
Unlike some of my previous recent posts (read: Leishmania, Hantavirus), I think this one is of value. The reason being this bug is not thought of (outside of medical school, when it is learned with Nocardia). Most of the time, this infection is diagnosed by the pathologist, after a surgery to remove what is thought to be a tumor. Given this organism remains exquisitely sensitive to penicillins and can be cured by antibiotics alone, consideration of this etiology needs to be done in the early stages of diagnosis. I am talking about Actinomyces spp.
Basics of the Bug:
Actinomyces belongs to the actinomycetales order and are what are considered “higher order” bacteria (1, 2). These are gram positive, filamentous, non-spore forming anaerobic bacteria that tends to colonize the mouth, GI, and GU tract. Of note, while not really important to get into the weeds here, the bacteria is related to Nocardia, Mycobacteria, Corynebacterium, and Propionibacterium (3).

Notably, this organism has never been isolated from nature (2), and colonization tends to occur early, with oral cavity colonization with Actinomyces been around ⅓ by age of 2 months and nearly 100% by the age of 2 (4). Further, Actinomyces species plays a role in the initial sages of biofilm formation on teeth (plaques; 5). Various studies have also cited the isolation of actinomyces throughout the GI tract and GU tract (1) :

Over 30 species of actinomyces have been isolated and described:

Despite this extensive list, six have been the ones that have been known to cause most disease: A. israelii, A. naeslundii, A. odontolyticus, A. viscous, A. meyeri, and A. gerencseriae. By far, all of these species tend to cause very similar presentations, so there no reason to fret about each species. The highlight of these species is that, when they cause infection, the presentation tends to be an indolent, slowly progressing granulomatous disease categorized according to the body site.
Given its role as a colonizer of oral and GI/GU flora, its virulence tends to not be impressive. Indeed, in many cases it tends to be isolated with other oral commensals such as Aggregatibacter actinomycetemcomitans, Eikenella corrodens, Capnocytophagia, fusobacteria, bacteroides, and streptococci (6). This association with other bacteria may actually help with its pathophysiology, serving as co-pathogens and aiding in the inhibition of host defenses, or by reducing oxygen tension (2). For instance, the combination of A. viscous and S. smitis lead to a greater proportion of abscess formation in mice compared to heat-treated strains of either organism (7):


Moreover, seems the combination was more resistant to phagocytosis and killing by neutrophils in vitro and in vivo:

In another animal study (8), lower doses of A. israelii were required when co-infected with Eikenella corrodens (1.7 x 107 CFU vs 8.5 x 104 CFU):

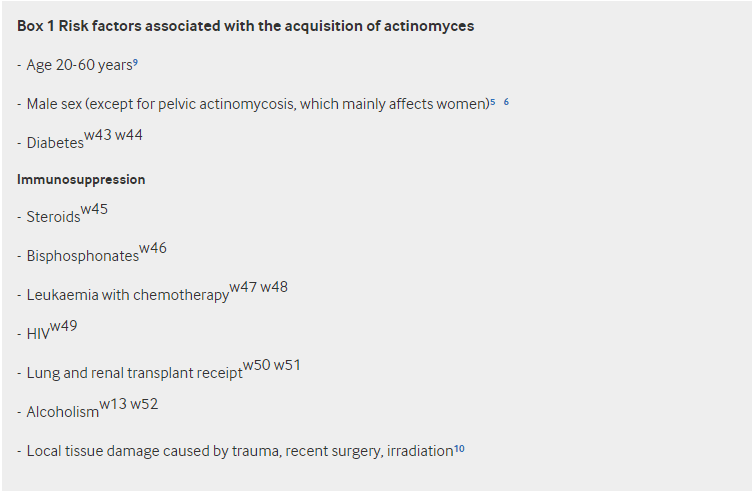
The second part of the equation is disruption of the mucosal barrier. Cervicofacial disease is typically found after head and neck surgery (9), dental surgery, trauma (10), or prior infection (11). Abdominal surgeries are also a risk factor for abdomino-pelvic presentation (12). IUDs have been reported to be a risk factor, with one case series reporting 7% of women with IUDs being colonized with Actinomyces (13). Indeed, a review found a total of 11 cases of pelvic actinomyces associated with IUDs (14).
Clinical Presentations:
There are 3 general clinical presentations to remember:
- Cervicofacial
- Abdomino-pelvic
- Pulmonary
The most common presentation is cervicofacial, with abdomino-pelvic and pulmonary being others to keep in the back pocket of your differential diagnosis. When it comes to the cervicofacial presentation (which accounts for roughly 65% of all cases of actinomycosis), it typically presents as a chronic painless or painful soft tissue swelling of the perimandibular region, from which a sinus tract can develop over time (15). Other presentations include an abscess, mass lesion, indurated mass, or ulcerative lesion. A hallmark of this disease is its propensity to cross tissue planes (2). For instance, extension into the skin into a sinus tract (or multiple sinus tracts) can develop, involvement of muscles of mastication has been described, as well as mandibular periostitis or osteomyelitis can also be found, though this is rare. Typically, this follows a traumatic event as noted above, either surgery or a previous infection, whatever causes a breach in the mucosal surface. Typically, this is cultured along with other commensals. Other risk factors include poor oral hygiene (3). Furthermore, actinomyces has also been implicated in the pathogenesis of both osteoradionecrosis and bisphosphonate-associated osteonecrosis.
Abdominal actinomycosis makes up 20% of all cases of actinomycosis, with the most common risk factor being appendicitis complicated by perforation. Other risk factors include laparoscopic procedures, GI perforation, neoplasia, or foreign bodies. The presentation here can be delayed from the previous surgery. A case report of 2 patients described actinomyces abscesses following surgical interventions (laparoscopic cholecystectomy) with presentation occurring 18 months and 30 months after surgical intervention (16). One patient had a retroperitoneal abscess with connection to subcutaneous tissue and presence of a sinus tract. The delay may be up to several years. Symptoms here are non-specific, with fever, weight loss, abdominal pain, or sensation of a mass being described in the literature. It can present as an abscess, or a firm hard mass that is fixed to an underlying tissue, mimicking malignancy in some instances (17).
As mentioned previously, women who have an IUD can be come colonized with actinomycosis, though in these instances, this is benign. Despite this, pelvic actinomycosis has been identified as a risk factor of IUD placement. For instance, a review on the topic (18) found 92 cases of pelvic actinomycosis associated with IUD placement. In this cohort, the average age of the patients was 37 years old, with mean use of IUD being 8 years. In some instances, pelvic actinomycosis has been confused with malignancy (19, 20).

