality and the impact of capsular serotypes as a herald for community-acquired infection. Arch Intern Med. 2002 May 13;162(9):1021-7. doi: 10.1001/archinte.162.9.1021. PMID: 11996612.
- Wang J, Yan Y, Xue X, Wang K, Shen D. Comparison of pyogenic liver abscesses caused by hypermucoviscous Klebsiella pneumoniae and non-Klebsiella pneumoniae pathogens in Beijing: a retrospective analysis. J Int Med Res. 2013 Aug;41(4):1088-97. doi: 10.1177/0300060513487645. Epub 2013 May 31. PMID: 23729468.
- Ko WC, Paterson DL, Sagnimeni AJ, Hansen DS, Von Gottberg A, Mohapatra S, Casellas JM, Goossens H, Mulazimoglu L, Trenholme G, Klugman KP, McCormack JG, Yu VL. Community-acquired Klebsiella pneumoniae bacteremia: global differences in clinical patterns. Emerg Infect Dis. 2002 Feb;8(2):160-6. doi: 10.3201/eid0802.010025. PMID: 11897067; PMCID: PMC2732457.
- Li W, Sun G, Yu Y, Li N, Chen M, Jin R, Jiao Y, Wu H. Increasing occurrence of antimicrobial-resistant hypervirulent (hypermucoviscous) Klebsiella pneumoniae isolates in China. Clin Infect Dis. 2014 Jan;58(2):225-32. doi: 10.1093/cid/cit675. Epub 2013 Oct 7. PMID: 24099919.
- Ratra D, Saurabh K, Das D, Nachiappan K, Nagpal A, Rishi E, Bhende P, Sharma T, Gopal L. Endogenous Endophthalmitis: A 10-Year Retrospective Study at a Tertiary Hospital in South India. Asia Pac J Ophthalmol (Phila). 2015 Sep-Oct;4(5):286-92. doi: 10.1097/APO.0000000000000120. PMID: 26181589.
- Ratra D, Saurabh K, Das D, Nachiappan K, Nagpal A, Rishi E, Bhende P, Sharma T, Gopal L. Endogenous Endophthalmitis: A 10-Year Retrospective Study at a Tertiary Hospital in South India. Asia Pac J Ophthalmol (Phila). 2015 Sep-Oct;4(5):286-92. doi: 10.1097/APO.0000000000000120. PMID: 26181589.
- Yang CS, Tsai HY, Sung CS, Lin KH, Lee FL, Hsu WM. Endogenous Klebsiella endophthalmitis associated with pyogenic liver abscess. Ophthalmology. 2007 May;114(5):876-80. doi: 10.1016/j.ophtha.2006.12.035. PMID: 17467526.
- Fung CP, Chang FY, Lee SC, Hu BS, Kuo BI, Liu CY, Ho M, Siu LK. A global emerging disease of Klebsiella pneumoniae liver abscess: is serotype K1 an important factor for complicated endophthalmitis? Gut. 2002 Mar;50(3):420-4. doi: 10.1136/gut.50.3.420. PMID: 11839725; PMCID: PMC1773126.
- Lee SS, Chen YS, Tsai HC, Wann SR, Lin HH, Huang CK, Liu YC. Predictors of septic metastatic infection and mortality among patients with Klebsiella pneumoniae liver abscess. Clin Infect Dis. 2008 Sep 1;47(5):642-50. doi: 10.1086/590932. PMID: 18643760.
- Lee CR, Lee JH, Park KS, Jeon JH, Kim YB, Cha CJ, Jeong BC, Lee SH. Antimicrobial Resistance of Hypervirulent Klebsiella pneumoniae: Epidemiology, Hypervirulence-Associated Determinants, and Resistance Mechanisms. Front Cell Infect Microbiol. 2017 Nov 21;7:483. doi: 10.3389/fcimb.2017.00483. PMID: 29209595; PMCID: PMC5702448.
- Remya P, Shanthi M, Sekar U. Occurrence and characterization of hyperviscous K1 and K2 serotype in Klebsiella pneumoniae. J Lab Physicians. 2018;10(3):283-288. doi:10.4103/JLP.JLP_48_18
- Wang JH, Liu YC, Lee SS, Yen MY, Chen YS, Wang JH, Wann SR, Lin HH. Primary liver abscess due to Klebsiella pneumoniae in Taiwan. Clin Infect Dis. 1998 Jun;26(6):1434-8. doi: 10.1086/516369. PMID: 9636876.
