
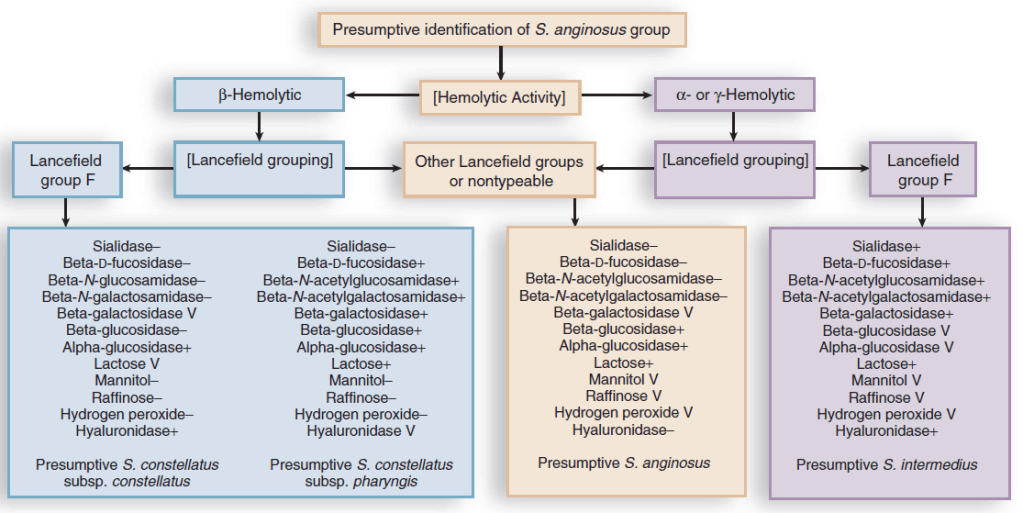
The group streptococcus anginosis or milleri consist of 3 types of streptococci. These include Streptococcus intermedius, Streptococcus constellatus, and streptococcus anginosus and they are usual colonizers of the oropharygneal, urogenital, and gastrointestinal tract and tend to cause pyogenic infections (i.e. abscesses, 1). While I mentioned in a previous post that I tend to think of these as a type of viridans streptococci (2), they actually have different hemolytic activities and Lancefield grouping:

Virulence Factors and Association with Anaerobes
I have mentioned previously I am not a fan of going over virulence factors because they have no use in a clinical setting. Factors such as adhesins which bind fibronectin and leads to the binding of platelets (1, 3), its capsule (similar to pneumococcus), and intermedilysin, which is a cytotoxin that has been suggested to be responsible for some strains to cause liver abscess. One of the more interesting tidbits seems to be its interaction with anaerobes. Given it colonizes the oropharyngeal flora, it is not surprising some abscesses will be polymicrobial and these 2 groups of organisms have some sort of synergistic activity. For instance, a mouse model found that co-infection with both an organism from the S. milleri group and F. nucleatum resulted in bigger abscesses (4):

As well as a higher degree of bacterial recovery when both were innoculated:

Another model of pneumonia in mice evaluated the combination of S. constellatus and Prevotella intermedia (5). More mice who were inoculated with both died:
And S. constellatus bacteria recovery was higher when combined with P. intermedia both in vitro and in mice lungs:


Why this is the case is unclear, though one study (5) proposes that it may be due to the ability of anaerobes by their metabolic products or capsules to inhibit phagocytosis of anaerobes, alterations of local environment that leads to reduction of oxygen tension, or production of substances toxic to the host. In a study of BAL from 59 patients using 16s sequencing (6), anaerobes made up 42.5% of organisms obtained from cultures, with 62.7% being mixed infections, and 15.3% having S. anginosus group as well. These suggests that, at least for oropharyngeal and lung abscess, both S. milleri group and anaerobes tend to go together.
Clinical Characteristics
If there is one thing to know about these organisms if you see them on blood culture, is if you find it, look for an abscess. For instance, a case series of 51 bacteremic episodes found that 6/51 ended up with an abscess (11.8%, 7) with this number going up to 31.6% in a review of 158 other bacteremic cases. Another single-center retrospective study of 263 cases found that 60% of these caused some sort of abscess (8). These included intra-abdominal abscess (69 patients, 43.1%), skin and soft tissue abscesses/arthritis/OM (44 patients, 28.1%), empyema or lung abscess (32 patients, 20%), CNS abscess (15 patients 9.4%). The most commonly recovered organism was S. anginosus (69.2%), followed by S. constellatus (17.1%) and S. intermedius (13.7%). A multivariate model found that abscesses were less common in S. anginosus and S. constellatus when compared to S. intermedius:

Indeed, 31 of 36 infections with S. intermedius involved an abscess. In another study of 153 clinical isolates (9), S. anginosus was the most commonly isolated organism of the Strep milleri group:

Notably, the S. intermedius group made up the vast majority of the Strep milleri group CNS abscesses. This pattern of S. intermedius being more common in CNS abscesses held up in a retrospective study of 463 patients (10), which included 254 patients with S. anginosus, 173 with S. constellatus, and 36 for S. intermedius. S. constellatus was more likely to cause thoracic infections while S. intermedius constituted nearly 50% of CNS infections in this cohort:

Besides body part, there was a distribution seen for each organism in regards to age, with S. constellatus infection being more common in middle age (35-54) and S. intermedius having more cases in those >65:

Another study of 76 cases found that all CNS abscesses were due to S. intermedius, with S. agninosus being the most commonly isolated organism of the SMG and the vast majority of abscesses being intra-abdominal (11):

Further, in one retrospective analysis of 245 cases (12), S. anginosus was the most commonly isolated organism, with the most common method of culture identification was through pus (35%), which included mostly intra-abdominal fluid collections.

Most of the community acquired infections were intra-abdominal spontaneous abscesses (67/144, 47%) while hospital-acquired infections were generally surgical complications (43/52, 83%). Another case series of 3 culture negative brain abscesses were attributed to S. intermedius after 16S ribosomal sequencing (13). Deep neck, and ENT infections have also been attributed to S. milleri group, which was evident in a case series of 16 cases of such infections (14).
To summarize:
- Strep anginosis tends to be the most commonly cultured organism of this family
- Strep intermedius, while rare, tends to cause CNS disease
- Most common pyogenic infection tends to be intra-abdominal, either liver disease, gallbladder, or peritoneal
Tissue Planes
Infections that cross from one area to another, i.e. those that cross tissue planes, are rare and include actinomyces and mucormycosis. One example of this pathogenesis includes the crossing of pleural surfaces into the chest wall, mediastinum, or into the abdomen (it goes everywhere). One of the interesting things about the streptococcus anginosis group is that these can also cross tissue planes and it has been described in several case series. A review of e cases (15) found extension of a right middle lobe mass into the anterior right lower lobe and into the pleural space, infection involving the entire left lobe of the lung going into the right lobe of the liver and the gallbladder/diaphragm, pericardial space, and a left lobe mass extending into the chest wall. Another case report found concurrent pulmonary nodule and empyema (16), and one case reported on a patient with pulmonary and brain involvement (17). Sinusitis complicated by a brain abscess (18) and necrotizing fasciitis developing into an empyema have also been described (19, the pictures here are quite brutal; I won’t post them here but you can look at the citation).
References:
- [edited by] John E. Bennett, Raphael Dolin, Martin J. Blaser. Mandell, Douglas, And Bennett’s Principles and Practice of Infectious Diseases. Philadelphia, PA :Elsevier/Saunders, 2015.
- Siegman-Igra Y, Azmon Y, Schwartz D. Milleri group streptococcus–a stepchild in the viridans family. Eur J Clin Microbiol Infect Dis. 2012 Sep;31(9):2453-9. doi: 10.1007/s10096-012-1589-7. Epub 2012 Mar 6. PMID: 22391759.
- Ruoff KL. Streptococcus anginosus (“Streptococcus milleri”): the unrecognized pathogen. Clin Microbiol Rev. 1988 Jan;1(1):102-8. doi: 10.1128/cmr.1.1.102. PMID: 3060239; PMCID: PMC358032.
- Nagashima H, Takao A, Maeda N. Abscess forming ability of streptococcus milleri group: synergistic effect with Fusobacterium nucleatum. Microbiol Immunol. 1999;43(3):207-16. doi: 10.1111/j.1348-0421.1999.tb02395.x. PMID: 10338189.