Pulmonary actinomycoses have also been reported, though this is rarer relative to the other 2 presentations. Usually follows chronic aspiration in setting of poor dentition, leading to a presentation resembling that of a chronic pneumonia, sometimes mimicking tuberculosis and malignancy. In one case of 19 patients (21), most patients presented with cough, sputum production, chest pain, and hemoptysis. Nine of these patients had a provisional diagnosis of cancer with only 2 developing cutaneous symptoms. Another case report notes how bronchial actinomycosis can also look like carcinoma in the setting of FDG-PET, with similar uptake of radioactive material (22). Furthermore, given its propensity to cross tissue planes, contiguous extension into ribs, sternum, shoulder girdle, as well as involvement of chest-wall muscles and soft tissues have been described (23). Involvement of mediastinal structures, leading to the development of pericarditis and myocarditis, has also been described (23).
Pathology:
A brief word on the pathology here, since it is a bit interesting. Typically, they develop a chronic granulomatous infection characterized by the formation of tiny clumps (aka sulfur granules), which are an internal tangle of mycelial fragments stabilized by a protein-polysaccharide complex (3). These are thought to provide some resistance to phagocytosis. Microscopic findings include necrosis with a yellowish sulfur granules and filamentous gram-positive fungal-like pathogens. The sulfur granules represent a conglomeration of bacteria trapped in biofilm, and these appear as round/oval basophilic mass with eosinophilic terminal “clubs” on H&E staining (15):


Diagnosis:
This is a tricky diagnosis, because it is not thought of frequently given its propensity to mimic tuberculosis, malignancy, or other fungal infections such as histoplasmosis or cryptococcus. Due to this, cultures have a high failure rate of isolation, quoted to be >50%. Ideally, a large sample of tissue can be obtained to look at characteristics such as sulfur granules, as with small samples these can be missed and the specimen will only show fibrosis with or without inflammation (2).
Cultures can also be tricky. Ideally, isolation would be from puss, tissue, or sulphur granules and not swabs. These are fastidious bacteria and require cultures enriched with brain-heart infusion media, aided in growth with ambient CO2 at 6-10%. Further, while most are microaerophilic, some are strict anaerobes, so whenever possible let the micro lab know so these can be grown in anaerobic conditions. While growth can appear after 3-7 days, it may need to be observed for up to 21 days as it can be slow growing. Some clues to the diagnosis include:
- “Bread crumb” appearance on broth
- “Molar tooth” colonies on agar

One interesting phenomena that can be seen on H&E staining is called the Splendore-Hoeppli phenomena and it is thought to be an ill-defined host response (2). This is a unique reaction characterized by bacteria being surrounded by radiating eosinophilic material. It has believed to be due to deposition of antigen-antibody complexes and debris from the host inflammatory cells (24).

