
The ACTIVE trial! This is a phase III, RCT, double blind, multicenter, non-inferiority trial comparing isavuconazole vs caspofungin in invasive candidiasis. Folks, in ID, it doesn’t get any better than this (look at all these studies!) Exclusion criteria were Candida in any body part (i.e. osteomyelitis, IE, meningitis), severe immunodeficiency, >48hrs of other antifungal therapy. The intervention was between IV isavuconazole 200mg q8h for 2 days followed by 200mg daily for at least 10 days or caspofungin 75mg once followed by 50mg daily for at least 10 days. After this, it was up to the physican to step down to either PO isavuconazole or PO voriconazole. Patients were randomized in a 1:1 ratio. Primary endpoint was overall response to therapy in the modified ITT population (defined as mycological eradication, clinical cure or improvement at the end of IV therapy within 48hrs…hmm…ok..makes sense I guess since the comparison is between Isavuconazole and caspofungin). Secondary end point was overall response at 2 weeks after end of therapy. Patients were treated for a minimum of 14 days.
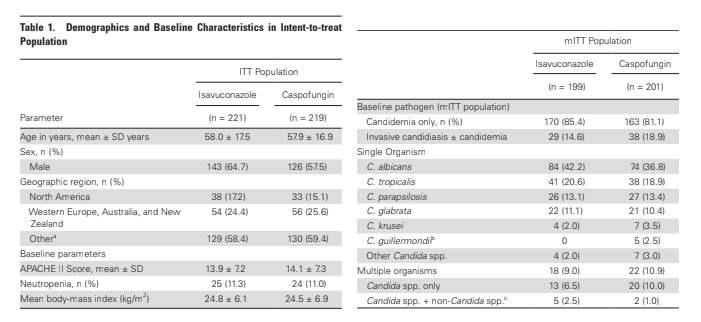
They ended up recruiting 221 patients in the isavuconazole arm and 219 in the caspofungin arm. Both groups were fairly well balanced. As were the types of Candida:
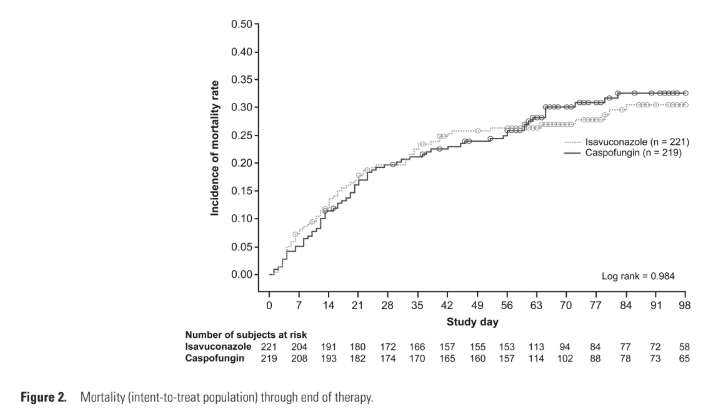
The mortality in the ITT is similar in both, but remember, the primary endpoint is response to therapy within 48hrs at the end of IV therapy for a pre-specified NONINFERIORITY…
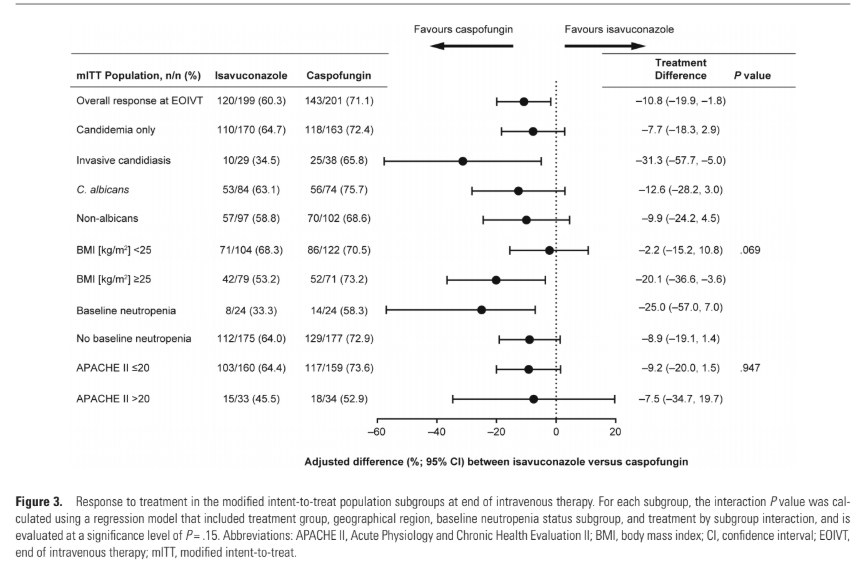
When analyzing that bit:
Both groups had similar adverse events, with roughly 5% in each group leading to discontinuation of the drug.
Lots to unpack here. I am a fan of isavuconazole because in general I do not have to worry about lots of the more common side effects you encounter with vori (and you get to cover some Mucorales spp, which is neat). I think this is further evidence that, up front, ecchinocandins are much better for Candidemia (not necessarily IE, osteo, etc) than at least isavuconazole. The end point is a bit odd; its not something I would traditionally think of as an outcome I would look at (for instance, relapse or mortality) but in this study, it makes sense since they are trying to prove non-inferiority between their azole and an echinocandin (and there is no oral echinocandin). There was no mortality difference, but remember, this study was not powered to show that. Hell, maybe there is some mortality benefit but unless there is a bigger study to prove that, we won’t know. How to interpret this data going forward, its tough to say. I do not think any of us would start someone on isavuconazole for disseminated candidemia. The other question is how do azoles play a role down the line (i.e. as step down). We use fluconazole all the time without impunity. Well, this is interesting but again, not practice changing.