- Shinzato T, Saito A. A mechanism of pathogenicity of “Streptococcus milleri group” in pulmonary infection: synergy with an anaerobe. J Med Microbiol. 1994 Feb;40(2):118-23. doi: 10.1099/00222615-40-2-118. PMID: 8107060.
- Mukae H, Noguchi S, Naito K, Kawanami T, Yamasaki K, Fukuda K, Akata K, Fukuda Y, Kido T, Ishimoto H, Sakamoto N, Taniguchi H, Yatera K. The Importance of Obligate Anaerobes and the Streptococcus anginosus Group in Pulmonary Abscess: A Clone Library Analysis Using Bronchoalveolar Lavage Fluid. Respiration. 2016;92(2):80-9. doi: 10.1159/000447976. Epub 2016 Aug 23. PMID: 27548533.
- Bert F, Bariou-Lancelin M, Lambert-Zechovsky N. Clinical significance of bacteremia involving the “Streptococcus milleri” group: 51 cases and review. Clin Infect Dis. 1998 Aug;27(2):385-7. doi: 10.1086/514658. PMID: 9709892.
- Kobo O, Nikola S, Geffen Y, Paul M. The pyogenic potential of the different Streptococcus anginosus group bacterial species: retrospective cohort study. Epidemiol Infect. 2017 Oct;145(14):3065-3069. doi: 10.1017/S0950268817001807. Epub 2017 Aug 14. PMID: 28803566.
- Whiley RA, Beighton D, Winstanley TG, Fraser HY, Hardie JM. Streptococcus intermedius, Streptococcus constellatus, and Streptococcus anginosus (the Streptococcus milleri group): association with different body sites and clinical infections. J Clin Microbiol. 1992 Jan;30(1):243-4. doi: 10.1128/JCM.30.1.243-244.1992. PMID: 1734062; PMCID: PMC265033.
- Jiang S, Li M, Fu T, Shan F, Jiang L, Shao Z. Clinical Characteristics of Infections Caused by Streptococcus Anginosus Group. Sci Rep. 2020 Jun 3;10(1):9032. doi: 10.1038/s41598-020-65977-z. PMID: 32493976; PMCID: PMC7270121.
- Junckerstorff RK, Robinson JO, Murray RJ. Invasive Streptococcus anginosus group infection-does the species predict the outcome? Int J Infect Dis. 2014 Jan;18:38-40. doi: 10.1016/j.ijid.2013.09.003. Epub 2013 Oct 18. PMID: 24215937.
- Petti CA, Simmon KE, Bender J, Blaschke A, Webster KA, Conneely MF, Schreckenberger PC, Origitano TC, Challapalli M. Culture-Negative intracerebral abscesses in children and adolescents from Streptococcus anginosus group infection: a case series. Clin Infect Dis. 2008 May 15;46(10):1578-80. doi: 10.1086/587655. PMID: 18419492.
- Han JK, Kerschner JE. Streptococcus milleri: an organism for head and neck infections and abscess. Arch Otolaryngol Head Neck Surg. 2001 Jun;127(6):650-4. doi: 10.1001/archotol.127.6.650. PMID: 11405863.
- Siegman-Igra Y, Azmon Y, Schwartz D. Milleri group streptococcus–a stepchild in the viridans family. Eur J Clin Microbiol Infect Dis. 2012 Sep;31(9):2453-9. doi: 10.1007/s10096-012-1589-7. Epub 2012 Mar 6. PMID: 22391759.
- Sunwoo BY, Miller WT Jr. Streptococcus anginosus infections: crossing tissue planes. Chest. 2014 Oct;146(4):e121-e125. doi: 10.1378/chest.13-2791. PMID: 25288003.
- Schattner, A., Dubin, I., & Gelber, M. (2016). Double jeopardy – concurrent lung abscess and pleural empyema. QJM : monthly journal of the Association of Physicians, 109(8), 545–546. https://doi.org/10.1093/qjmed/hcw078
- Al-Saffar F, Torres-Miranda D, Ibrahim S, Shujaat A. How an Opportunistic Infection Can Mess with Your Brain and Take Your Breath Away: A Rare Case of Simultaneous Lung and Brain Abscess due to Streptococcus anginosus. Case Rep Infect Dis. 2015;2015:462459. doi: 10.1155/2015/462459. Epub 2015 Apr 1. PMID: 25922772; PMCID: PMC4397419.
- Esplin N, Stelzer JW, All S, Kumar S, Ghaffar E, Ali S. A Case of Streptococcus anginosus Brain Abscess Caused by Contiguous Spread from Sinusitis in an Immunocompetent Patient. Cureus. 2017 Oct 4;9(10):e1745. doi: 10.7759/cureus.1745. PMID: 29218260; PMCID: PMC5714405.
- Tcherveniakov P, Svennevik E, Tzafetta K, Milton R. Necrotizing fasciitis following drainage of Streptococcus milleri empyema. Interact Cardiovasc Thorac Surg. 2010 Mar;10(3):481-2. doi: 10.1510/icvts.2009.219485. Epub 2009 Dec 21. PMID: 20026487.
- Terzi HA, Demiray T, Koroglu M, Cakmak G, Hakki Ciftci I, Ozbek A, Altindis M. Intra-Abdominal Abscess and Primary Peritonitis Caused by Streptococcus anginosus. Jundishapur J Microbiol. 2016 May 17;9(6):e33863. doi: 10.5812/jjm.33863. PMID: 27630763; PMCID: PMC5011413.