Treatment:
Unfortunately, there is no randomized controlled trial or retrospective data to draw from, but rather extensive experience for well over 70 years. A few principles have evolved:
- Resistance to penicillin is not common and remains the first line therapy
- Total duration of therapy ranges from 6-12 months, largely due to the avascularity and induration of infected areas (2-6 weeks of high dose IV therapy followed by the rest with PO)
A survey from the UK evaluated 87 isolates of Actinomyces (25) and found that all were susceptible to penicillin and amoxicillin. A number were less susceptible to pip-tazo, with all being resistant to ciprofloxacin and only 3% being resistant to linezolid:

A Danish survey of 37 isolates (2) found all strains to be sensitive to benzylpenicillin, pip-tazo, CTX, meropenem, erythromycin, clindamycin, and linezolid:

Some reviews note decreased activity of third-generation cephalosporins in some strains (A. europaus, A. graevenitzii), and even considers some PO options such as oxacillin, cloxacillin, and cephalexin to not be active (3). Despite the experience with prolonged therapy, some infections may warrant shorter duration such as 2 months for mild cervicofacial disease (2) with oral options upfront being reasonable choices (PO Pen V 2-4g per day divided in four doses; PO amoxicillin 1.5 to 3g per day divided into three or four doses). All told, go high with penicillins here.
Other infections, the recommendation is as follows:
- IV penicillin G 18-24 million units/day divided q6h for 4-6 weeks followed by PO Penicillin V 2-4g/d divided q6h for 6-12 months OR amoxicillin 500mg q6h (note: Mendel cites 18-24 million units per day, while Smego et al cites 10-20 million units, though you could probably go either way here as long as the patient is able to tolerate it).
- Cephalosporins such as CTX, followed by doxycycline or clindamycin can also be used if penicillin allergic.
- Others that have in vitro activity that you can use include moxifloxacin, linezolid, and ertapenem
- For OPAT purposes, continuous infusion of penicillin is one option, or a high dose of CTX (2g q24h) can also be done
TL;DR
- Actinomycosis is a gram positive rod that resembles a fungus, is not isolated from nature, and is a colonizer of the oral flora, GI tract, and GU tract
- The presentation is usually chronic and indolent, with some systemic symptoms including fevers and weight loss.
- Its calling card is the fact it crosses tissues plane; don’t be surprise if a thoracic lesion invades pleura, ribs, and go into soft tissue as well as skin
- It remains incredibly susceptible to penicillins. Therapy for severe infection is prolonged (6-12 months), with IV given for the first 4-6 weeks.
References:
- Könönen E, Wade WG. Actinomyces and related organisms in human infections. Clin Microbiol Rev. 2015 Apr;28(2):419-42. doi: 10.1128/CMR.00100-14. PMID: 25788515; PMCID: PMC4402957.
- Bennett, J. E., Dolin, R., & Blaser, M. J. (2014). Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Elsevier Inc.
- Valour F, Sénéchal A, Dupieux C, Karsenty J, Lustig S, Breton P, Gleizal A, Boussel L, Laurent F, Braun E, Chidiac C, Ader F, Ferry T. Actinomycosis: etiology, clinical features, diagnosis, treatment, and management. Infect Drug Resist. 2014 Jul 5;7:183-97. doi: 10.2147/IDR.S39601. PMID: 25045274; PMCID: PMC4094581.
- Sarkonen N, Könönen E, Summanen P, Kanervo A, Takala A, Jousimies-Somer H. Oral colonization with Actinomyces species in infants by two years of age. J Dent Res. 2000 Mar;79(3):864-7. doi: 10.1177/00220345000790031301. PMID: 10765961.
- Zijnge V, van Leeuwen MB, Degener JE, Abbas F, Thurnheer T, Gmür R, Harmsen HJ. Oral biofilm architecture on natural teeth. PLoS One. 2010 Feb 24;5(2):e9321. doi: 10.1371/journal.pone.0009321. PMID: 20195365; PMCID: PMC2827546.
- Schaal KP, Lee HJ. Actinomycete infections in humans–a review. Gene. 1992 Jun 15;115(1-2):201-11. doi: 10.1016/0378-1119(92)90560-c. PMID: 1612438.
- Ochiai K, Kurita-Ochiai T, Kamino Y, Ikeda T. Effect of co-aggregation on the pathogenicity of oral bacteria. J Med Microbiol. 1993 Sep;39(3):183-90. doi: 10.1099/00222615-39-3-183. PMID: 8366516.
- Jordan HV, Kelly DM, Heeley JD. Enhancement of experimental actinomycosis in mice by Eikenella corrodens. Infect Immun. 1984 Nov;46(2):367-71. doi: 10.1128/IAI.46.2.367-371.1984. PMID: 6389342; PMCID: PMC261540.
- Zitsch 3rd RP, Bothwell M. Actinomycosis: a potential complication of head and neck surgery. Am J Otolaryngol. 1999 Jul-Aug;20(4):260-2. doi: 10.1016/s0196-0709(99)90012-1. PMID: 10442782.
- Moturi K, Kaila V. Cervicofacial Actinomycosis and its Management. Ann Maxillofac Surg. 2018;8(2):361-364. doi:10.4103/ams.ams_176_18
- Belmont MJ, Behar PM, Wax MK. Atypical presentations of actinomycosis. Head Neck. 1999 May;21(3):264-8. doi: 10.1002/(sici)1097-0347(199905)21:3<264::aid-hed12>3.0.co;2-y. PMID: 10208670.
- Vyas JM, Kasmar A, Chang HR, Holden J, Hohmann E. Abdominal abscesses due to actinomycosis after laparoscopic cholecystectomy: case reports and review. Clin Infect Dis. 2007 Jan 15;44(2):e1-4. doi: 10.1086/510077. Epub 2006 Dec 6. PMID: 17173208.
- Westhoff C. IUDs and colonization or infection with Actinomyces. Contraception. 2007 Jun;75(6 Suppl):S48-50. doi: 10.1016/j.contraception.2007.01.006. Epub 2007 Mar 23. PMID: 17531616.
- García-García A, Ramírez-Durán N, Sandoval-Trujillo H, Romero-Figueroa MDS. Pelvic Actinomycosis. Can J Infect Dis Med Microbiol. 2017;2017:9428650. doi: 10.1155/2017/9428650. Epub 2017 Jun 8. PMID: 28684963; PMCID: PMC5480022.
- Wong VK, Turmezei TD, Weston VC. Actinomycosis. BMJ. 2011 Oct 11;343:d6099. doi: 10.1136/bmj.d6099. PMID: 21990282.
- Vyas JM, Kasmar A, Chang HR, Holden J, Hohmann E. Abdominal abscesses due to actinomycosis after laparoscopic cholecystectomy: case reports and review. Clin Infect Dis. 2007 Jan 15;44(2):e1-4. doi: 10.1086/510077. Epub 2006 Dec 6. PMID: 17173208
- Ridha A, Oguejiofor N, Al-Abayechi S, Njoku E. Intra-Abdominal Actinomycosis Mimicking Malignant Abdominal Disease. Case Rep Infect Dis. 2017;2017:1972023. doi: 10.1155/2017/1972023. Epub 2017 Feb 19. PMID: 28299215; PMCID: PMC5337322.
- Fiorino AS. Intrauterine contraceptive device-associated actinomycotic abscess and Actinomyces detection on cervical smear. Obstet Gynecol. 1996 Jan;87(1):142-9. doi: 10.1016/0029-7844(95)00350-9. PMID: 8532252.
- Kumar N, Das P, Kumar D, Kriplani A, Ray R. Pelvic actinomycosis mimicking: an advanced ovarian cancer. Indian J Pathol Microbiol. 2010 Jan-Mar;53(1):164-5. doi: 10.4103/0377-4929.59216. PMID: 20090255.
- Munjal K, Nandedkar S, Subedar V, Jain S. Tubo-ovarian actinomycosis mimicking as ovarian malignancy: report of three cases. Indian J Pathol Microbiol. 2010 Oct-Dec;53(4):870-1. doi: 10.4103/0377-4929.72020. PMID: 21045457.
- Kinnear WJ, MacFarlane JT. A survey of thoracic actinomycosis. Respir Med. 1990 Jan;84(1):57-9. doi: 10.1016/s0954-6111(08)80095-9. PMID: 2371423.
- Andreani A, Rossi G, Giovannini M, Cappiello GF. Unexpected positron emission tomography-positive actinomyces-related mass of the bronchial stump. Can Respir J. 2012 Mar-Apr;19(2):77-9. doi: 10.1155/2012/502041. PMID: 22536574; PMCID: PMC3373284.
- Smego RA Jr, Foglia G. Actinomycosis. Clin Infect Dis. 1998 Jun;26(6):1255-61; quiz 1262-3. doi: 10.1086/516337. PMID: 9636842.
- Gopinath D. Splendore-Hoeppli phenomenon. J Oral Maxillofac Pathol. 2018;22(2):161-162. doi:10.4103/jomfp.JOMFP_79_18
- Smith AJ, Hall V, Thakker B, Gemmell CG. Antimicrobial susceptibility testing of Actinomyces species with 12 antimicrobial agents. J Antimicrob Chemother. 2005 Aug;56(2):407-9. doi: 10.1093/jac/dki206. Epub 2005 Jun 21. PMID: 15972310.
- Hansen JM, Fjeldsøe-Nielsen H, Sulim S, Kemp M, Christensen JJ. Actinomyces species: A danish survey on human infections and microbiological characteristics. Open Microbiol J. 2009 Jul 23;3:113-20. doi: 10.2174/1874285800903010113. PMID: 19657460; PMCID: PMC2720514.
